
Abstract
Over the last five years, many states have sought to limit access to Medicaid by adopting restrictive policies. How can we reconcile this development with studies that imply that Medicaid should be insulated from policy backlash? The answer lies in understanding the policy feedback effects that accompanied Medicaid expansion and how these effects created electoral pressure that led to policy modification. We situate our expectations within a policy diffusion framework that accounts for variation in both the content and timing of policy adoptions across states. We develop and test several hypotheses using survey data and an original dataset on gubernatorial support for Medicaid work requirements. Our hypotheses are generally supported and provide a more nuanced understanding of the policy feedback effects following Medicaid expansion.
The enactment of the Affordable Care Act (ACA), or Obamacare, in 2010 was undoubtedly the most significant reform of health-care policy in the United States since 1965. Although the original legislation granted state policymakers some control over implementation of the ACA, the role of state governments was significantly enhanced by the Supreme Court’s ruling in National Federation of Independent Business v. Sebelius in 2012.1 This decision effectively granted state policymakers the discretion to decide whether to expand Medicaid to a large group of low-income citizens in their state, most of whom had previously been ineligible. As a result, governors and state legislators across the country suddenly became a focal point in the debate over Medicaid expansion, governors taking center stage (Béland, Rocco, and Waddan 2016). As of late 2019, thirty-six states had either implemented or approved implementation of Medicaid expansion; fourteen had yet to initiate it (Kaiser Family Foundation 2019a).
A number of recent studies have leveraged the discretionary and uneven implementation of Medicaid expansion to better understand the politics of health-care reform. Some focus on the factors that led states to choose expansion. Consistent with studies of Medicaid policy choices prior to the passage of the ACA (Bernick and Myers 2012; Lukens 2014), these studies generally reveal that the decision to expand Medicaid was strongly related to various indicators of the state political environment, including party control of state government (Barrilleaux and Rainey 2014; Grogan and Park 2017; Jacobs and Callaghan 2013; Lanford and Quadagno 2016) public opinion (Grogan and Park 2017; Lanford and Quadagno 2016), racial resentment and racial backlash (Grogan and Park 2017; Lanford and Quadagno 2016) and state interest group pressure (Callaghan and Jacobs 2016).
More recently, scholars have turned their attention to understanding the political impact of the ACA, often through the lens of policy feedback theory. Broadly, policy feedback refers to the effect that a policy has on politics as well as future policy development (Béland 2010; Pierson 1994; Skocpol 1992). The early work on policy feedback theory focused almost exclusively on policies that guaranteed benefits to a targeted group (such as veterans or senior citizens). Such programs, scholars argue, often create a sense of entitlement that results in the development of supportive constituencies and ultimately, policy entrenchment (Campbell 2003; Mettler 2005). As Jonathan Oberlander and Kent Weaver (2015) note, positive policy feedbacks are self-reinforcing for these popular entitlement programs. Following this approach, several studies have examined the potential self-reinforcing feedback effects of the ACA through its effects on the political attitudes and behavior of program targets (Campbell 2011; Chattopadhyay 2017; Clinton and Sances 2018; Haselswerdt 2017; Hopkins and Parish 2018; Lerman and McCabe 2017). Indeed, two of the articles in this volume address such questions. Charles Courtemanche, James Marton, and Aaron Yelowitz (2020) examine the impact of the implementation of Medicaid expansion on voter mobilization. In contrast to other studies, which have found evidence of increased mobilization among Medicaid-eligible voters (Clinton and Sances 2018; Haselswerdt 2017), they find that the ACA had little impact on voter turnout. Julianna Pacheco, Jake Haselswerdt, and Jamila Michener (2020) examine the impact of ACA implementation on partisan polarization in support for the ACA. Consistent with other studies of ACA feedback effects on voter attitudes (Hopkins and Parish 2018; Lerman and McCabe 2017), they find that ACA implementation did have a significant effect on ACA support, but the direction of the effect varied based on the state partisan environment.
These studies have advanced our understanding of the political impact of health-care reform but leave a central question unanswered. If Medicaid expansion has generated positive, self-reinforcing feedback effects in states where it has been implemented, then we would expect that Medicaid would remain relatively entrenched and insulated from policy backlash. But this is not what has happened. In the wake of expansion, policymakers in many states have sought to limit access to Medicaid by adopting restrictive policies, such as Medicaid work requirements and patient copays. Supporters of work requirements have argued that such restrictions are necessary to eliminate potential work disincentives that may attract people to the program who could otherwise work and afford their own health care rather than receive a handout at taxpayers’ expense. Opponents of work requirements disagree with the premise of this argument and argue that work requirements will lead to a loss of coverage for many people and, in the end, a negative effect on public health (Ku et al. 2018). Despite these concerns, as of April 2019 fifteen states had submitted Section 1115 Medicaid Demonstration Waivers to the Trump administration requesting to implement work requirements. Seven had been approved, six were pending, and two—Kentucky and Arkansas—had their work requirements set aside by a court (Kaiser Family Foundation 2019b). How can we can reconcile this movement to roll back Medicaid with studies concluding that Medicaid expansion had positive feedback effects?
THE COMPLEXITY OF POLICY FEEDBACK EFFECTS
The answer, we argue, lies in understanding the full range of policy feedback effects that accompanied Medicaid expansion and how these effects subsequently led to electoral pressure in many states that brought about policy modification. Early on, the policy feedback literature largely devoted its attention to positive, self-reinforcing feedback effects. However, scholars have increasingly come to appreciate that policies often have negative and mixed effects, which can be “self-undermining” for a policy (Oberlander and Weaver 2015) rather than self-reinforcing (see also Campbell 2011; Patashnik and Zelizer 2013). More recent research on policy feedback theory has thus sought to identify the specific conditions that determine whether feedback effects are self-reinforcing, self-undermining, or some mix of the two (Béland 2010). Examining the impact of negative feedback is especially important to understanding the political consequences of Medicaid expansion because the debate over the ACA was highly salient and from the moment it was passed, support for Obamacare was deeply polarized along partisan and ideological lines (Mayer, Kenter, and Morris 2015; Plein 2014). It was inevitable that expansion would result in at least some backlash among conservative voters, and it is likely that these negative feedback effects have had important political consequences (Grogan and Park 2017, 2018). To understand how and where these political consequences have affected policymaking, we follow Richard Fording and Dana Patton (2019) and trace the connection between attitudes toward Medicaid expansion and the attribution of blame or reward to state policymakers deemed responsible for expansion—a process they refer to as evaluative feedback. As conceptualized, evaluative feedback thus serves as the link between attitudinal change and subsequent policy effects that have been the subject of so many studies of policy feedback.
POLICY FEEDBACK IN A DECENTRALIZED POLICY ENVIRONMENT
Because the magnitude and direction of evaluative feedback is so highly conditional on the political context, a theoretical approach that explicitly takes state variation in the political context into account is needed to properly understand the policy feedback effects of Medicaid expansion. To accomplish this, we situate our theoretical expectations regarding the effects of policy feedback within a policy diffusion framework that accounts for variation in both the content and timing of policy adoptions across states (Karch and Cravens 2014; Karch 2007). Applying this framework to Medicaid expansion, we argue that work requirements first emerged as an effort by (mostly) Republican governors in expansion states to manage negative feedback effects from Republican voters who generally opposed expansion. The adoption of work requirements has taken three forms within the diffusion process. Several states have added work requirements to their Medicaid expansion plan through processes that diffusion scholars refer to as (1) policy modification or (2) policy reinvention (Glick and Hays 1991; Clark 1985). Yet work requirements simultaneously diffused to non-expansion states that never adopted Medicaid expansion through a process we term (3) policy regression. Rather than expand Medicaid, these states seized on the opportunity provided by the introduction of work requirements into the policy stream (Kingdon 1995) to restrict a program that they felt was already too generous. As a result, Medicaid eligibility is now even more restrictive in these states than it was before passage of the ACA.
