
Abstract
The Patient Protection and Affordable Care Act (ACA) included new optional Medicaid home and community-based (HCBS) initiatives: the Balancing Incentive Program, the 1915(k) Community First Choice personal care benefit, and the revised 1915(i) state plan benefit. This study identifies political, economic, programmatic, and intergovernmental factors that facilitated or impeded state participation in these ACA programs. Longitudinal and cross-sectional regression analyses were used to model state adoption from 2011 to 2015. Findings indicate that political ideology, economic factors, and existing HCBS policies were the most important determinants of whether a state adopted the ACA’s HCBS opportunities. This research has implications for federal officials interested in spurring states to achieve greater rebalancing of Medicaid long-term services and supports toward HCBS.
In the United States, an estimated twelve million individuals require long-term services and supports (LTSS) (Kaye, Harrington, and La-Plante 2010; Commission on Long-Term Care 2013). Most people in need of LTSS and their families prefer to remain at home and in the community rather than receive care in a nursing home or other institutional setting. Despite this preference and federal and state government programs to increase access to noninstitutional care, progress rebalancing Medicaid-funded LTSS toward home and community-based services (HCBS) for the elderly and people with physical disabilities has been slow.
The Patient Protection and Affordable Care Act (ACA) included several initiatives that provided states with the opportunity to expand and improve Medicaid HCBS. These new optional HCBS initiatives—the Balancing Incentive Program (BIP), the 1915(k) Community First Choice (CFC) personal care benefit, and the revised 1915(i) state plan benefit—build on and extend prior efforts to rebalance LTSS. Although these programs have received limited political and public attention, states have been adopting and implementing them, which is consistent with findings in this issue that the ACA has largely proven resilient despite a concerted campaign to dismantle it (Levy, Ying, and Bagley 2020). Between 2011 and 2015, nine states enacted two or more of these new programs, twenty enacted one, and twenty-one enacted none of the ACA’s HCBS provisions.
The states that did are a diverse array—liberal and conservative, northern and southern, wealthy and poor, and supportive of and opposed to the ACA more generally. Several states that challenged the individual mandate and Medicaid insurance expansion, such as Louisiana, Mississippi, and Texas, have pursued more than one of these options. An interesting puzzle therefore exists as to the reasons various states opt in or out. Initial observation suggests that the factors that shaped state positions on the LTSS provisions may have differed from those that influenced stances on the ACA’s Medicaid expansion and exchange provisions (Jacobs and Callaghan 2013; GAO 2012). The intent of this study is to identify the factors that facilitated or impeded state participation in the ACA’s new HCBS programs.
PRIMER ON REBALANCING MEDICAID LONG-TERM SERVICES AND SUPPORTS
Medicaid is the joint state and federal health insurance program that provides health-care coverage to low-income individuals. The federal government establishes the broad regulations of the program, including comparability and statewideness, which require states to provide Medicaid services to all eligible individuals in the state. States receive federal matching revenue for Medicaid expenditures. In fiscal year 2020, the federal match rate ranges from 50 percent to nearly 77 percent based on the income level of the state. Each state has a Medicaid state plan that details its Medicaid program, including eligibility criteria, services covered, and rates of provider reimbursement (Rudowitz and Schneider 2006). To change existing Medicaid HCBS and other state plan offerings, states must submit a state plan amendment to the Centers for Medicare and Medicaid Services (CMS). In addition, states can submit 1915(c) HCBS waivers to CMS to waive specific federal requirements such as comparability and statewideness to provide home and community-based services. With 1915(c) HCBS waivers, states can target benefits to specific geographic regions or populations such as individuals with specific diagnoses. States serve individuals who require an institutional level of care, such as in a nursing facility or intermediate care facility for the developmentally disabled, through 1915(c) waivers but must demonstrate to CMS that the waiver services are a less costly alternative to institutional care. As Philip Rocco and Andrew Kelly (2020) discuss elsewhere in this issue, the federal government also permits states to conduct demonstration waivers to test new Medicaid policies or delivery systems, including in relation to HCBS. Within the bounds of federal Medicaid regulations, state governments have significant discretion in operating the program and determining the specific eligibility criteria and services offered. This flexibility not only allows states to offer Medicaid services to meet the unique needs of their populations but also contributes to substantial variation in Medicaid programs across states.
In the United States, Medicaid is the primary payer of LTSS and accounts for more than half of all related spending annually (Reaves and Musumeci 2015). In fiscal year 2016, Medicaid spent $167 billion on LTSS, approximately 30 percent of overall Medicaid spending that year (Eiken et al. 2018). Most Medicaid spending for LTSS is for older adults and persons with physical disabilities ($104 billion), followed by those with developmental disabilities ($47 billion), those with serious mental illness or serious emotional distress ($9.4 billion), and other populations ($6.7 billion).
Federal regulations require state Medicaid programs to cover nursing facility care, and institutional care was historically the prevailing option for LTSS. HCBS, though preferred by many patients and families, are almost exclusively offered by states as optional benefits—often with limited enrollment slots. Over the past several decades, however, federal and state officials have been focused on rebalancing Medicaid LTSS spending away from institutional care toward home and community-based alternatives. Medicaid LTSS rebalancing has been driven, in part, by the preferences and well-being of individuals receiving services and perceived cost savings associated with expanding HCBS (Keenan 2010; Wiener and Stevenson 1998). Medicaid HCBS rebalancing further accelerated after the 1999 U.S. Supreme Court’s decision in Olmstead v. L.C., which established disabled individuals’ right to live in the most integrated setting possible under the Americans with Disabilities Act.1
Policymakers often cite the cost-effectiveness of HCBS in support of its expansion; however, the literature is inconclusive. Even though the cost per person decreases when services are provided in the home rather than in an institution, the total budgetary cost can increase if more people are served—that is, come out of the “woodwork”—than otherwise would have been the case when expanded HCBS options are provided (Doty 2000). A large body of research suggests that HCBS programs do not result in aggregate cost savings (Weissert, Cready, and Pawelak 1988; Grabowski 2006). Other research, however, finds cost savings under certain circumstances (GAO 1994; Mollica 2009).
Due to federal and state policy changes, Medicaid spending has increasingly shifted toward HCBS, which has grown while spending on institutional care has decreased. Federal fiscal year 2013 marked the first time Medicaid HCBS spending (51 percent) exceeded spending on institutional services (49 percent) (Eiken et al. 2018). In addition, the number of individuals receiving Medicaid HCBS has increased significantly. In 2012, 3.2 million people received Medicaid HCBS services relative to 2.3 million in 2002 (Ng et al. 2015). However, Medicaid LTSS rebalancing remains uneven across different populations and across states. In general, states have achieved greater rebalancing for individuals with intellectual disabilities or developmental disabilities (ID-DD) than for the elderly or individuals with physical disabilities (Eiken et al. 2018), and some states have achieved significantly more rebalancing than others. In 2016, the percentage of state Medicaid LTSS spending on noninstitutional care relative to institutional care ranged from 27 percent in Mississippi to more than 80 percent in Oregon.
The substantial cross-state variation in LTSS rebalancing is partly attributable to the optional nature of most Medicaid HCBS programs. Given how few federal mandates relate to the provision of HCBS, most HCBS decision making occurs at the state level. This devolution contributes to disparities in access to HCBS that can have serious implications for individuals. Previous research and government publications have noted considerable cross-state differences in HCBS offerings (Coleman 1996; GAO 2002; Harrington et al. 2009; Woodcock et al. 2011; Houser, Fox-Gage, and Ujvari 2012; Ng et al. 2015). A 2013 report from the U.S. Senate Committee on Health, Education, Labor, and Pensions bemoaned cross-state disparities in HCBS (2013).
Prior to the Affordable Care Act, states primarily provided Medicaid-funded HCBS through three mechanisms: home health state plan services, personal care state plan services, and 1915(c) HCBS waivers. All states are required to provide Medicaid home health state plan services; personal care state plan services are optional. Home health state plan services include nursing, home health aides, and medical equipment; personal care state plan services include assistance with tasks necessary to live independently, such as activities of daily living (ADLs) (eating, toileting, dressing, bathing) and instrumental activities of daily living (IADLs) (cleaning, shopping, meal preparation, money management). 1915(c) HCBS waivers are also optional and have driven much of the LTSS rebalancing over the past decade.