THE DIFFUSION OF POLICY FEEDBACK IN A FEDERAL SYSTEM: AN ANALYTICAL FRAMEWORK
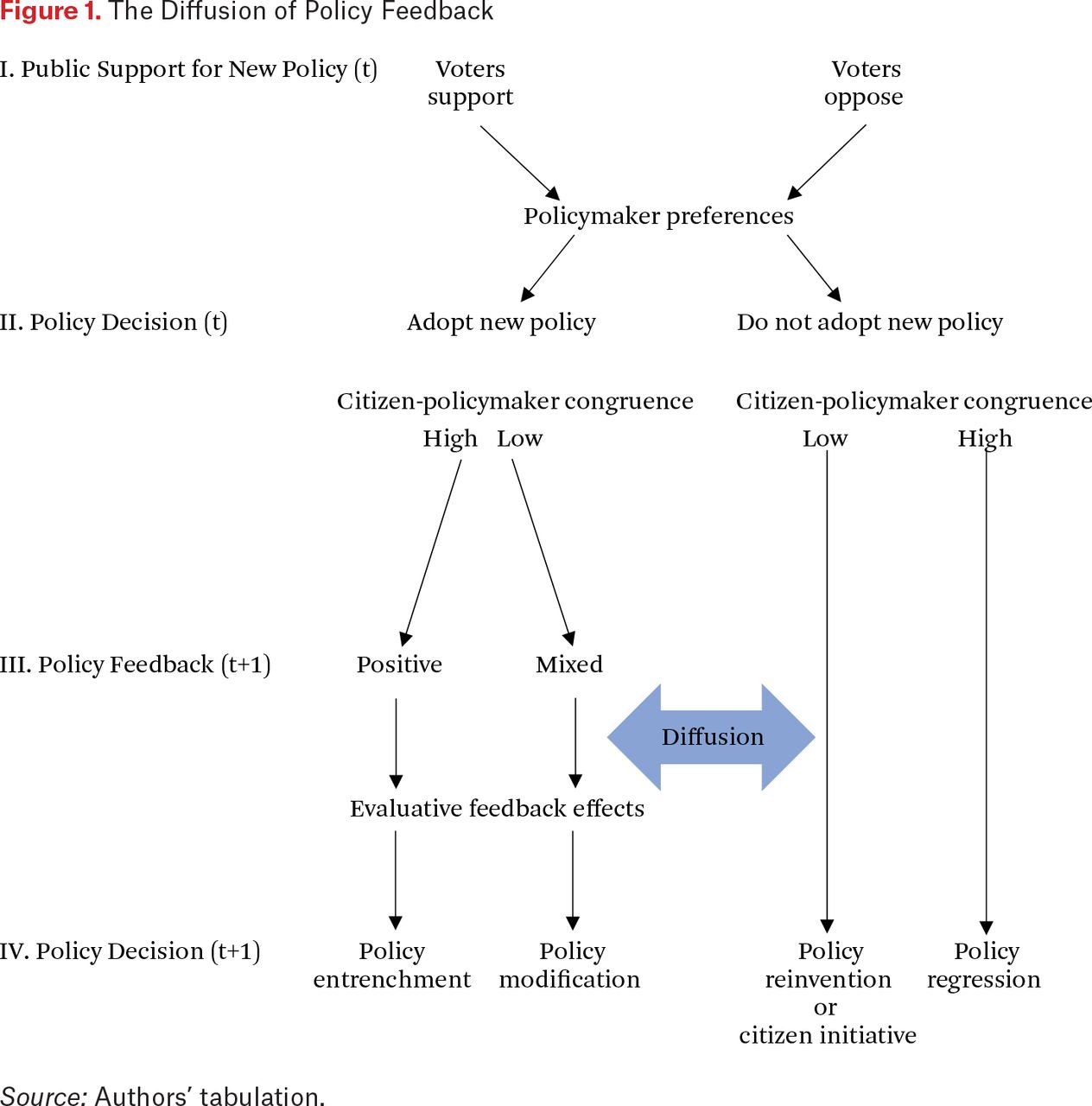
To understand the impact of Medicaid expansion on state policymaking, we develop a framework that integrates the insights of policy feedback theory with policy diffusion theory. Policy feedback theory, put most simply, asserts that policy decisions affect politics, which, in turn, affect subsequent policy decisions (Campbell 2003; Mettler 2005). Diffusion, defined by Everett Rogers (1995, 35), is “the process by which an innovation is communicated through certain channels over time among the members of a social system.” Innovation is understood to occur when a state adopts a policy that is new to the state, regardless when it was first conceived (Berry and Berry 2018). In this research, the social system we examine is the American states. Our framework attempts to account for state policy adoption and modification due to feedback effects, as well as the diffusion of policy modifications to other states. The framework is depicted in figure 1. To simplify our presentation of the logic, the figure proceeds chronologically across two periods represented as time t (stages I and II) and t+1 (stages III and IV).
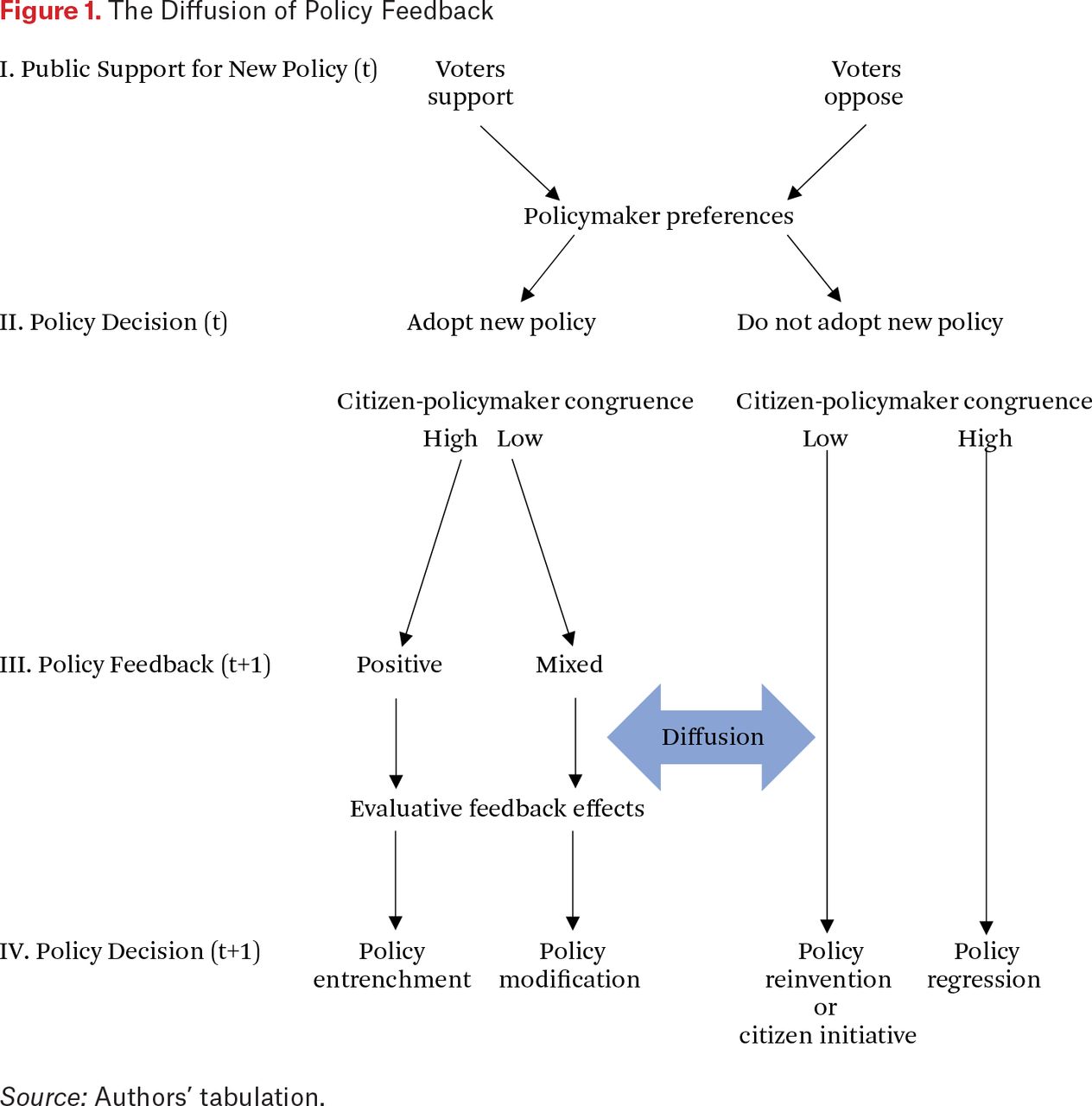
The Diffusion of Policy Feedback
Source: Authors’ tabulation.
The Initial Adoption (Stages I and II)
Stages I and II reflect the initial policy adoption decision, which takes place at time t. We assume that the initial adoption decision is largely influenced by characteristics internal to the jurisdiction (Berry and Berry 2018). Specifically, we assume that the policy is highly salient and therefore the adoption decision at time t is determined by the level of public support for the policy (stage 1), mediated by the policy preferences of state policymakers (stage 2) (Graham, Shipan, and Volden 2013). At the end of time t, state policymakers decide to either adopt or not adopt the initial policy.
What happens next, we argue, is largely determined by the political context in which the adoption decision is made. The most important dimension of the political environment, we maintain, is the level of citizen-policymaker congruence (that is, agreement) regarding the adoption decision. Although congruence is inherently a continuous variable, for the sake of simplicity we conceptualize congruence as dichotomous—congruent and incongruent. This leads to four decision environments in figure 1 based on the combination of the initial adoption decision (adopt or not adopt) and the degree of citizen-policymaker congruence regarding the decision (congruent-incongruent). We discuss each of these contexts in turn.
For most adoption decisions, the majority of states will likely fall into the congruent category given the natural alignment of citizen and policymaker preferences in a functioning representative democracy. In our framework, congruence exists in one of two forms. First, citizens and policymakers may both oppose adoption. This is the context most likely to lead a state to be a non-adopter, at least in the initial phase of the process (time t). Congruence can also occur when both citizens and policymakers support the policy. This is the context most likely to lead a state to be an “early adopter” (or innovator) (Walker 1969; Gray 1973) given that elites can pursue their preferred course of action without any risk of voter backlash.
Although a majority of states are likely to be classified as congruent, not all are given the inherent, imperfect connection between citizen and policymaker preferences in a representative democracy. Incongruence can also result when the policy under consideration will have a broad range of effects and citizens and elites disagree over which ought to be prioritized in the adoption decision. In incongruent contexts, the initial adoption decision is not an easy one because it is impossible (by definition) to satisfy the demands of both citizens and policymakers. For this reason, regardless of the adoption decision at time t, additional policymaking activity at time t+1, spurred in part by the actions of the losing side at time t, is likely.
Policy Feedback and Policy Diffusion (Stages III and IV)
Stages III and IV reflect our expectations regarding what happens after the initial adoption decision. During stage III, the political impact of the initial adoption decision is experienced through a range of policy feedback processes that are determined by the nature of citizen-policymaker congruence. These feedback effects diffuse to other adopting and non-adopting states and have a significant effect on the second round of policy decisions that occur in stage IV at time t+1. In the following section, we outline the theoretical logic that connects the initial adoption decision at time t to the decision at time t+1 for each subset of states defined by the adoption status and the specific configuration of citizen and policymaker preferences.
Early Adopters: Congruent
Early adopters that display relatively high citizen-policymaker congruence are expected to experience positive, self-reinforcing policy feedback effects that can ultimately lead to policy entrenchment and (perhaps) further expansion of the policy. This outcome is contingent on the new policy having the impact that was expected before implementation. If this is the case, opposition should be limited and the majority of citizens should reward the state policymakers responsible for adoption of the policy through positive evaluative feedback effects. As a result, policymakers should become further incentivized to protect or even expand the policy to maximize electoral security.
Early Adopters: Incongruent
The fate of early adopters characterized by low citizen-policymaker congruence is expected to be quite different. Policy feedback effects for these states are more likely to be mixed given the weaker support for the policy by either citizens or policymakers before implementation. This is expected to lead to both a strong mobilization of opposition to the policy after it is adopted and a countermobilization of supporters. The challenge for supporters is to frame the policy debate to highlight the benefits. If these do in fact materialize upon implementation it is possible that positive feedback effects may eventually demobilize enough of the opposition that policy entrenchment becomes possible. However, this outcome is less likely when attitudes toward the policy are highly polarized along partisan lines and partisan frames are highly salient in national media. In this case, opinions about the policy are most likely to be shaped by partisanship and to be resistant to change due to the phenomenon of “motivated reasoning” (Taber and Lodge 2006; Achen and Bartels 2016). One possible outcome, of course, is policy repeal. However, it is more likely that policymakers will respond first with “policy modification,” in which the new policy is revised in a way to move it closer to the preferences of the opposition in their state (Karch and Cravens 2014; Boehmke and Witmer 2004; Holyoke et al. 2009). Once a state implements a policy modification, it may also diffuse to other early adopters facing similar political challenges, especially if the modification appears to have demobilized the opposition.
Non-Adopters: Incongruent
The fate of non-adopters also depends on the extent of citizen-policymaker congruence, and the outcome at time t+1 can take different paths. This will ultimately depend, we argue, on the specific configuration of citizen and policymaker preferences regarding the initial adoption decision at time t. One common form of incongruence seen in non-adopting states is when policymakers support the policy but are hesitant to adopt in the face of low levels of citizen support for the policy in its current form. If this is the case, non-adopters may adopt a modified version of the policy through a process known as policy reinvention (Clark 1985; Glick and Hays 1991). The political dynamics operating here are similar to those of policy modification in that the process is driven by negative feedback effects. The major difference is that adoption of a modified policy is in anticipation of negative feedback effects rather than because of actual negative feedback.
It is also possible that incongruence may occur because of strong citizen support for the policy coupled with policymaker opposition. In this case, two outcomes are possible. First, if citizen demand is strong enough, policymakers may eventually acquiesce. However, they are likely to do so through a policy reinvention that results in a compromise of citizen and policymaker preferences. Second, if policymakers fail to give in to citizen demands, we may see citizens bypass the governor and legislature and use direct democracy to pass their preferred version of the policy. This second option, of course, is possible only in states that allow the citizen initiative.
Non-Adopters: Congruent
The final category of non-adopting states are states in which citizen-policymaker congruence is high because of shared opposition to the policy. State policymakers in these states chose not to adopt the new policy at time t because the new policy moves the status quo in a direction unacceptable to both citizens and policymakers. These states are unlikely to engage in policy reinvention that results in adoption of any form of the initial policy. It is possible that the process of policy modification and reinvention occurring in other states might provide these congruent states an opportunity to engage in policy modification that moves the status quo in the opposite direction of the new policy. We refer to this type of policy modification as policy regression.
APPLYING THE FRAMEWORK TO MEDICAID EXPANSION
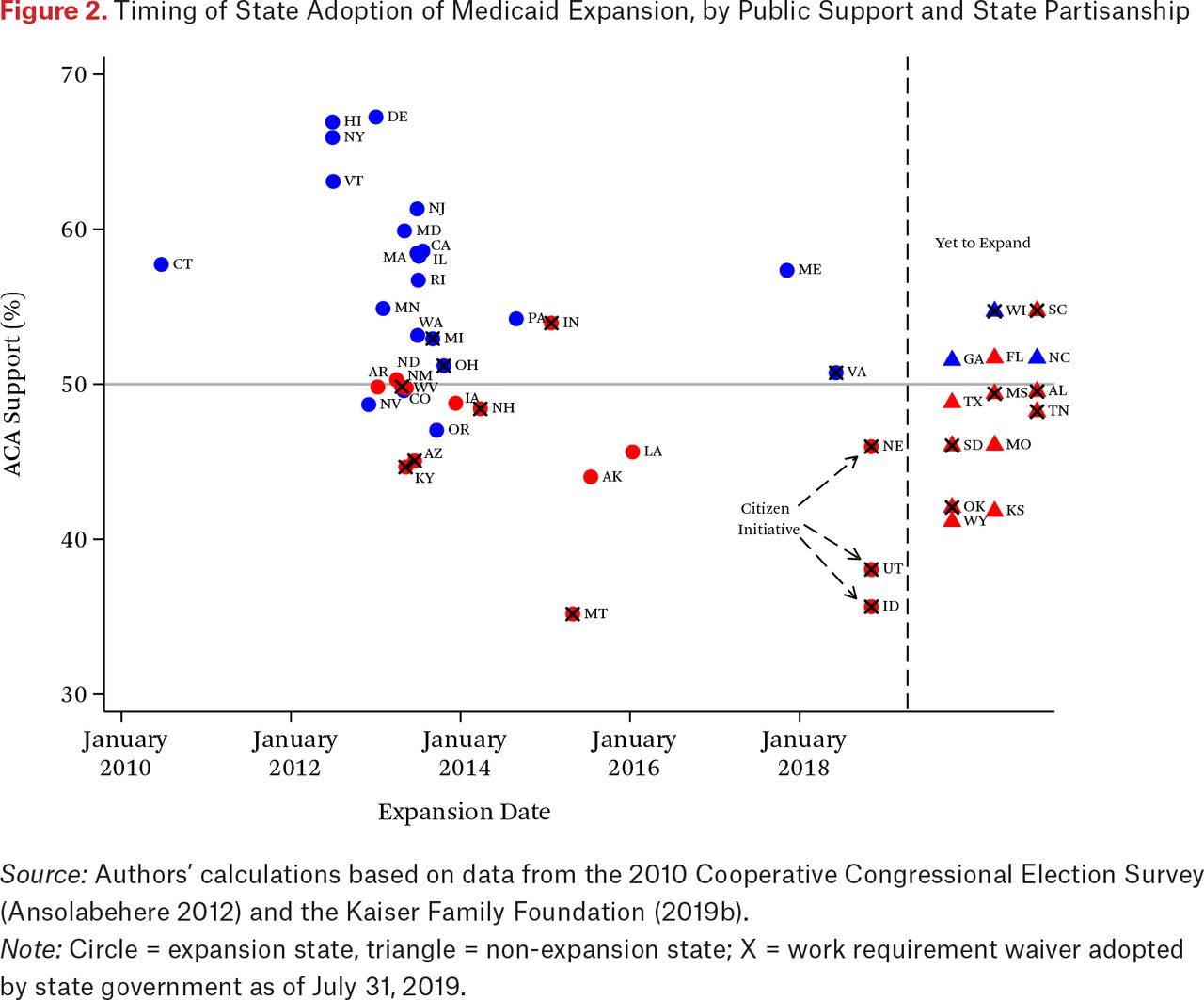
Our theoretical framework is particularly useful in understanding the adoption and subsequent policy feedback effects of Medicaid expansion as well as the diffusion of policy modifications to non-adopting states. To facilitate the application to the case of Medicaid expansion, we present figure 2, which displays a scatterplot of the timing of Medicaid expansion adoption by the average level of public support for the ACA in 2010 and 2011, mean state partisanship (measured as the strength of Republican identification), and whether a state has submitted a federal waiver to implement some type of work requirement as a condition of eligibility (as of April 30, 2019).
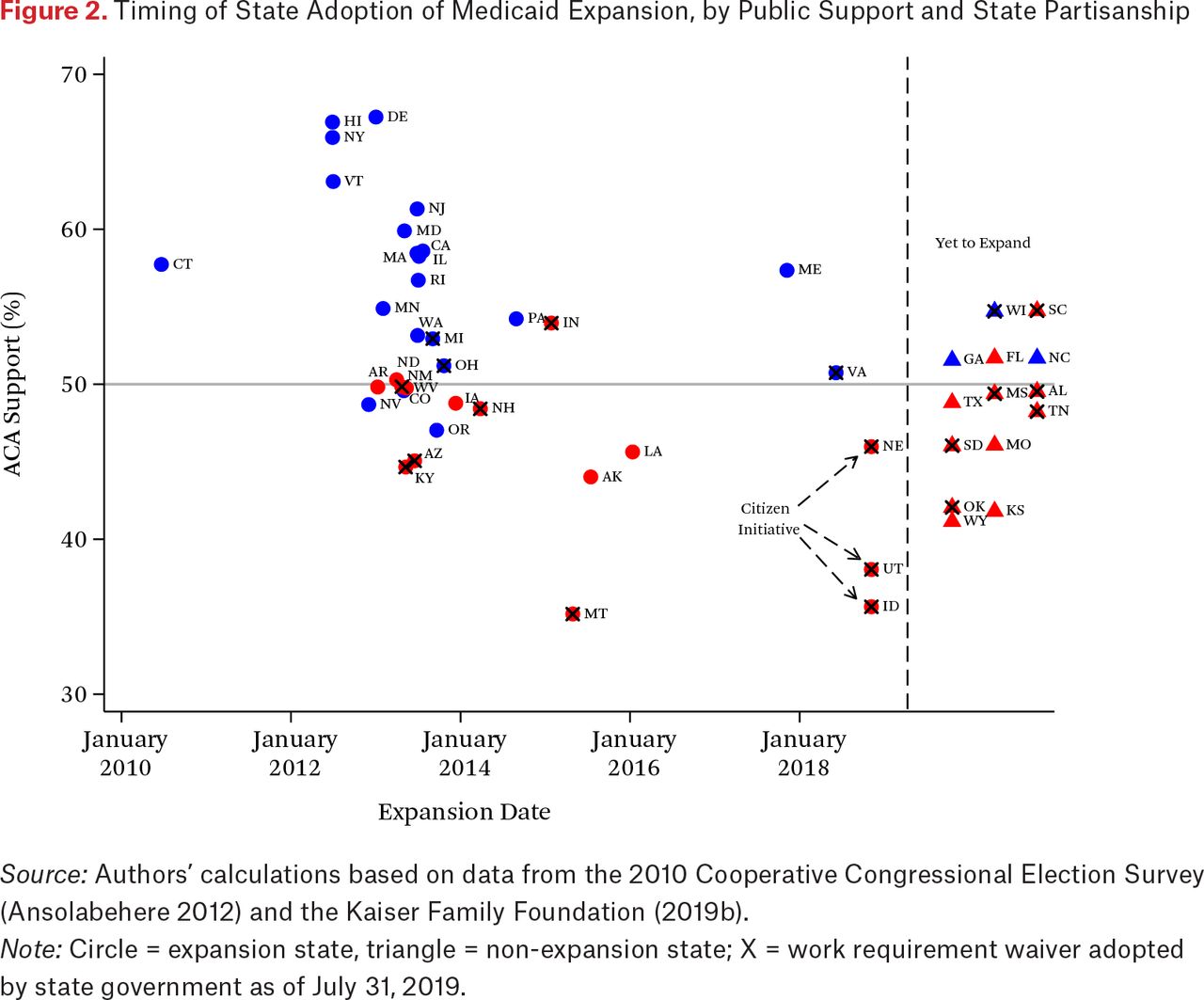
Timing of State Adoption of Medicaid Expansion, by Public Support and State Partisanship
Source: Authors’ calculations based on data from the 2010 Cooperative Congressional Election Survey (Ansolabehere 2012) and the Kaiser Family Foundation (2019b).