The Omnibus Budget Reconciliation Act of 1981 added Section 1915 to the Social Security Act, allowing states to waive Medicaid requirements for comparability and statewideness. Using this waiver, states could provide HCBS to specific populations such as the elderly or developmentally disabled, and could choose to provide services to certain regions within the state. Section 1915(c) in particular gives states the option of providing home and community-based services to individuals who meet the eligibility requirements for institutional care. Use of these waivers proved popular: in 2001, waiver spending was $14.3 billion; in 2016, it more than tripled to $48.3 billion (Ng et al. 2015; Eiken et al. 2018).
The ACA sought to further promote rebalancing within Medicaid LTSS. BIP, CFC, and the 1915(i) benefit provide additional opportunities to expand HCBS. Although none of these programs are mandatory, state officials have the option of adopting them as part of their Medicaid offerings. The goal of BIP was to further rebalance LTSS spending and improve access and quality of Medicaid HCBS across states. BIP was a time-limited program through federal fiscal year 2015 open to states with less than 50 percent of Medicaid LTSS spending on noninstitutional care. States could apply for BIP between 2011 and 2014, and thirty-eight states were eligible for BIP based on the requirement. Participating states with less than 50 percent LTSS spending on HCBS had to achieve the 50 percent benchmark by September 30, 2015, and states with less than 25 percent had to achieve the 25 percent benchmark in the same period. In return, states initially at less than 50 percent HCBS spending received an additional 2 percent federal match on noninstitutional Medicaid HCBS spending, and states at less than 25 percent received an additional 5 percent federal match through September 30, 2015. Participating states were also required to implement a No Wrong Door–Single Entry Point system to streamline access to LTSS by providing information and assistance, ensure a system of conflict-free case management, and collect core data elements when conducting functional assessments for services. Of the thirty-eight eligible states, twenty-one pursued this program (CMS n.d.a).
The second HCBS initiative is the Community First Choice 1915(k) state plan option that allows states to provide home and community-based attendant services. A key benefit for states in adopting this option is an additional 6 percent federal match rate for these expenditures. Under the benefit, states may provide more extensive services with a greater emphasis on participant self-direction than existing Medicaid HCBS (GAO 2012). CFC’s comprehensive services include assistance with ADLs, IADLs, health-related tasks, and back-up systems such as medical alert buttons. To receive these services, an individual must be at an institutional level of care and have an income at or less than 150 percent of the federal poverty level. Individuals with a higher income level are eligible for CFC if they are receiving waiver services. Unlike 1915(c) waivers, states cannot target specific populations or regions of the state with CFC. All states were eligible for CFC and could apply for the program beginning in 2011. Between 2011 and 2015, eight states pursued this option (CMS n.d.b).
The ACA also revised the existing 1915(i) state plan benefit—first enacted in the Deficit Reduction Act of 2005—to make it more attractive for states. The 1915(i) option differs from 1915(c) waivers in that individuals receiving these services do not need to be clinically eligible for institutional care, states do not have to achieve cost neutrality, and the benefit has to be available in all regions of the state. Similar to 1915(c) waivers, the 1915(i) benefit allows states to target specific populations such as the elderly, individuals with serious mental health conditions, or individuals with developmental disabilities. Only a handful of states adopted the 1915(i) state plan benefit before the ACA because states could not target services to specific populations, could only serve individuals with income at or below 150 percent of the federal poverty level, and could offer fewer services than available through 1915(c) waivers (CMS 2014). The ACA revised the 1915(i) state plan benefit so that states have the flexibility of targeting specific populations, determining a wide array of available services, and establishing more lenient financial eligibility criteria (GAO 2012). Thus the 1915(i) offers an expansion of HCBS in allowing states to provide services to individuals with less stringent functional eligibility standards than 1915(c) waivers. Thirteen states adopted this option between 2010 and 2015 after the changes in the ACA went into effect (CMS n.d.b).
The states that have pursued the ACA HCBS opportunities are diverse and represent different geographic regions of the country (see table 1). Only three states—Connecticut, Maryland, and Texas—adopted all three of these policies. Adopting states differed in their political ideology, economic climate, existing HCBS and LTSS policies, and LTSS demand and supply. In addition, some states strongly opposed to the health insurance aspects of the ACA pursued these opportunities, which suggests that state decision-making processes around HCBS programs may differ from Medicaid eligibility policies. First, HCBS programs generally benefit elders or individuals with developmental disabilities, whereas Medicaid expansion largely benefits low-income adults. The social construction of groups can influence whether a population is considered positively or negatively constructed and shape policymaking (Schneider and Ingram 1993). In contrast to older adults and individuals with disabilities, expanded Medicaid eligibility for low-income working adults apparently contributed to policy backlash in some states due to the comparatively negative social construction of those groups (Fording and Patton 2020). Second, these policies are largely focused on providing or enhancing HCBS options for those who are already eligible for Medicaid. Third, research suggests that some aspects of Medicaid policymaking, such as optional benefits, are generally not politically salient issues and are often determined by state bureaucrats, leaving governors and state legislators to focus more on overall program spending and eligibility policies (Schneider and Jacoby 1996). Last, whereas the health insurance aspects of the ACA receive substantial attention in the media and among the general public, LTSS policies receive far less. Public opinion surveys suggest that many Americans know little about LTSS or the role that Medicaid plays, and incorrectly believe that Medicare will pay for LTSS (Khatutsky et al. 2016; AP-NORC 2016). Because this issue receives far less attention from the general public, the factors influencing HCBS policy may be different from other Medicaid eligibility policies. For these reasons, this study sought to uncover the factors that contribute to states’ adoption of optional HCBS programs within the ACA.
State Adoption of ACA Policies (as of 2015)
HYPOTHESES
Existing research has identified numerous factors that may contribute to variation in state policy adoption of the ACA’s HCBS opportunities. This literature recognizes that public policies can be shaped by internal state factors, such as political, socioeconomic, and programmatic conditions (Berry and Berry 1990; E. Miller 2005). It also recognizes that the decisions of other states may shape state decision making in this area.
Political Factors
The political party in control of state government may influence a state’s pursuit of new Medicaid HCBS opportunities. Republican governors have been leading the fight challenging the ACA’s health insurance provisions, and they may also be opposed to the HCBS provisions because of the association with the controversial health insurance legislation (Republican Governors Association 2011). In contrast, research has found that states with Democratic governors spend more on Medicaid and are more likely to adopt 1915(c) HCBS waiver programs (Schneider 1993; Nelson 2007; N. Miller et al. 2008). In adopting optional Medicaid HCBS benefits, evidence also suggests that elected officials’ political liberalism, as measured by senators’ voting records, is associated with a greater likelihood of offering the state plan personal care benefit (Kitchener et al. 2007). States with unified Democratic government may be especially likely to adopt the ACA’s HCBS provision, given greater consensus and fewer roadblocks when the same party holds the governorship and legislature (Berry and Berry 1990). This may also be the case because unified government tends to produce more policy and be more responsive to the public, whereas divided government may limit innovative and significant legislation (Kelly 1993; Edwards, Barrett, and Peake 1997; Binder 1999; Coleman 1999).
Hypothesis 1: States with more liberal elected officials should be more likely to adopt the ACA’s HCBS provisions, all else equal.
Hypothesis 2: States with Democratic control of the state should be more likely to adopt the ACA’s HCBS provisions, all else equal.
Institutional capacities of the bureaucracy, legislature, and governor to govern may also impede or facilitate the adoption of new HCBS policies. In particular, bureaucratic capacity, legislative professionalism, and gubernatorial power may play a role in state HCBS policymaking. States that lack the bureaucratic capacity and knowledge to research new HCBS opportunities, develop a Medicaid state plan amendment, and operate a new HCBS program may be less likely to pursue the ACA’s HCBS expansion opportunities. Indeed, this was the key conclusion of a GAO report examining state decisions around the ACA’s HCBS opportunities: limited staff resources posed an impediment to implementing the new HCBS options (GAO 2012).
Hypothesis 3: States with more capable bureaucracies should be more likely to adopt the ACA’s HCBS provisions, all else equal.
In some states, the state legislature has taken an active role in determining whether the state pursues aspects of the ACA by passing laws or constitutional amendments opting in or out of various parts of the legislation (National Conference of State Legislatures 2017a). Research also suggests that states with professional legislatures are better positioned to adopt new policies, more likely to adopt policies earlier, and more likely to enact generous social welfare policies than states with less professional legislatures (Walker 1969; Hayes 1996; Rom 2014). In addition, the governor may be influential in determining which opportunities to pursue. Charles Barrilleaux and Michael Berkman (2003) conclude that governors with stronger institutional budgetary power are better able to influence state policy. Similarly, Barrilleaux (1999) finds that states with stronger governors tend to pursue more liberal public policies. The extent of gubernatorial influence on public policy likely varies across states and may depend on the governor’s overall power (Woods 2004; Barrilleaux 1999).
Hypothesis 4: States with more professional legislatures should be more likely to adopt the ACA HCBS provisions, all else equal.
Hypothesis 5: States with institutionally stronger governorships should be more likely to adopt the ACA’s HCBS provisions, all else equal.
Both provider lobbies and consumer advocates have an interest in Medicaid policy (Kronebusch 1997). Within LTSS policymaking, the nursing facility lobby is less supportive of expanding HCBS than other LTSS providers. In a survey of individuals involved in LTSS policy, 80.1 percent of community-based providers (including home care, hospice, and assisted living providers) supported rebalancing versus only 45.7 percent of nursing home providers (E. Miller, Mor, and Clark 2009). During the 1990s, the growth of the for-profit nursing facility industry created an influential lobbying block with interests in protecting its financial stake (Kitchener and Harrington 2004). Nursing facilities depend heavily on public funding and nursing facility executives therefore meet regularly with state officials, contribute to state political campaigns, and hire lobbyists (Wiener and Stevenson 1998). Consequently, strong nursing facility lobbies that oppose expanding HCBS programs may be well positioned to influence state decision making. In contrast, HCBS providers are more supportive of increasing home care services (E. Miller, Mor, and Clark 2009). Studies suggest that more certified home health agencies per capita within a state are associated with more waiver participants and higher waiver spending per capita (N. Miller et al. 2006).
Hypothesis 6: States with stronger nursing home lobbies should be less likely to adopt the ACA’s HCBS provisions, all else equal.
Hypothesis 7: States with stronger HCBS provider lobbies should be more likely to adopt the ACA HCBS provisions, all else equal.
In addition to provider lobbies, consumer advocates representing elders or persons with disabilities may shape state LTSS policy. Advocates representing elders and disabled individuals strongly support rebalancing. In a survey of LTSS specialists, 92 percent of consumer advocates indicated that the LTSS system should be rebalanced away from institutions to HCBS (Grabowski et al. 2010). Elder interest groups are often considered among the more influential groups because of their size and voting power (Day 2017). The significant LTSS rebalancing that has occurred over the last several decades for individuals with developmental disabilities was largely driven by consumer advocacy efforts, including self-advocacy and family members (Braddock 1992).
Hypothesis 8: States with stronger consumer advocacy groups should be more likely to adopt the ACA’s HCBS provisions, all else equal.
Economic Factors
Because Medicaid is a joint federal-state program, states with greater fiscal capacity and health are often better positioned to fund the state portion of Medicaid expenditures. The literature on Medicaid and HCBS spending suggests that state wealth or fiscal capacity is an important determinant in policymaking (N. Miller et al. 2001; N. Miller, Harrington, and Goldstein 2002; Kitchener, Carrillo, and Harrington 2004; E. Miller et al. 2005). In addition, a state’s ability to adopt a new policy may be shaped not only by the level of wealth but also by the prevailing fiscal climate. During periods of economic downturn, states often encounter declining revenues at the same time that demand for public benefits rises (Rom 2014); specifically, higher unemployment leads to more individuals eligible for welfare and Medicaid benefits as the size of the tax base declines. In 2012, the GAO published a preliminary study about states’ decisions to pursue the ACA’s HCBS opportunities, concluding that ongoing fiscal challenges and budget concerns were factors in most states’ decision-making processes (GAO 2012).
Hypothesis 9: States with stronger fiscal capacity should be more likely to adopt the ACA’s HCBS provisions, all else equal.
Hypothesis 10: States with stronger fiscal health should be more likely to adopt the ACA’s HCBS provisions, all else equal.
Programmatic Factors
Existing policies can shape the development of future policies. Within Medicaid policymaking, several studies have found that previous policymaking is crucial in understanding the adoption of later policies. Shad Satterthwaite (2002) finds that states with a policy legacy of managed care are more likely to adopt managed care programs for the Medicaid program. In respect to the ACA, states that had already implemented Medicaid policies expanding coverage to optional groups were more likely to adopt aspects of the ACA’s health insurance provisions (Jacobs and Callaghan 2013). States that already provide robust HCBS programs may be more likely to adopt new programs because of stronger prior commitments to providing LTSS in the community as opposed to an institutional setting. In addition, states may perceive the ACA’s state plan options as providing new opportunities to substitute existing services. Some states may be offering state-funded HCBS programs and have budgetary motivations to adopt these new options if the opportunity exists for additional federal funding.
Hypothesis 11: States that adopted the Medicaid health insurance expansion should be more likely to adopt the ACA’s HCBS options, all else equal.
Hypothesis 12: States with more HCBS programs should be more likely to adopt the ACA’s HCBS options, all else equal.
Decisions to adopt the ACA’s HCBS options may also be shaped by efforts to control LTSS costs. LTSS spending is an increasing portion of state Medicaid budgets, and states pursue several approaches to constrain costs. One method is limiting the supply of LTSS through nursing facility or home health agency certificate-of-need (CON) programs. Such programs limit the supply of nursing facilities or home health agencies by requiring approval for new entities or the expansion of existing entities. Nursing facility CON programs may suggest a commitment to rebalancing, whereas home health agency CON programs may indicate a state is less committed to increasing HCBS. Research suggests that states with nursing facility certificate-of-need programs invest more in HCBS while states with home health agency CON programs devote relatively less LTSS spending to 1915(c) waivers (N. Miller, Ramsland, and Harrington 1999; N. Miller et al. 2001). The decision to adopt these HCBS policies in an effort to control LTSS costs may also be influenced by a state’s Medicaid eligibility rules. States with more liberal eligibility standards may have greater financial incentive to adopt HCBS policies as cost containment measures due to higher spending. Research suggests that states with more generous Medicaid eligibility may face greater pressure to constrain expenditures (Harrington et al. 2000; E. Miller and Wang 2009).
Hypothesis 13: States with nursing home certificate-of-need policies should be more likely to adopt the ACA’s HCBS options, all else equal.
Hypothesis 14: States with HCBS certificate-of-need policies should be less likely to adopt the ACA’s HCBS options, all else equal.
Hypothesis 15: States with more generous Medicaid eligibility requirements should be more likely to adopt the ACA’s HCBS options, all else equal.
Policy Diffusion from Other States
A state’s experience adopting the ACA’s HCBS provisions may be influenced by other states’ actions in this area. Because the ACA’s programs are primarily new HCBS options, states may be reluctant to adopt them initially out of concerns about unintended consequences, such as over-enrollment or expenditures exceeding estimates. These concerns can be mitigated by observing the successful adoption and implementation of programs in nearby states (Walker 1969), which often are close geographically, have a similar political climate, and are in similar economic circumstances. Research suggests that state policy adoption is affected by neighboring state policies (E. Miller 2005, 2006; Berry and Berry 1990).
Hypothesis 16: States with a higher proportion of neighboring states adopting the ACA’s HCBS options should be more likely to adopt the ACA’s HCBS options themselves, all else equal.