Note: Circle = expansion state, triangle = non-expansion state; X = work requirement waiver adopted by state government as of July 31, 2019.
THE INITIAL ADOPTION OF MEDICAID EXPANSION
As our framework suggests, we expect state policymakers in states with high levels of citizen-policymaker congruence to respond in one of two ways—as early adopters or as non-adopters—depending on the direction of support for the new policy. The pattern in figure 2 largely conforms to our expectations. The early adopters of Medicaid expansion were primarily the blue states, indicating more liberal state partisanship as well as more support for the ACA. The level of citizen-policymaker congruence is also high for the states that have not adopted expansion, (labeled “Yet to Expand” on the right side of the figure). Most of these non-adopters are “red” states and with a few exceptions, display majority opposition the ACA as we would predict.
Not all of the adopters shown in figure 2 display high citizen-policymaker congruence. Here we refer especially to the red-colored expansion states that display lower levels of support for the ACA relative to most of the blue states. Why did state policymakers adopt in these red states? Before 2016, Republican policymakers at the national level uniformly opposed Medicaid expansion, often citing ideological arguments concerning the enormous costs to taxpayers. However, for their counterparts at the state level, the decision calculus was much different. Many Republican governors undoubtedly had reservations about expansion based on traditional conservative principles, but also saw the financial benefits that expansion would bring to their state, specifically, an inflow of federal funds and the many new jobs created by the expansion of the health-care sector. Medicaid expansion also allowed the states to shift a good portion of the costs of treating the uninsured to the federal government. Because state governments must pass balanced budgets, these cost savings had the effect of potentially sparing cuts to programs that could cause political stress. These financial incentives were especially important to governors, who are generally held accountable by their citizens for the health of the economy in their state (Kousser and Phillips 2012). These fiscal incentives were clearly a factor in some solidly anti-Obama states, such as Arizona, Ohio, and Indiana, if not all of the Republican-led expansion states. For example, while leading the successful campaign to pass Medicaid expansion in Arizona, Governor Jan Brewer (R) justified her decision by claiming that expansion would protect rural and other hospitals from the rising costs of paying for uninsured patients, inject $2 billion into the state’s economy, and create thousands of jobs (Schwartz 2013). As Governor John Kasich (R) of Ohio explained, Medicaid expansion was the right thing to do because it represented “a chance to bring some Ohio money back to Ohio to do some things that frankly needed to be done” (Béland, Rocco, and Waddan 2016, 101).
The financial incentives were less important to conservative citizens for a variety of reasons. Most important, perhaps, was that the dominant opposition frame in national discourse continued to portray Medicaid expansion as welfare and, as a result, it is unlikely that conservative citizens in expansion states were persuaded that expansion was the right policy choice. Expansion in these states thus took place in a political environment of citizen-policymaker incongruence—a condition ripe for mixed policy feedback.
POLICY FEEDBACK EFFECTS AND THE DIFFUSION OF POLICY MODIFICATION
As noted, a handful of early adopters did so despite creating a potentially problematic lack of citizen-policymaker congruence. We expect that states in this category experienced a combination of positive and negative feedback effects, or mixed feedback. Mixed policy feedback results in evaluative feedback effects that may create electoral insecurity. This was especially a concern for Republican policymakers in conservative-leaning expansion states. To address this concern, Republicans in several states engaged in some form of policy modification by which they sought to limit the impact of expansion. One of the most popular policy modifications in such states has been Section 1115 waiver requests to impose work requirements for able-bodied, non-elderly Medicaid recipients as a condition of eligibility. Although a few states submitted waivers under the Barack Obama administration, they were all denied. For example, in 2015, Arizona Governor Doug Ducey (R) signed legislation that resulted in a wide range of social safety net limitations, including work requirements for Medicaid recipients and limiting Medicaid to five years. Although the Obama administration did not allow Arizona to implement the measure, the attempt undoubtedly influenced other states.
As a political strategy, the Medicaid work requirement has provided an ideal opportunity for governors to address two of the most important concerns of Republican citizens in expansion states. First, governors could frame work requirements as an attempt to rein in the potential costs of expansion. As Governor Ducey claimed, passage of the legislation that would have introduced work requirements was “necessary to protect taxpayers and education” (see table A2 of the online appendix).2 A similar logic has been used to defend the introduction of monthly premiums and copays for able-bodied adult Medicaid recipients—the beneficiaries of expansion. Indeed, several states have used both policies as a way of limiting the impact of Medicaid expansion (Arkansas, Indiana, and Kentucky, for example). Second, and perhaps most important, governors have been able to use work requirements to appeal to resentful conservatives who view Medicaid expansion as an expansion of “welfare” (Grogan, Singer, and Jones, 2017). As Arkansas Governor Asa Hutchinson (R) explained, Medicaid “is supposed to be an incentive and encouragement for people to work versus an incentive for people to just receive the government benefit and not be part of a working culture of Arkansas” (Wheaton 2015).
Requests for work requirements have increased markedly following a Trump administration letter in early January 2018 opening the door to states to request this policy modification to Medicaid. Several states initially prohibited from imposing a work requirement have since taken advantage of the new federal policy. For example, New Hampshire was an early adopter of Medicaid expansion, but as shown in figure 2 has a relatively lower level of citizen-policymaker congruence. The first attempt at work requirements in New Hampshire was made by then Governor Maggie Hassan (D) in 2016. The Obama administration denied the request, but following the Donald J. Trump administration’s change in policy, New Hampshire Republican Governor Chris Sununu’s waiver request was approved. Regarding work requirements, Sununu explained that would “allow states to control the costs of their Medicaid programs by helping more people enter the workforce” (Quinn 2018).
Soon after the idea of work requirements was introduced into the “policy stream” of potential policy modifications, it diffused to non-adopting states. Diffusion scholars have identified several mechanisms through which policy diffusion occurs, one of the most important of which is policy learning. As Frances and William Berry note (2018, 256), learning as a mechanism for policy diffusion may be due not only to the success of the policy, but also to “success . . . in achieving political goals such as winning reelection or higher office” (see also Shipan and Volden 2008; Gilardi 2010; Seljan and Weller 2011). The introduction of work requirements may have been especially important in motivating state policymakers who were attracted by the financial incentives offered by expansion, but who declined expansion during the early period because they feared the potential for negative policy feedback effects. The experiences of adopter states facing the same political difficulties may have motivated reluctant states to pursue a more restrictive version of expansion through policy reinvention.
One influential example along these lines is Indiana, where Republican Governor Mike Pence presided over a Medicaid expansion via waiver for Healthy Indiana 2.0 in 2015. Although Indiana’s request to implement work requirements was denied, the more restrictive measures included in its expansion plan was important inspiration for other state policymakers. Indeed, soon after being elected in Kentucky and inheriting his Democratic predecessor’s Medicaid expansion decision, Republican Governor Matt Bevin cited Indiana’s plan as an inspiration for what eventually became a series of restrictive policy modifications to Kentucky’s program that included work requirements.
In figure 2, we have marked states with an X if they have adopted a Medicaid work requirement at the state level as of July 31, 2019. The pattern is consistent with our theoretical expectations regarding the policy consequences of policy feedback and its relationship with the level of citizen-policymaker congruence. Our theory suggests positive policy feedback effects in early-adopting states displaying high citizen-policymaker congruence. This should lead to policy entrenchment. The evidence provided in figure 2 is consistent with this prediction. None of the early-adopting blue states have sought to roll back expansion by pursuing a work requirement. In contrast, the vast majority of work requirement waivers have come from adopting states with less citizen-policymaker congruence and therefore more (or anticipated) potentially problematic negative feedback. Some of these states (such as New Hampshire) pursued work requirements as a policy modification, and others as policy reinvention.
One of the most novel aspects of Medicaid expansion as a case study in policy diffusion is that several states have pursued work requirements but not expanded Medicaid. We refer to this process as policy regression and suggest that it is most likely in states with higher citizen-policymaker congruence in opposition to the new policy (that is, expansion). It can occur only when policy modifications can be adopted without adopting the new policy. This is true for work requirements, which can be adopted even in the absence of expansion. One interesting example is Alabama. Alabama has one of the strictest Medicaid eligibility policies in the country for adults to receive Medicaid. Non-disabled, non-elderly, childless adults are ineligible and parents or caregivers of dependent children are eligible for Medicaid only if they are at or below 18 percent of the federal poverty line. For a family of three, that equates to annual earnings of less than $3,839. Given these strict eligibility rules, few able-bodied childless adults receive Medicaid in Alabama. Yet the state has applied for a work requirement waiver. Governor Kay Ivy (R) noted that the requirement would only apply to “able-bodied” adults, the goal being to “increase efficiency and decrease costs related to Medicaid, all in an effort to be good stewards of taxpayer dollars” and said, “I look forward to future implementation of those policies” (Gore 2018).