METHODS
This research used panel and cross-sectional datasets to model state adoption of the three ACA HCBS policies. The cross-sectional model enabled the identification of factors predictive of adoption of any one of the ACA HCBS policies by the end of the study period. By contrast, the panel analysis examined state adoption decisions across each year of the observation period. Consistent findings across the two approaches would increase confidence in the conclusions with respect to the factors posited to influence state adoption of the ACA HCBS provisions.
In the longitudinal model, the dependent variable was a dummy variable indicating whether a state adopted any one of the three ACA HCBS programs within a given year. In the cross-sectional model, the dependent variable was again a dummy variable, this time indicating whether the state had adopted any of the ACA HCBS policies as of December 31, 2015. The explanatory variables in both models were factors posited to be associated with state policymaking based on the hypotheses. These included measures of state government ideology (Democratic control, liberal elected officials’ ideology), governing capacity (gubernatorial power, legislative professionalism, administrative capacity), industry and consumer advocacy power (using supply and demand side proxies), fiscal capacity, fiscal health, other Medicaid HCBS and LTSS policies (services, spending, programs), and prior neighboring state adoptions. Both models were estimated with Stata 15.
Dependent Variables
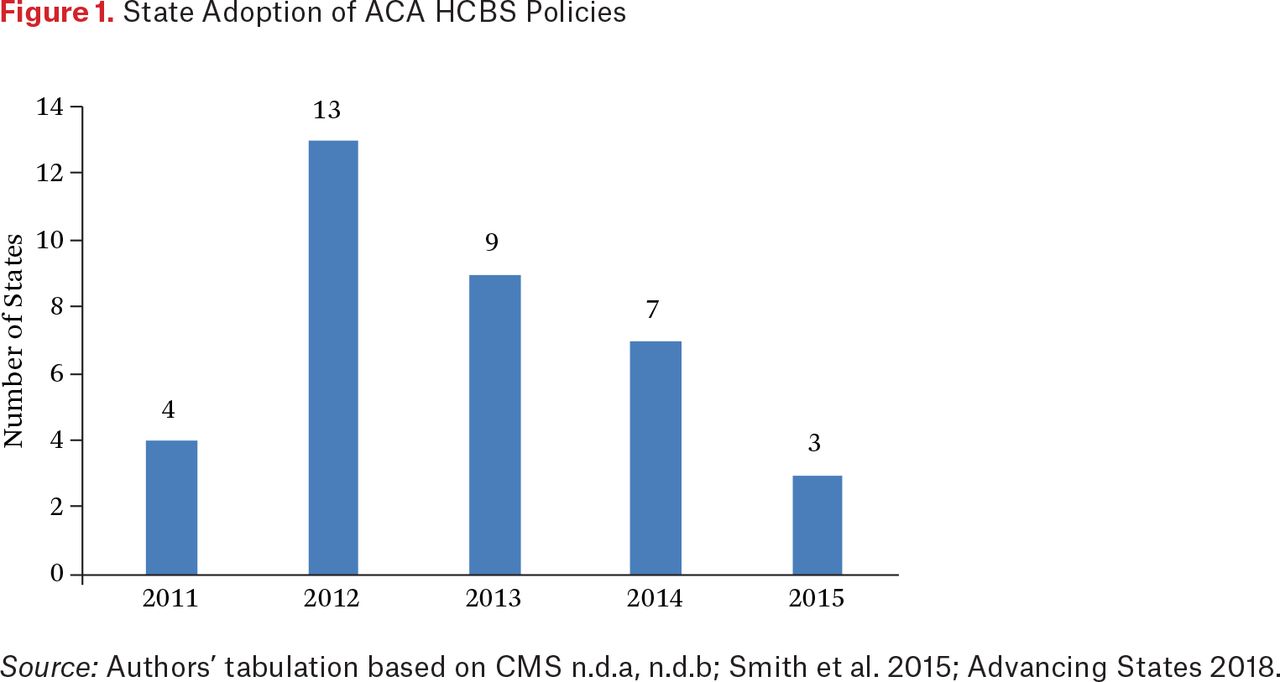
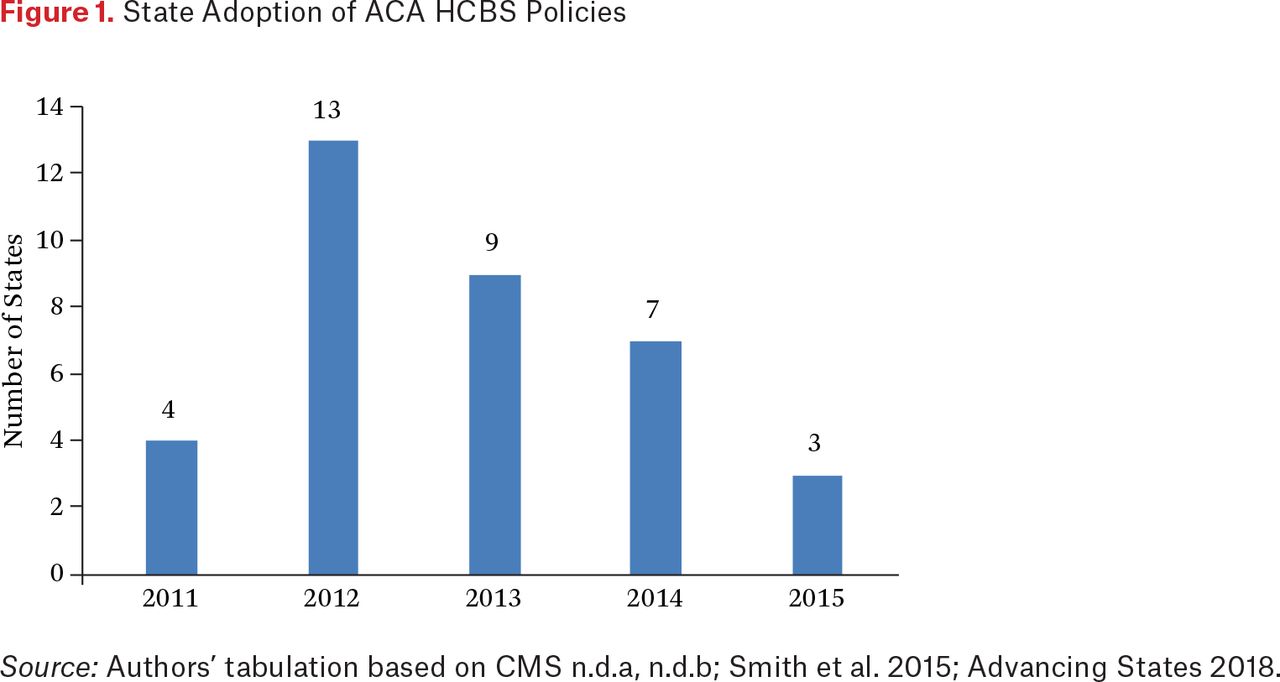
In the panel model, we used a dichotomous variable indicating whether the state adopted any one of the three ACA HCBS programs within a given year. The unit of analysis was the state-year, and observations were included for each state for all years in the dataset, resulting in a balanced panel of fifty states for five years. We calculated the dependent variable by summing the number of policies each state adopted each year. If the sum was one or greater, this variable was coded 1, otherwise 0.2 The year the state submitted their state plan amendment or application to CMS was used as the year of adoption. The data sources for this variable were CMS’s Balancing Incentive Program website, CMS’s state plan amendments database, the National Association of States United for Aging and Disabilities, and the Kaiser Family Foundation (CMS n.d.a, n.d.b; Smith et al. 2015; Advancing States 2018). The study period extended from 2011 to 2015 and included 235 observations; Alaska, Hawaii, and Nebraska were excluded because of missing data on key variables.
The cross-sectional model had one observation for each state. The dependent variable for this model was a dummy variable indicating whether or not the state had adopted any of the three policies. This variable was coded 1 if the state had adopted as least one of the ACA HCBS policies as of December 31, 2015, and 0 if it did not. The data sources for this variable were the same as the dependent variable for the panel model. Alaska and Hawaii were omitted for missing data so the total number of observations in this model was forty-eight.
Figure 1 displays the number of adoptions by year. As shown, 2012 saw the largest number of adoptions and 2015 the smallest. This is partly because states were no longer able to apply for BIP after 2014. In total, between 2011 and 2015, twenty-one states adopted none of the programs, twenty states adopted one, six states adopted two, and three states adopted all three.
Independent Variables
The variable Democratic control ranged from zero to three and indicated the number of legislative chambers and governor’s office with Democratic leadership (National Governors Association 2015; National Conference of State Legislatures 2015). The variable liberal ideology was a continuous variable indicating the political liberalism of the state’s congressional delegation. The measure was calculated using the Americans for Democratic Action (ADA)’s Annual Voting Records (Americans for Democratic Action 2017). In the ADA voting records, each legislator receives a score ranging from 0 to 100, higher scores indicating greater political liberalism. For this study, each state’s individual legislators’ scores were averaged to generate a political liberalism score for the state.3
The state employees per thousand residents variable was a continuous variable calculated based on the number of total full-time equivalent (FTE) employees for each state divided by the total state population from the Census Bureau’s population projections divided by a thousand (Census Bureau 2017, 2016b).4 Gubernatorial power is measured using an index developed by Thad Beyle and Margaret Ferguson (Ferguson 2017). The data to calculate the index was derived from the Book of States tables 4.4, 4.9, and 4.10 (Council of State Governments 2010–2015), the National Governors Association annual governors’ roster (2015), and the National Conference of State Legislatures’ annual state and legislative partisan composition (2015). We used the average salary of state legislators as a proxy for legislative professionalism. The variable measuring legislative professionalism was the real annual salary of state legislators per $1,000 in 2009 dollars. For states that pay legislators a per diem salary, the salary was calculated based on the per diem and length of the legislative session. The data for this variable comes from the Book of States table 3.9 (Council of State Governments 2010–2015).
Three variables were proxy measures for interest group power and political influence of LTSS providers: number of nursing facility beds per elder, percentage of for-profit nursing facilities beds, and number of home health agencies per hundred thousand residents. The first variable was a continuous variable that measured the number of nursing home beds per thousand individuals sixty-five and older. The nursing facility bed data came from CMS’s Nursing Home Compare dataset (CMS 2016; U.S. Census Bureau 2016b). The Nursing Home Compare dataset also identifies the ownership status of each nursing home as either for-profit, government, or nonprofit; from this, the proportion of for-profit nursing homes was calculated. The measure of home health agencies per capita was calculated by dividing the number of home health agencies in each state by the state population per hundred thousand. Data were derived from CMS and the Census Bureau’s annual population projections (CMS 2017; Census Bureau 2016b).
Two variables, percentage of elder population and the percentage of population with a disability were proxy measures for interest group power and political influence of consumer advocates. The first variable was a continuous variable indicting the percentage of the state population age sixty-five and older. This variable was calculated using data from the Census Bureau’s annual population projections (2016b). The variable measuring the percentage of the population with a disability was also a continuous variable. The percentage of the population with a disability was calculated based on the percentage of the civilian noninstitutionalized population in each state with a disability (Census Bureau 2016a).
This study included two economic measures: fiscal health and fiscal capacity. Both variables were lagged one year because policies are often based on the prior year’s fiscal outlook. Fiscal health was measured by a continuous variable based on the average state unemployment rate. Data for this variable came from the Department of Labor (BLS 2016). Fiscal capacity was measured by real per capita personal income per $1,000 from the Department of Commerce (BEA 2016).
Several variables measured existing Medicaid HCBS programs and policies, including 1915(c) HCBS waivers, state plan personal care benefits, and spending levels. These variables were lagged one year because a prior year’s HCBS program and policies may influence the current year’s policy adoption. The 1915(c) waiver variable indicated the number of 1915(c) HCBS waivers the state operated in each year (CMS n.d.c). The state plan personal care variable was a dichotomous variable indicating whether the state offered a state plan personal care benefit. The variable HCBS percentage was the ratio of total Medicaid HCBS spending divided by total Medicaid LTSS spending from the Truven Long-Term Services and Supports Expenditure data (Wenzlow, Eiken, and Sredl 2016). Last, the variable measuring HCBS spending per capita was measured based on the total Medicaid HCBS spending divided by the state population from the Census Bureau’s population projections (Wenzlow, Eiken, and Sredl 2016; Census Bureau 2016b).
Four variables measured existing LTSS and Medicaid politics targeted at provider supply and program eligibility. Two dichotomous variables measured whether the state had a home health aide certificate-of-need program or a nursing facility certificate-of-need program. The variables were coded 0 if the state did not have a CON program and 1 in years the state did have one (National Conference of State Legislatures 2017b). In addition, we included a dichotomous variable indicating whether the state provided Medicaid benefits to the medically needy. This was coded 0 if the state did not have a medically needy program and 1 if it did (MACPAC 2017). All three variables were lagged one year. Last, we included a dichotomous variable, Medicaid expansion, indicating whether the state adopted the Medicaid expansion (Kaiser Family Foundation 2019). This was coded 1 in the year the state adopted the Medicaid expansion and in subsequent years and 0 if the state did not adopt the Medicaid expansion that year or at all.
The longitudinal model included indicator variables for each program reflecting whether the state adopted BIP, CFC, or the 1915(i) in prior years. These variables were coded 1 in the year after a state adopted the specific policy and for all subsequent years in the dataset. Including these variables in the panel model allowed us, in part, to control for the fact that as a state adopts these policies it has fewer available policies to adopt. For example, if a state adopted BIP in 2012, the state could no longer adopted BIP and would only have the opportunity to adopt CFC or the 1915(i) state plan benefit thereafter.5
The panel and cross-sectional models also included variables indicating whether a neighboring state had adopted these policies previously. These variables were based on the cumulative percentage of contiguous states that had adopted any of these three policies up to that point. These variables were lagged one year because a state’s policy development may be influenced by observing the action of a nearby state the year prior.6
ANALYSIS
Descriptive statistics on all study variables are reported. Because the data set included multiple observations for the same state, we estimated the model with generalized estimated equations (GEE) to account for correlation among the observations for each state across years. GEE estimates reflect a population average and this approach has been used to model policy adoption longitudinally (Daley and Garand 2005; Yi, Feiock, and Berry 2017). In the model, we used robust standard errors and AR(1) covariance structure. Year indicator variables were included in the panel model as well.
A logistic regression with robust standard errors was used for the cross-sectional model. The relatively small sample precluded the inclusion of all independent variables used in the longitudinal model. Those for the cross-sectional model were thus chosen based on their theoretical importance for predicting the dependent variable. When multiple variables measured similar concepts, the one that most clearly captured the concept examined was included. For example, elected officials’ liberalism was included as a measure of political factors because political parties are not uniform across states. For this reason, the political liberalism of a state may be a better measure of ideological support for adding optional Medicaid programs than partisanship. The bureaucratic capacity measure, the number of FTEs per thousand people, was chosen to represent governing capacity because the literature suggests that program administrators demonstrate considerably more influence than governors or state legislatures in highly technical areas such as Medicaid policy (Schneider and Jacoby 1996; Schneider, Jacoby, and Coggburn 1997; E. Miller 2006). Similarly, the choice of nursing facility beds per thousand people sixty-five and older in the industry category was informed by nursing homes being among the most active pressure groups on state government and rebalancing having a disproportionately large, adverse impact on the industry’s financial bottom line (Wiener and Stevenson 1998; N. Miller, Harrington, and Goldstein 2002). Including the percentage of the population with a disability was informed by the considerably greater success states have had rebalancing LTSS for the ID/DD population than for the older adult population, as noted earlier (Eiken et al. 2018). The 1915(c) waivers, the personal care program, and percentage Medicaid LTSS spending on HCBS measures were included from the existing HCBS and LTSS policies category because they most directly get at prior state efforts to make progress in this area (N. Miller et al. 2001; Kitchener et al. 2007). Finally, the indicators for Medicaid expansion and neighboring state adoption were included because of their potential theoretical importance (Jacobs and Callaghan 2013; Mooney 2001), and because no other variables measure those concepts.