As figure 2 makes clear, most of the non-expansion states that have adopted work requirements are like Alabama—they have high citizen-policymaker congruence in opposition to expansion. Some of these states are also similar to Alabama in that they are characterized by a high level of racial diversity (Mississippi, South Carolina, Tennessee), which has been shown to be positively related to the stringency of work requirements in other social welfare programs such as Temporary Assistance for Needy Families, or TANF (Soss, Fording, and Schram 2011). Yet this group also includes states such as South Dakota, Wisconsin, and Oklahoma, which are not considered highly diverse. We would not expect that work requirements, as a form of policy modification, would originate in non-expansion states, and indeed they have not. But the mobilization of opposition to expansion in states in which feedback effects have been mixed has created an opportunity for policymakers in states like Alabama to further restrict a program increasingly characterized as a stigmatized welfare program during the course of the health-care reform debate.
Overall, the patterns depicted in figure 2 are generally consistent with our expectations of policy entrenchment, policy modification, policy reinvention, and policy regression. However, the figure presents no evidence regarding the precise causal mechanisms at work that have led many states to begin to chip away at Medicaid expansion. Our argument relies on two central claims. First, we propose that Medicaid expansion had important evaluative feedback effects that affected citizen evaluations of state government performance. To test this proposition, we use survey data to examine the effect of Medicaid expansion on approval ratings for the governor and the state legislature. Having established the potential importance of evaluative feedback effects, we turn our attention to our second claim—that evaluative feedback effects motivated state policymakers to pursue work requirements through policy modification or reinvention. We test this hypothesis through an analysis of state-level data on the adoption of Medicaid work requirements.
MEDICAID EXPANSION AND EVALUATIVE FEEDBACK: AN EMPIRICAL ANALYSIS
For evaluative feedback effects to occur, we must assume that citizens come to some consensus regarding the political actor or actors responsible for the policy (regardless of whether their attribution of responsibility is accurate). When this happens, policy feedback effects on mass attitudes can have significant political consequence. The populations affected by the policy will presumably direct their political punishment or reward at a specific political target. The first question to grapple with, then, is whether it is plausible to expect Medicaid expansion to have an effect on evaluations of state government. Survey research has shown that in recent years, voters have regularly cited health care as an important policy problem. In the years immediately before and after the passage of the ACA, roughly a quarter of Americans believed that health care was “the most important problem facing the U.S.” (McCarthy 2017). In the years since then, the salience of health care has fluctuated but has consistently ranked among the top “problems” facing the country. Thus it is not surprising that health care continues to be on the minds of voters when casting their ballots. In the 2016 presidential election, the Kaiser Family Foundation (2016) reported that 68 percent of voters cited health care as a “major” factor in their voting decision. And in the 2018 midterm elections, this continued to be the case. Approximately three-quarters of voters cited “health care” as “very important” to them in their vote decision (Pew Research Center 2018). Thus, there is good reason to suspect that, as one of the central components of the ACA, Medicaid expansion has been and continues to be salient enough to have an impact on voter evaluations.
To the extent that voters were aware that the decision to expand Medicaid was left to state government, we expect that voter support for expansion will be taken into consideration in their evaluation of state government performance. The most likely target of blame or reward, we believe, was the governor. Many studies find that as the chief executive, voters “look to governors to lead their states, credit them with any successes and hold them accountable for most failures” (Kousser and Phillips 2012, 1). We expect this to be just as true for the decision to expand Medicaid, which is one of the most significant policy decisions made at the state level in recent years.
Despite the central role of the governor in the expansion debate, there are at least two reasons we might expect that the expansion decision would impact legislative approval as well as gubernatorial approval. Most significantly, expansion required legislative action in the majority of states and many voters may well have been aware of this fact. But perhaps a more compelling reason for why voters might attribute some responsibility for expansion to their state legislature is that they are unaware of how expansion was passed in their state. For this reason, it is likely that many voters simply attributed expansion to “state government,” without necessarily distinguishing between the legislative or executive branches. This leads to our two first testable hypotheses:
H1: Voter support (opposition) to Medicaid expansion should be positively (negatively) related to voter approval of state government institutions.
H2: The effect of voter support on institutional approval should be stronger for governors than for state legislatures.
Connecting Medicaid Expansion to Institutional Evaluations
We test these hypotheses by estimating the impact of Medicaid expansion on approval items for the governor and the state legislature utilizing the 2014 wave of the Cooperative Congressional Election Study (CCES). The CCES is desirable because the sampling design ensures large, representative samples for every state. This is critical for our analysis given the fact that one of our primary variables of interest—Medicaid expansion—varies only at the state level. The CCES is also the only large-scale survey that regularly includes items measuring approval of the governor and the state legislature. We begin by using the 2014 wave, as this is the only wave that includes an item measuring support for Medicaid expansion. Specifically, the item asks, “Should your state refuse to implement the expansion of health care for poor people, even if it costs the state federal Medicaid funds (yes or no)?” Of the approximately fifty-five thousand responses, nearly two-thirds (64.3 percent) responded no. However, reflecting the highly polarized nature of the health-care debate, responses to this question are strongly related to partisanship. Among Republicans, 57 percent responded that their state should refuse Medicaid expansion; 79 percent of Democrats responded that they should not.
To test our hypotheses, we begin with a simple test that examines the connection between one’s position regarding expansion and evaluation of their state government. The dependent variables for this analysis come from the CCES approval items, which ask respondents, “Do you approve of the way each of the following is doing their job?” Respondents are asked to rate the performance of several political leaders and institutions, including their governor and state legislature, on a scale we have recoded to range from 1 (strongly disapprove) to 5 (strongly approve). The key independent variable in our analysis is the respondent’s position on Medicaid expansion, which we code as a measure of opposition to expansion (0 = do not refuse to implement, 1 = refuse to implement). The logic of the analysis is straightforward. We estimate the effect of opposition to expansion separately for respondents in expansion and non-expansion states.3 If voters do in fact attribute blame or reward for their state’s expansion decision to their state’s governor and legislature, we should observe opposition to expansion to be positively related to approval in non-expansion states as a reward for refusing expansion. But in expansion states, the reverse should be true—opposition to expansion should be negatively related to approval.
Because voters may be influenced by a variety of policy attitudes when evaluating their political leaders, we control for several potential confounding variables. Specifically, we include preferences for state spending across four policy areas—welfare, education, law enforcement, and transportation-infrastructure. We also include measures of party identification and ideological identification, each measured on a 7-point scale and scaled as measures of Republican and conservative identification, respectively. To control for unmeasured characteristics of governors and legislatures, we include state fixed effects. Because it is well established that gubernatorial approval is related to perceptions of economic performance (Cohen and King 2004), we also control for retrospective economic evaluations. Finally, we control for respondent demographic variables (education, income, age, gender, religion, and employment status).
The results of our analysis are presented in table 1. To save space, we report only the coefficients for the variables of interest and the most important controls. The results largely conform to our expectations. In non-expansion states, opposition to Medicaid expansion is positively related to approval. For governors, the coefficient value suggests that in non-expansion states, the level of approval among those who opposed the ACA was 1.0 larger than the approval rating for otherwise similar respondents who supported expansion. This is impressive given the fact that the approval measure ranges from 1 to 5. As expected, in expansion states the relationship is reversed. In expansion states, the approval rating for governors among those who opposed the ACA was approximately 0.46 lower relative to respondents who supported the ACA. Contrary to our expectations, the effect sizes are approximately the same for the governor and the legislature.
Effect of Citizen Opposition to Medicaid Expansion on State Government Approval, 2014
That attitudes toward Medicaid expansion had such strong effects on state government evaluations even after controlling for so many measures of policy preferences is strong evidence that Medicaid expansion had significant evaluative feedback effects. This analysis is limited, however, because it relies on a cross-sectional design. We therefore provide a second test by using a longitudinal design that allows us to identify the effect of expansion based on within-state changes in approval ratings measured before and after implementation.
Medicaid Expansion and Evaluative Feedback: A Difference-in-Difference Analysis
To conduct this analysis, we use CCES data from the five federal election years from 2008 to 2016. Thus we are able to measure the level of institutional approval both before and after the announcement of the Medicaid expansion decision in each state (for the dates of these announcements, the presiding governor, and the date the state officially adopted full Medicaid expansion, see table A1). We measure Medicaid expansion as a dichotomous variable that takes on a value of 0 before expansion and a value of 1 beginning with the first survey year after the adoption date. For non-expansion states, this variable is set at 0 for the entire period.
For both governors and state legislatures, we assume that the effect of expansion is experienced only during the term of office during which the expansion decision was made. Therefore, we assign a value of 1 to the subsequent survey year if the same governor and legislature is still in office and a value of 0 to all survey years for which a new governor and legislature have replaced the policy actors responsible for expansion. Three governors led an effort to expand Medicaid but had their expansion legislation voted down in their state legislature. We code them as expansion governors for our analysis because the fight over expansion in these three states was highly salient. Voters should therefore have awarded credit or blame for their governor’s attempt to expand Medicaid even though it was unsuccessful.4 However, we code state legislatures in these states as non-expansion legislatures. Finally, in two states (Connecticut and Pennsylvania), Medicaid was expanded twice, in each case broadening eligibility. In these two states, we therefore code two periods as expansion periods. This results in a total of thirty-six governors coded as expansion governors and thirty-three legislatures coded as expansion legislatures. We are able to measure approval for at least one survey wave before and after expansion for twenty-six governors and legislatures that were in office when Medicaid expansion was adopted in their state. For the ten other cases of expansion, we are only able to observe approval for either the before or after period.