The results of both models report the coefficients and odds ratios. The odds ratio is the exponentiated value of coefficient. Odds ratios greater than 1 indicate a positive relationship and those of less than 1 a negative relationship. For example, an odds ratio of 1.25 would indicate that a one unit change in the independent variable would result in a 25 percent increase in the odds of adoption.
RESULTS
A bivariate correlation matrix indicated that most of the variables were not highly correlated (< 0.55); however, the Democratic control and ADA Ideology index variables were highly correlated (0.77).7 Table 2 displays the mean, standard deviation, minimum, and maximum for all of the independent variables. The results for the longitudinal and cross-sectional models predicting ACA HCBS policy adoptions are shown in table 3.
Descriptive Statistics for State Policy Variables, 2011–2015
Factors Influencing Adoption of ACA HCBS Programs
The significant predictors of ACA HCBS program adoption were state political ideology, state employees per population, per capita income, nursing facility beds per elderly population, and existing HCBS policies. Consistent with expectations, the ADA Ideology index variable was statistically significant and positive in both the longitudinal and cross-sectional models (b = 0.055, p < .01; b = 0.054, p < .05). States were 5.6 percent more likely to pursue the ACA HCBS policies in a given year with each unit increase on the ADA Ideology index in the longitudinal model (OR = 1.056).8 In the cross-sectional model, each unit increase on the ADA Index increased the likelihood of adopting these policies by 5.5 percent (OR = 1.055). Although Democratic control was not significant in this longitudinal model, it was when the ADA Ideology index variable was removed (b = 0.381, p < .05).
In both models, states with more state FTEs were less likely to pursue these policies (b = –0.138, p < .05; b = –0.337, p < .01) which is opposite of expectations.9 In the longitudinal model, each additional state FTE per thousand residents decreased the likelihood of adoption of the ACA HCBS policies by 12.9 percent (1- (OR = 0.871)). In both the longitudinal and cross-sectional models, the impact of the number of nursing facility beds per thousand elders was also significant but the opposite sign of expectations (b = 0.049, p < .05; b = 0.106, p < .05). Each additional nursing facility bed per thousand elders increased the likelihood of pursuing these policies by 5 percent (OR = 1.050) in the longitudinal model. Also opposite of expectations, states with higher per capita income were less likely to pursue these policies (b = –0.143, p < .05; b = –0.339, p < .01). In the longitudinal model, each additional $1,000 in per capita income decreased the likelihood of adoption by 13.3 percent (1–(OR = 0.867)).
Consistent with expectations, several variables measuring HCBS policies in the previous year proved related to state adoption. In the longitudinal and cross-sectional models, the variable measuring the number of 1915(c) waivers in the previous year was significant (b = 0.195, p < .05; b = 0.348, p < .05). Each additional waiver in the previous year was associated with a 21.5 percent increased likelihood of pursuing the ACA’s HCBS policies in a given year in the longitudinal model (OR = 1.215), whereas each additional waiver was associated with a 41.7 percent increased likelihood of adoption in the cross-sectional model (OR = 1.417). In the longitudinal and cross-sectional models, states with a state plan personal care benefit were more likely to pursue the ACA’s HCBS policies relative to states that did not offer this benefit (b = 0.967, p < .05; b = 2.400, p < .05) with states offering these services being 2.63 times more likely to adopt the ACA HCBS options (OR = 2.63) in the longitudinal model and more than eleven times more likely in the cross-sectional model. The percentage of Medicaid LTSS spending on HCBS in the previous year was also significant but negative in both models (b = –0.094, p < .01; b = –.157, p < .01). This indicates that states were 9 percent less likely to adopt the ACA HCBS policies in a given year with each percentage point increase in Medicaid LTSS spending on HCBS during the previous year (1–(OR = 0.910)) in the longitudinal model.
In the longitudinal model, the cumulative percentage of neighboring states that adopted the ACA HCBS programs was significant and positive (b = 0.013, p < .05). States were 1.3 percent more likely to adopt these policies in a given year with each percentage point increase in this variable (OR = 1.013). In addition, in the cross-sectional model, a variable measuring whether the state adopted the Medicaid expansion was statistically significant (b = 2.452, p < .01). Consistent with expectations, states that expanded Medicaid were nearly twelve times more likely to pursue the ACA HCBS programs than states that did not expand Medicaid (OR = 11.608).
DISCUSSION
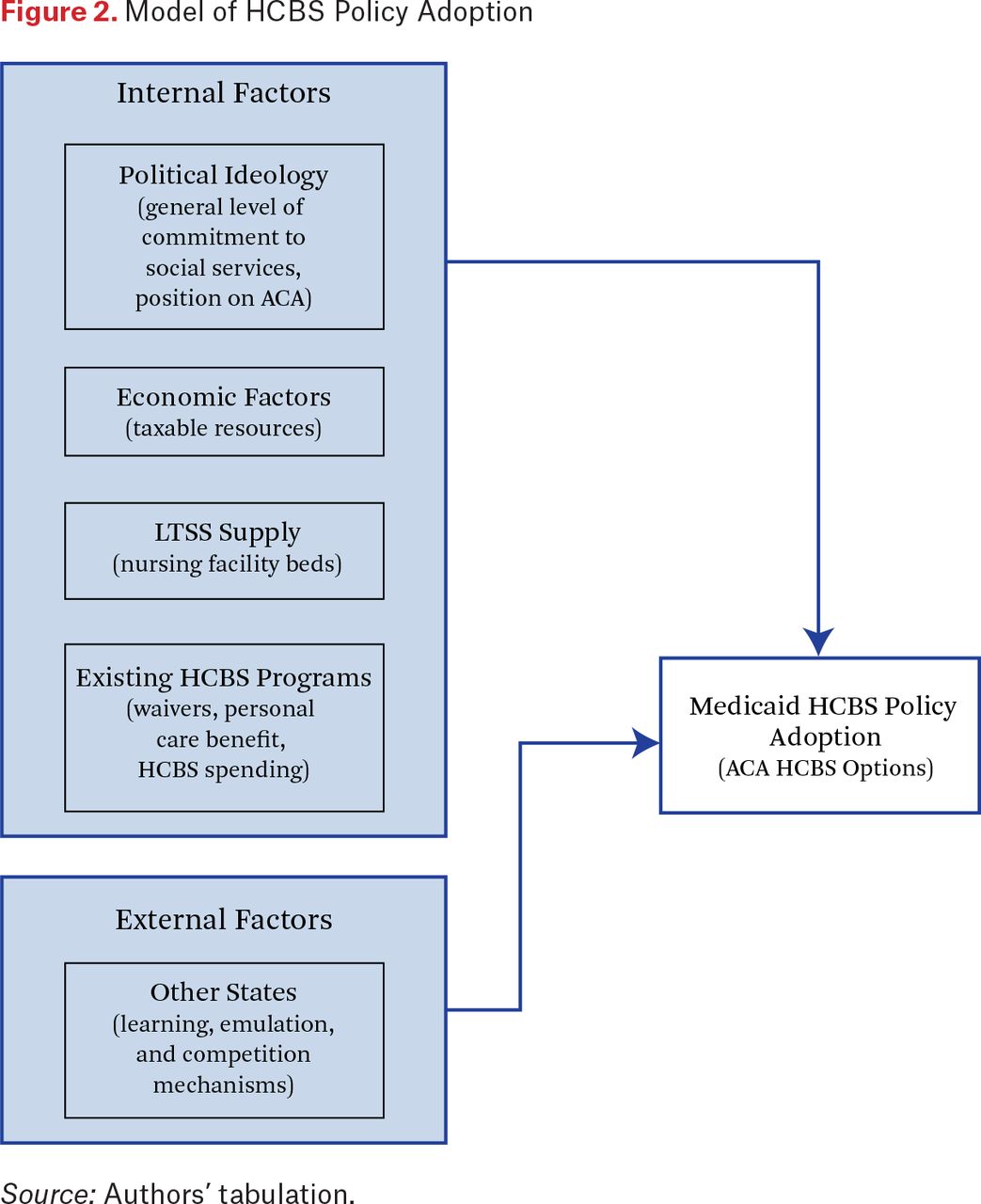
Based on the findings from the regression models, we propose a model of HCBS policy adoption (see figure 2). The diagram identifies factors internal and external to the state that may affect the adoption of new HCBS policies. Overall, the results provide evidence for the role of political ideology in the ACA HCBS policy adoption decision. In both the longitudinal and cross-sectional models, states with a more liberal political ideology were more likely to pursue the ACA HCBS policies. This finding suggests that the inclusion of HCBS programs within the larger ACA legislation may have deterred some states from adopting these policies for ideological reasons. The ACA was and continues to be a highly partisan piece of legislation strongly opposed by many conservative leaders at both the state and national levels. Indeed, interviews with individuals involved in HCBS policymaking conducted as part of the larger project within which this research is situated indicates that opposition to the ACA influenced some states’ positions on the LTSS opportunities.10 According to a national consultant, for some states “the political climate was very hostile to the Affordable Care Act, and so anything that came out of the ACA was just immediately tainted. . . . In a number of states, it [BIP] was just politically dead on arrival” (Beauregard 2019). That ideology played a role is further indicated in the finding that states adopting the Medicaid expansion—most of which were liberal in orientation—were nearly twelve times more likely to adopt at least one of the ACA HCBS options by the end of the study period. Future federal policy initiatives should consider whether the benefits of including HCBS policies within larger controversial pieces of legislation outweigh the drawbacks. On the one hand, policymakers often need to add HCBS initiatives to larger pieces of legislation simply to pass legislation and get programs enacted. On the other hand, attaching HCBS policies to controversial legislation may dissuade some states from adopting policies they might otherwise be interested in pursuing. Although the political ideology measure was significant in the findings, the number of branches of government controlled by Democrats was significant only after removing the political ideology measure. This finding suggests that ideology may be a mediator variable, and that the reason Democratic control influences adoption of these HCBS policies is ideological differences between the parties.
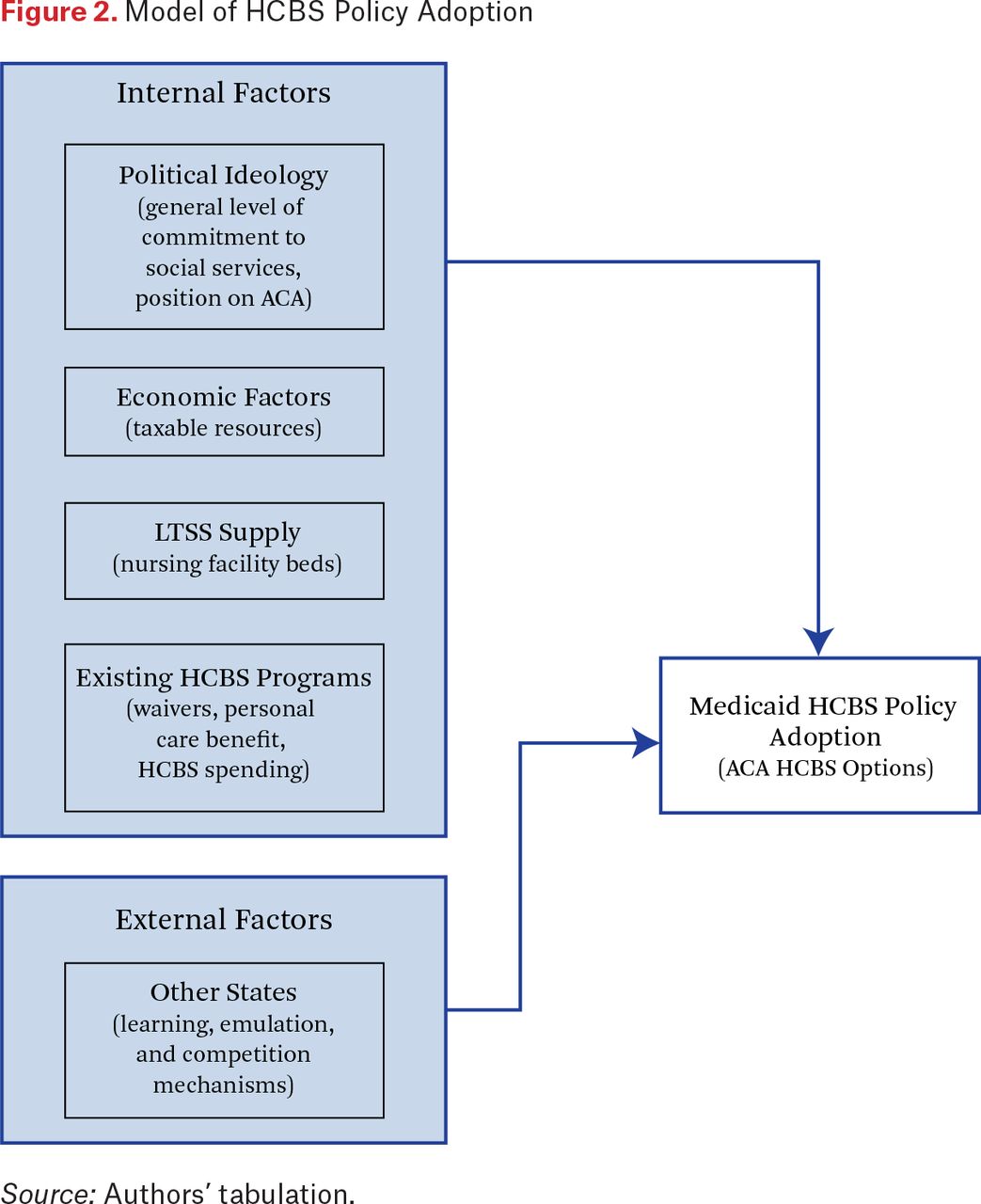
Model of HCBS Policy Adoption
Source: Authors’ tabulation.
The hypotheses related to the importance of governing capacity in policy adoption were not supported. Contrary to expectations, states with more state FTEs per thousand people were less likely to pursue the ACA HCBS policies and the measures of gubernatorial power and legislative professionalism were not statistically significant. The negative sign for state FTEs per thousand people is surprising given that the literature suggests that state bureaucrats within the state Medicaid agency often initiate Medicaid policy changes (Schneider and Jacoby 1996; Schneider, Jacoby, and Coggburn 1997). In addition, federal reports suggest that limited state staff was one impediment to states’ adoption of the ACA HCBS policies (GAO 2012; HHS 2015). One reason for this unexpected finding could be that state officials realized that they could use the enhanced funding associated with some of these program to hire additional staff within HCBS programs, thereby bolstering limited state capacity in this area. States that experienced significant reductions in staff in response to the Great Recession may have perceived additional Medicaid funding as a mechanism to increase staffing levels.
Overall, the results provide limited support for the role of interest groups, including consumer advocates and provider representatives in policy adoption decisions. The measures for elder and disability advocacy and HCBS providers were not statistically significant, though one measure for nursing facility strength was but the opposite sign of expectations. States with more nursing facility beds per elder population were more likely to pursue the ACA HCBS programs. This finding may suggest that this measure is capturing supply of nursing facility beds as opposed to the strength of the nursing facility industry. States with more nursing facility beds per elder population may have more incentives and motivations to decrease spending on institutional care and increase HCBS options in an effort to meet the preferences of residents and reduce costly nursing facility care.
The findings also suggest that economic factors influenced state adoption decisions. Contrary to expectations, state with lower per capita income were more likely to pursue the ACA HCBS programs. One potential explanation for this contradictory finding is that many of these programs included enhanced federal revenue, which may have made them comparatively more attractive for states with lower per capita income. Furthermore, the perceived cost-effectiveness of HCBS relative to institutional care may have made adopting the ACA’s HCBS provisions more appealing for less wealthy states with greater resource constraints, all else being equal.