Unfortunately, we are unable to include a measure of opposition to Medicaid expansion in this analysis because this item was included only in the 2014 wave. We therefore conduct a more indirect test of the contingency of evaluative feedback effects by estimating the effect of Medicaid expansion on approval, conditional on two political measures known to be strongly correlated with attitudes toward Medicaid expansion—partisanship and ideology. These conditional effects are estimated by including two product terms to our models: Medicaid expansion*partisanship and Medicaid expansion*ideology. Because partisanship and ideology are scaled so that higher values reflect stronger conservatism, we expect the coefficients for the interaction terms to be negative. As in our first analysis, we also control for respondent age, gender, education, income, race, retrospective economic evaluations, and survey year. Finally, we include fixed effects for governors and legislative terms in our respective approval models, thus restricting identification of the expansion effect to come solely from within-term variation in a difference-in-difference framework.
The results of this analysis are presented in table 2. Our primary hypothesis predicts that the effect of Medicaid expansion on approval will be moderated by the ideology and partisanship of the respondent. Specifically, the hypothesis predicts that Medicaid expansion will cause Democrats and liberals to respond more positively to expansion than Republicans and conservatives. The results of model 2 provide support for this hypothesis. The interaction coefficients for Medicaid expansion*partisanship and Medicaid expansion*ideology are both negative and statistically significant. This is true for both models of approval—for governors as well as state legislatures.
Effect of Medicaid Expansion on Gubernatorial and Legislature Approval
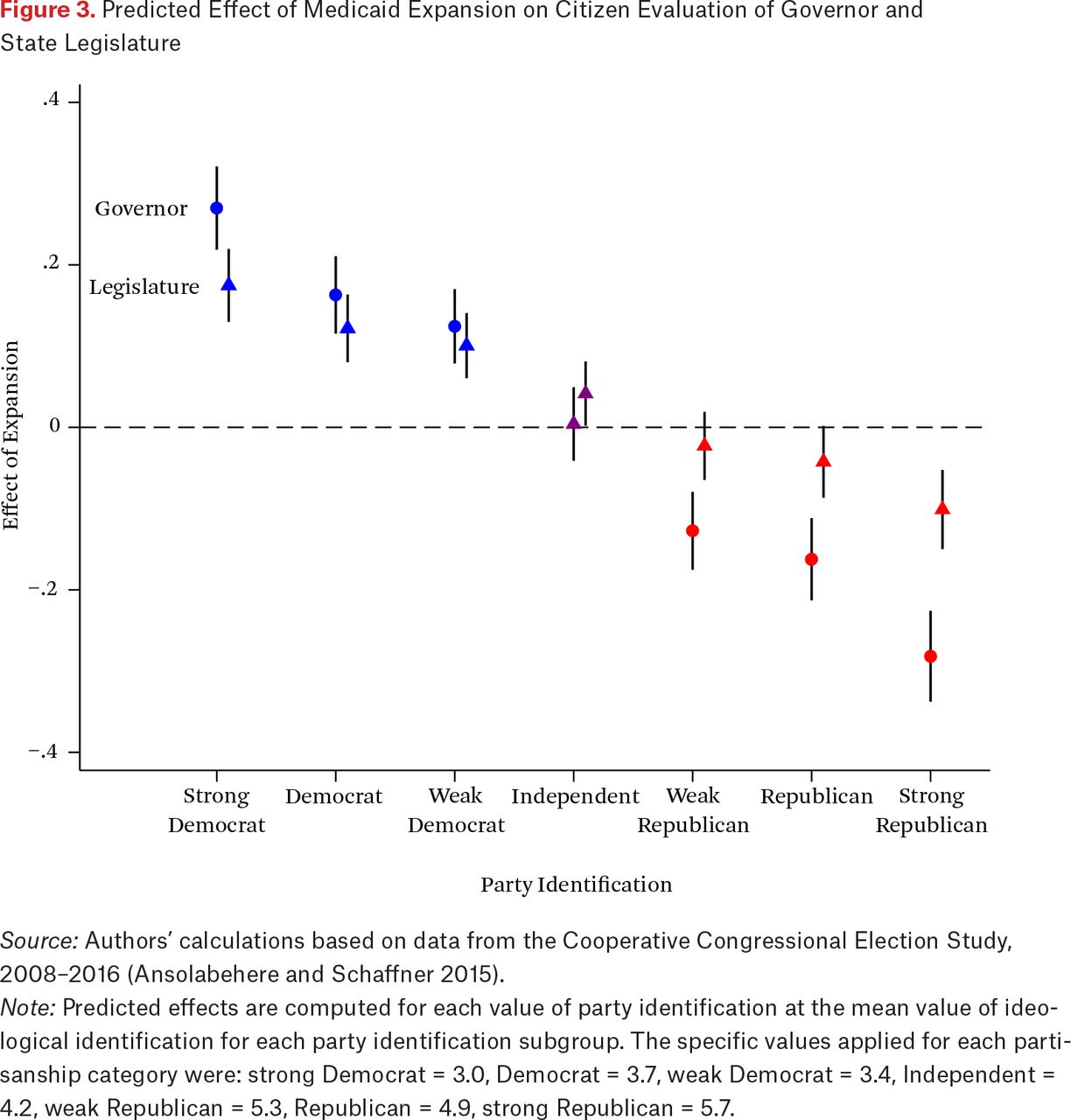
In figure 3, we present a graphical representation of the marginal effect of expansion on gubernatorial and state legislative approval across a combination of values for partisanship and ideology. For each value of partisanship (1 through 7), we computed the mean value of ideology across the entire sample. We then computed the marginal effect for each pair of partisanship and ideology values. This provides a more informative estimation of the political effects of expansion due to the fact that (as we would expect) party identification is strongly correlated with ideology (r = .68). We computed marginal effects of expansion for each political subgroup for both gubernatorial and legislative approval. This results in a set of fourteen marginal effects that provide a representative picture of the expected political implications of expansion experienced by governors and legislatures across the ideological spectrum.

Predicted Effect of Medicaid Expansion on Citizen Evaluation of Governor and State Legislature
Source: Authors’ calculations based on data from the Cooperative Congressional Election Study, 2008–2016 (Ansolabehere and Schaffner 2015).
Note: Predicted effects are computed for each value of party identification at the mean value of ideological identification for each party identification subgroup. The specific values applied for each partisanship category were: strong Democrat = 3.0, Democrat = 3.7, weak Democrat = 3.4, Independent = 4.2, weak Republican = 5.3, Republican = 4.9, strong Republican = 5.7.
The pattern of effects in figure 3 are consistent with our expectations regarding the politicized pattern of response to Medicaid expansion. Liberal Democrats responded positively to expansion and rewarded their governor and state legislature with similar bumps in approval. The Republican response was quite similar, although in the opposite direction. Republicans also punished their governor more than their legislature, providing the first evidence in support of hypothesis 2. Based on the marginal effects presented in figure 3, we see that the very strongest effects of expansion come from strong Republicans, who are predicted to experience a decrease in approval of approximately 0.30 for governors and 0.15 for legislatures. To provide some perspective on the magnitude of these effects, consider the effect of economic evaluations reported in table 2. Studies of gubernatorial approval have consistently found that evaluations of the economy have the most important effects on citizen approval ratings (Cohen and King 2004; Kousser and Phillips 2012) and indeed this is the case for our analysis as well. Our results find that the effect of expansion among strong Republicans was approximately equivalent to moving from an evaluation of much better to one of worse—a change of 3 points on the 5-point economic evaluation scale.
The figure also highlights the political dilemma that Republican governors in expansion states face. In 2018, in twelve expansion states with Republican governors the mean state Republican identification was above the fifty-state mean. The relationship between citizen preferences and policy in these states is thus to some degree incongruent. In ten of these twelve states (Iowa and North Dakota being the exceptions), the governor subsequently supported a work requirement. In contrast, seven Republican governors in office in 2018 were elected from states that had accepted Medicaid expansion and the mean Democratic identification was above the mean. Only two of these seven governors have supported a work requirement. This would seem to support our theoretical arguments regarding the importance of negative policy feedback and electoral considerations as an important motivation for policy modification, reinvention, and regression in the form of work requirements. We turn to a more rigorous test of this argument in the following section.
EVALUATIVE FEEDBACK EFFECTS AND MEDICAID WORK REQUIREMENTS
Our results suggest that Medicaid expansion has led to significant evaluative feedback effects that are likely to have important implications for state policymaking. In our final analysis, we examine the relationship between evaluative feedback effects (gubernatorial approval) and the pursuit of Medicaid work requirements. For both theoretical and practical reasons, we focus on the behavior of governors. Because governors represent the entire state, they are most likely to be responsive to our measure of statewide approval. State legislators, on the other hand, are most concerned about approval of their individual performance among constituents from their districts. As congressional scholars have repeatedly shown, constituents often offer low approval ratings for Congress as an institution while continuing to support their representative (Durr, Gilmour, and Wolbrecht 1997; Fenno 1975). As a result, connecting the behavior of state legislators to evaluative feedback effects is far less straightforward. We therefore leave this task for future research.
Measuring Gubernatorial Support for Work Requirements
Our dependent variable is a dichotomous measure of gubernatorial support for a work requirement. We measure support, rather than adoption or implementation, because support is entirely within the control of the governor, whereas adoption and implementation depend on the decisions of other policy actors. Governors’ support for work requirements was coded using Google News searches for the period from 2012 to 2019, using the governor’s name and state as well as the term “Medicaid work requirements” as search terms. The searches were independently conducted by each author to maximize accuracy.
Based on this information, we created a panel dataset using the governor-year as the unit of analysis. The dataset begins with observations for 2014, when Mike Pence (IN), Tom Corbett (PA), and Gary Herbert (UT) were the first governors to support a work requirement. We track support for work requirements for all governors through the first quarter of 2019. For each governor, work requirement support is coded as 1 beginning with the first year in which evidence of public support appears. Once a governor is coded as supporting a work requirement, they continue to be coded as supportive throughout the remainder of their time in office. Our final dataset includes observations for ninety-nine governors, thirty-three of whom supported a Medicaid work requirement at some point during their term. Of these thirty-three, twenty-nine were Republicans and four were Democrats (for the full list of governors coded as supporting work requirements, see table A2).
Work Requirements as Policy Feedback
In the previous section, we established that Medicaid expansion produced evaluative feedback effects by affecting the governor’s approval rating. We expect that these evaluative feedback effects have subsequently influenced governors’ decisions to support or not support a work requirement. Therefore we expect that support for a work requirement will be significantly related to this feedback, as communicated through the aggregate, state approval rating. We measure the governor’s approval rating at the state level by aggregating CCES data, computing the mean approval rating for each state and year of our analysis.
Given the politically polarized pattern of feedback effects seen in figure 3, we expect that public approval will affect Democratic and Republican governors differently. We expect that governors from both parties will be most concerned about feedback effects from their core supporters. Republican governors are most likely to support work requirements in the presence of sagging approval. We expect the opposite for Democratic governors, who are likely to lose support among their base due to the popularity of expansion among Democrats and liberals. We therefore test the following hypothesis:
H3: Support for Medicaid work requirements will be negatively related to approval for Republican governors and positively related to approval for Democratic governors.
We test this hypothesis by including a dichotomous variable for the party of the governor (Republican = 1, Democrat = 0), as well as an interaction term (Republican governor*approval). We expect that the coefficient for Republican governor will be positive, reflecting the stronger preference of Republicans for restricting Medicaid. However, we expect this partisan gap to be strongest when approval is relatively low, leading to the expectation that the coefficient for the interaction term should be negative.
We also control for several additional features of the state political and economic environment. To do so, we include an indicator variable measuring Republican control of the state legislature, as well as the mean level of Republican party identification, computed by aggregating CCES data for each state and year. We expect both variables to be positively related to support for work requirements. We include three variables measuring the effects of the state health-care environment—the number or hospital beds per capita, the percentage of the state’s citizens who are covered by Medicaid (based on self-reported CCES data), and a dichotomous variable taking on a value of 1 for state-years in which a state has expanded Medicaid. Given the importance of the hospital lobby in supporting Medicaid expansion, we expect that a greater density of hospitals in a state will be negatively related to any measure to restrict access to Medicaid, including work requirements. We expect the size of the Medicaid population to have a positive effect on work requirement support in response to potential concerns regarding the future impact of Medicaid on state finances. We are less certain regarding the effect of Medicaid expansion on support for work requirements. Although our theoretical model suggests that expansion should motivate some governors to pursue work requirements through policy modification or policy reinvention, governors in non-expansion states may be equally motivated to pursue work requirements for their political benefits, resulting in policy regression.
We also include measures of current state fiscal and economic health by including the annual level of state tax collections (per thousand residents), as well as the state unemployment rate. We expect that in states that benefit from robust tax collections, governors will be less likely to be concerned about affording the costs of Medicaid and will therefore be less likely to support restrictive policies such as work requirements. Because Medicaid work requirements rest on the assumption that work is readily available for all able-bodied, non-elderly low-income residents, we expect governors to be less likely to support work requirements when their state’s unemployment rate is high, because it provides evidence that contradicts the assumption. Finally, we include measures of the state racial context due to the spillover of racial attitudes into the debate over the ACA (Grogan and Park 2017; Tesler 2012), and the possibility that the negative feedback effects due to Medicaid expansion might be enhanced in the presence of a large nonwhite beneficiary population (Fording and Patton 2019).
We estimate our model using logit, including fixed effects for years and estimating robust standard errors corrected for error-clustering at the level of the governor. The results of our analysis are presented in table 3. Model 1 of table 3 reports the results for an additive specification of the model that does not include gubernatorial approval. We find that several of our hypotheses are supported. Specifically, Republican governors and governors in expansion states were significantly more likely to support work requirements. Governors were also less likely to support work requirements when they enjoyed relatively higher tax revenue per capita and when their job market was weaker than that of other states.
Determinants of Gubernatorial Support for Medicaid Work Requirements
Model 2 tests our primary hypothesis concerning the anticipated interaction of gubernatorial party and approval. The results largely support our hypothesis. The coefficient for approval is positive and statistically significant, suggesting that approval has a positive effect on support for work requirements for Democratic governors (that is, when Republican governor = 0). This suggests that the few Democratic governors who have supported work requirements may have been motivated by the desire to shore up support among Republican voters and felt electorally secure enough to risk a backlash from their base.5 However, because so few have done so, this result must be interpreted with some caution.
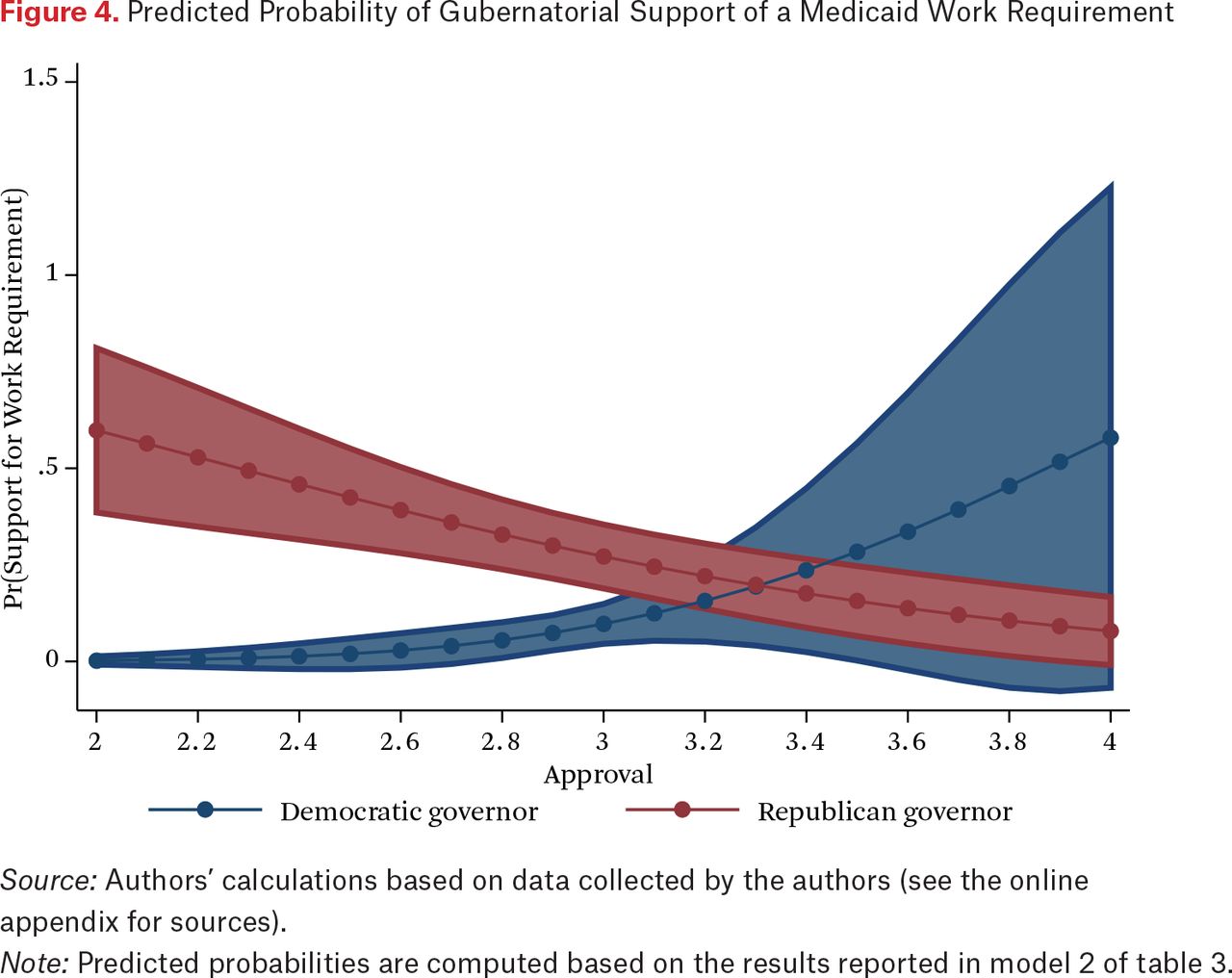
The coefficient for the interaction term is negative and statistically significant. The effect of approval is thus computed by summing the coefficient for approval and the coefficient for the interaction term, resulting in a predicted marginal effect of –2.48 (p < .01). This equates to a 0.27 increase in the probability of support, given a 1-point decrease in approval (holding other variables constant at their mean). The range of the mean approval rating in our sample is approximately 2.0, suggesting that this effect is not trivial. To provide a clearer interpretation of the substantive implications of our results, we present figure 4. The figure plots the predicted probability of support for a work requirement by the governor’s approval rating for Republican and Democratic governors (holding other variables constant at their mean). As can be seen, Republican governors were generally more likely than their Democratic counterparts to support work requirements, but this difference is predicted to be greatest in the context of relatively low approval, which presumably leads to more electoral insecurity.
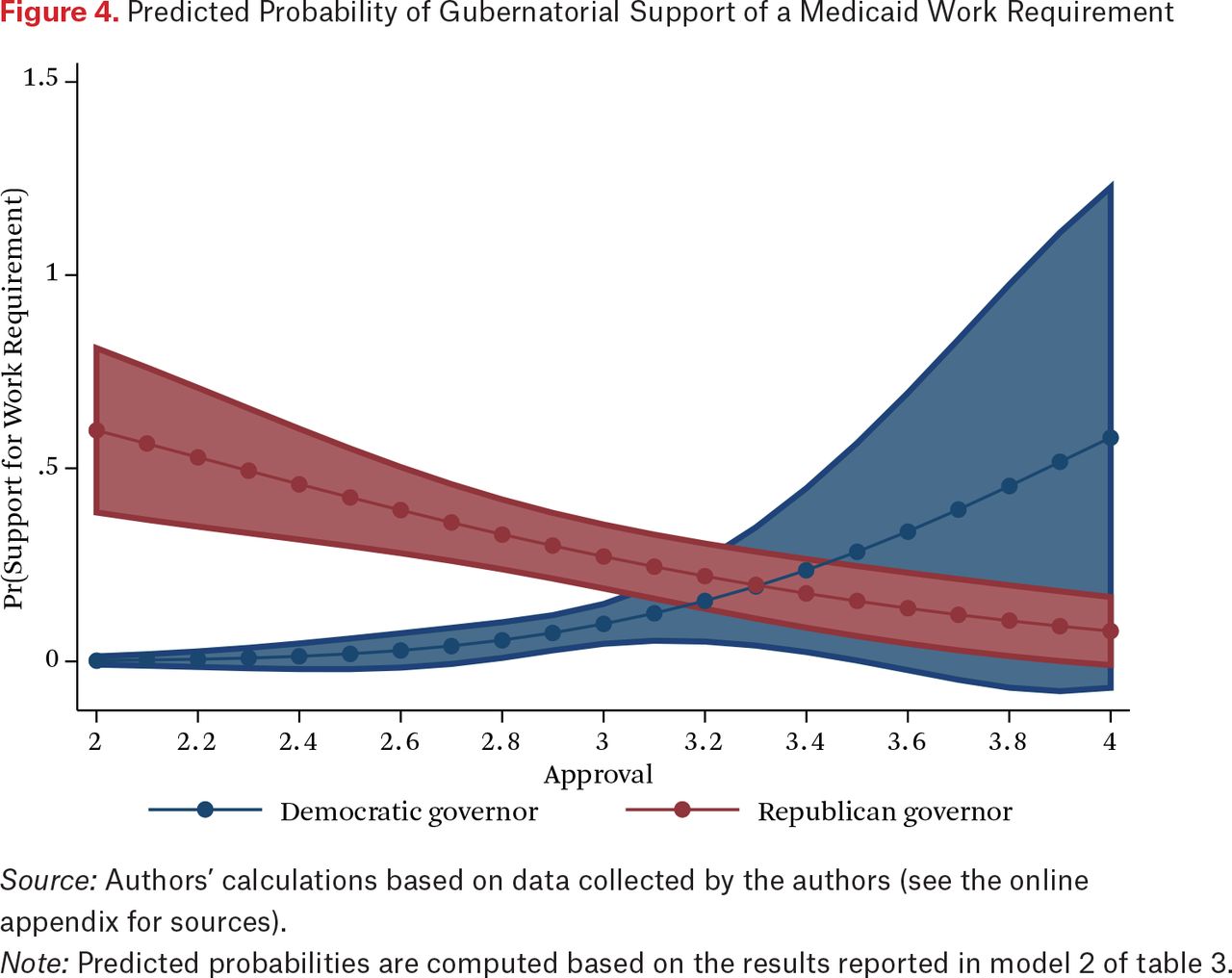
Predicted Probability of Gubernatorial Support of a Medicaid Work Requirement
Source: Authors’ calculations based on data collected by the authors (see the online appendix for sources).
Note: Predicted probabilities are computed based on the results reported in model 2 of table 3.
One possible reservation concerning the results for model 2 is the possibility that approval might be endogenous to support for a work requirement. After all, if our argument suggests that governors are motivated to pursue work requirements to improve their approval rating, we might expect that their efforts would be successful. The potential for endogeneity is limited by the fact that even though work requirement support and approval are measured in the same year, the approval data is measured using CCES data and this survey is administered late in the year—after the November election. Nevertheless, in model 3, we address this concern by including a measure of approval that is measured at a one-year lag. We lose sixty-eight observations by doing this because the lagged approval score is not available for new governors in the first year of their term. Nevertheless, the results for model 3 are highly consistent with those for model 2. Most important, we continue to find strong support for the hypothesis concerning the interaction between approval and gubernatorial party.
CONCLUSION
We began our study by posing a question. If Medicaid expansion has generated positive, self-reinforcing feedback effects, why have so many state policymakers sought to limit access to Medicaid by adopting restrictive policies? The answer, we argue, lies in an understanding of the full range of policy feedback effects that accompanied Medicaid expansion and how they are distributed across political environments. We show how these effects not only led to a process of policy modification that affected policymaking in expansion states, but also diffused to other states, ultimately contributing to unique expansion plans adopted through policy reinvention, as well as retrenchment in some non-expansion states through policy regression.
The key mechanism that drove this process, we argue, was the impact of evaluative feedback effects, which connected attitudes toward Medicaid expansion to the attribution of blame and reward for the expansion decision to state policymakers. Based on different analyses of survey data, we conclude that citizens did indeed connect their opinions of Medicaid expansion to their evaluations of institutional performance. Governors in conservative-leaning expansion states were especially likely to be the target of negative evaluative feedback effects because expansion was generally opposed by their conservative base. Finally, we find that evaluative feedback, operating through gubernatorial approval ratings, had a significant effect on governors’ support for Medicaid work requirements. Most important, approval was negatively related to work requirement support among Republican governors, consistent with the hypothesis that Republican governors were motivated to pursue work requirements as political damage control.
In many ways, Medicaid expansion presents a somewhat unique case. Given the salience of the national debate over health-care reform, state expansion decisions probably received more attention than most state policies normally receive, thus facilitating the attribution of responsibility and the possibility of evaluative feedback effects. Before the ACA, perhaps the best example of a policy issue that reached similar levels of salience and polarization was welfare reform during the 1990s. At the same time that Bill Clinton was providing national visibility to the issue by campaigning for president on a promise to “end welfare as we know it,” many governors began to pursue waivers from the federal government to implement their own brand of welfare reform. This likely led to important evaluative feedback effects for many governors, such as Tommy Thompson, who eventually parlayed his policy successes in Wisconsin to an unprecedented third term as governor.
Like TANF and food stamps, Medicaid expansion was also particularly vulnerable to negative framing by opponents due to the fact that the target population for expansion largely consists of able-bodied adults who are viewed by many Americans as less deserving of public assistance (Soss, Fording, and Schram 2011). The framing of Medicaid as welfare has therefore resonated with many Americans who continue to view welfare recipients as lazy. The “welfarization” of Medicaid in political discourse has also facilitated policy modification, reinvention, and regression given that welfare reforms already exist in the policy stream and were readily available to be adapted to Medicaid in what might be considered a form of cross-program feedback.
Finally, our results have some implications for what we might expect in the future. Some commentators viewed the failure of the Republican-controlled Congress to repeal Medicaid expansion in 2017 as evidence that expansion has become relatively entrenched. Our findings are not inconsistent with this interpretation. We tend to agree with Jacob Hacker and Paul Pierson (2018), who argue that the expectation that welfare state expansion will necessarily result in entrenchment is more tenuous now and depends on the political environment. Although they were more interested in understanding health-care reform at the national level, the contingent nature of entrenchment also applies at the state level. Our research supports this conclusion and suggests that in a decentralized, polarized policymaking environment where policy discretion is shared across levels of government, the degree of entrenchment can sometimes vary a great deal from state to state. At the national level, it appears that for now Medicaid expansion is relatively safe in the sense that given the takeover of the House by Democrats, Republicans are unlikely to have the votes needed to repeal expansion. However, as the Trump administration has become more permissive in approving state waiver applications, the door is opened to at least partial retrenchment in many states, at least in respect to the policy options that have been devolved to the states.
FOOTNOTES
↵1. National Federation of Independent Business v. Sebelius, 567 U.S. 519 (2012).
↵2. All supplemental appendix tables, designated in text with a leading A, are available via the online appendix at https://www.rsfjournal.org/content/6/2/131/tab-supplemental.
↵3. Twenty-seven states had adopted Medicaid expansion by the fall of 2014, when the CCES survey was in the field (see table A1).
↵4. These three governors were Jay Nixon (MO), Gary Herbert (UT), and Terry McAuliffe (VA) (for the results of models that do not code these governors as expansion governors, see the online appendix). We also considered an alternative coding for expansion that would reflect an additional category for governors who took a strong stand against Medicaid expansion. However, after investigating these cases, we determined that in every non-expansion state for which we could find information, the governor went on record opposing expansion.
↵5. The five Democratic governors in our dataset who came out in support of work requirements all did so after their state had expanded Medicaid during their tenure: John Hickenlooper (CO), Pete Ricketts (NE), John Bel Edwards (LA), Maggie Hassan (NH), and Ralph Northam (VA).
- © 2020 Russell Sage Foundation. Fording, Richard C., and Dana Patton. 2020. “The Affordable Care Act and the Diffusion of Policy Feedback: The Case of Medicaid Work Requirements.” RSF: The Russell Sage Foundation Journal of the Social Sciences 6(2): 131–53. DOI: 10.7758/RSF.2020.6.2.06. We thank the editors, anonymous reviewers, and conference participants for their helpful comments. Direct correspondence to: Richard C. Fording at rcfording{at}ua.edu, Department of Political Science, University of Alabama, Box 870212, Tuscaloosa, AL 35487; and Dana Patton at dana.patton{at}ua.edu, Department of Political Science, University of Alabama, Box 870212, Tuscaloosa, AL 35487.
Open Access Policy: RSF: The Russell Sage Foundation Journal of the Social Sciences is an open access journal. This article is published under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- THE COMPLEXITY OF POLICY FEEDBACK EFFECTS
- POLICY FEEDBACK IN A DECENTRALIZED POLICY ENVIRONMENT
- THE DIFFUSION OF POLICY FEEDBACK IN A FEDERAL SYSTEM: AN ANALYTICAL FRAMEWORK
- APPLYING THE FRAMEWORK TO MEDICAID EXPANSION
- THE INITIAL ADOPTION OF MEDICAID EXPANSION
- POLICY FEEDBACK EFFECTS AND THE DIFFUSION OF POLICY MODIFICATION
- MEDICAID EXPANSION AND EVALUATIVE FEEDBACK: AN EMPIRICAL ANALYSIS
- EVALUATIVE FEEDBACK EFFECTS AND MEDICAID WORK REQUIREMENTS
- CONCLUSION
- FOOTNOTES
- REFERENCES
- Figures & Data
- Additional
- Info & Metrics
- References
Related Articles
Cited By...
- No citing articles found.