The results also indicate that states’ existing HCBS policies influenced the adoption decision. In both models, states with a higher percentage of Medicaid LTSS spending devoted to HCBS were less likely to adopt these policies. This result indicates that the ACA’s HCBS programs had the intended effect of encouraging states who spent less on HCBS as a proportion of total Medicaid LTSS spending to pursue additional options to increase this spending. In addition, financial incentives, such as the enhanced federal match associated with BIP and CFC, may promote greater spending on HCBS particularly in states that have achieved less rebalancing to date.
Alternatively, both the longitudinal and cross-sectional models indicate that states with state plan personal care benefits and more 1915(c) waivers were more likely to adopt the ACA’s HCBS options. That states with state plan personal care benefits and more HCBS waivers were more likely to adopt suggests that states adopted the ACA HCBS policies in part because the programs were consistent with broader state HCBS goals. In addition, states with robust HCBS offerings may have financial incentives to pursue new federal HCBS opportunities in hopes of obtaining greater federal matching revenue for the offerings that are already provided. Many states that adopted CFC sought to transition existing personal care benefits or 1915(c) waiver services into CFC to receive the additional 6 percent federal match for these services.
The state plan personal care benefits and 1915(c) findings also suggests that states with more robust HCBS systems may be able to offer additional programs more easily than states with not as well developed systems. The provision of Medicaid HCBS programs requires states to have infrastructure and processes in place to conduct eligibility determinations, enroll individuals, ensure quality oversight, and have provider networks. States that already have these systems in place for personal care programs and 1915(c) waivers may be able to leverage this for new HCBS programs. In contrast, states with less robust HCBS systems may need to enact greater necessary programmatic and structural changes to pursue these new opportunities. This dynamic suggests that even greater financial incentives may be needed to help offset the additional state infrastructure spending associated with expanding the array of HCBS options available to promote adoption among states with less robust HCBS programs. Without additional incentives, the gap between the HCBS have and have-not states may widen given that states already inclined toward expanding the array of HCBS may be more likely to take advantage of any new options.
This study provides support for the role of neighboring states in policy adoption decisions. The literature indicates that states may look across their borders to address common policy problems or to learn from other states’ experiences (Balla 2001; Berry and Baybeck 2005; E. Miller and Banaszak-Holl 2005). The longitudinal models indicate that states were more likely to adopt the ACA HCBS policies if neighboring states had adopted them policies previously. This finding may suggest that the number of states pursuing these options may increase as states observe other states using them in their Medicaid programs.
LIMITATIONS
This study contributes to our understanding of state policy adoption decisions surrounding the new ACA HCBS programs, but there are several limitations. One limitation was the relatively short timeframe for this study. States could begin adopting these policies in 2010, for the 1915(i), and 2011, for BIP and CFC. The period for studying adoption of the 1915(i) and CFC programs ended in 2015 due to available data on the independent variables. The short time frame limited the number of observations in the longitudinal model. This in turn limits the statistical power of the models estimated, reducing the probability of finding statistically significant relationships. In addition, in the cross-sectional model, we needed to reduce the number of predictors of adoption examined given the larger number of possible predictors relative to the limited degrees of freedom available.
A second limitation is related to the operationalization of some variables. Several variables were proxy measures and may not adequately capture the concept being measured. For example, the number of nursing facilities and percentage of elders in the population were proxy measures for the strength of the nursing facility and elder lobbies in each state but these variables could also measure supply of institutional care and demand for long-term services and supports, respectively. The disability measure was also based on the overall percentage of the population with a disability and did not differentiate among physical, intellectual or developmental, and mental health disabilities. Significant differences exist in the specific target populations for HCBS which this measure did not capture. In addition, the variable measuring bureaucratic capacity was the number of FTE state employees per thousand people. This variable does not capture whether these state employees are within the Medicaid agency or other departments involved in HCBS policymaking. One measure of existing HCBS policies was the number of 1915(c) waivers a state operates. This variable, however, does not capture the size of each state’s waivers and whether the waiver is designed to serve a small, targeted population or the state has a waiting list for its waivers. In addition, states can offer HCBS services outside of 1915(c) waivers including through 1115 demonstration waivers or managed care.
CONCLUSION
This research sought to examine states’ policy adoption decisions concerning three HCBS programs included in the ACA. The BIP, CFC, and the 1915(i) HCBS state plan benefit were optional programs states could elect to adopt. The states pursuing these opportunities were diverse and differ from the states that have adopted the Medicaid expansion or exchange aspects of the ACA. Our findings indicate that political ideology, economic factors, and existing HCBS programs, were important predictors of state policy adoption. The importance of existing HCBS programs suggests that the adoption of other HCBS and LTSS policies is strongly influenced by previous policy development. The role of ideology in the adoption decision may only play a role when HCBS or LTSS policies are included within larger pieces of controversial legislation.
This study contributes to our understanding of state policy adoption and of the HCBS policies within the ACA. It also has implications for federal officials. This research expands the HCBS policy adoption literature because the opportunities in the ACA are arguably the most substantial development of Medicaid HCBS options for states since the authorization of 1915(c) waivers in the early 1980s. In addition, most research on the ACA focuses on the health insurance and exchange aspects of the legislation. Although some studies and reports have examined the HCBS opportunities in the ACA (GAO 2012; Dorn et al. 2016), this research covers a longer time frame and explores the adoption of multiple HCBS programs. Indeed, given the three HCBS policies examined, the findings may have more generalizability than if only one policy had been. Last, based on this research, federal officials interested in spurring states to achieve greater rebalancing of Medicaid LTSS can understand the factors that influence state HCBS policymaking and develop policies to promote further rebalancing.
FOOTNOTES
↵1. Olmstead v. L.C., 527 U.S. 581 (1999).
↵2. In most years, states adopted only one ACA HCBS policy within a given year. In only four instances did a state adopt two within a year.
↵3. We also ran a model using William Berry and colleagues’ (1998) “revised 1960–2016 citizen ideology series” and overall the results were similar.
↵4. We also ran a model using average non-education state FTEs salary as an alternative measure for bureaucratic capacity but it was not statistically significant. In the final model, we used number of FTE per thousand people because other studies examining state LTSS policy adoption have used a similar measure (Miller et al. 2012; Miller and Wang 2009).
↵5. We also considered including separate dummy variables indicating one policy adopted already, two policies adopted already, and three policies adopted already. However, the three policies adopted variable predicted non-adoption perfectly since two states that adopted three policies did not subsequently adopt additional policies. The result was that two observation and the three adoption dummy variable were dropped from the regression, leaving only the one policy and two policies adopted variables. As an alternative, we ran a regression that included dummy variables indicating one policy adopted already and two or more policies adopted already. The results of both the original and alternative models were essentially the same to the model presented below including indicator variables for each specific policy already adopted.
↵6. We also looked at alternative specification of the diffusion model, in particular, the innovator dynamic. We measured this variable as the cumulative percentage of innovator states, as measured by percentage spending on Medicaid HCBS, who adopted any of the three ACA policies in a given year. However, the model would not estimate due to multicollinearity.
↵7. We also ran a model separating the Democratic control variable into two separate variables: a Democratic governor variable and a party control variable based on whether the government was unified, divided, or divided legislature. These two variables were not highly correlated with the ADA Ideology index variable. In both the original and alternative models, the ADA Ideology variable index was statistically significant but none of the measures of Democratic or party control were significant.
↵8. As noted, the results were similar when we ran the models using the revised Berry and colleagues 1960–2016 citizen ideology series. With both measures, an increase in ideology toward greater liberalism increased the likelihood of pursuing these polices by approximately 5 to 6 percent.
↵9. As noted, the measurement of average state non-education salary was not statistically significant.
↵10. The interviews were conducted from 2016 to 2018 with individuals involved in LTSS policy in three states and nationally. Interviewees included national officials, national advocacy organizations, other policy experts, officials in both the bureaucracy and legislature of the state, and members of state-level interest groups.
- © 2020 Russell Sage Foundation. Beauregard, Lisa Kalimon, and Edward Alan Miller. 2020. “Why Do States Pursue Medicaid Home Care Opportunities? Explaining State Adoption of the Patient Protection and Affordable Care Act’s Home and Community-Based Services Initiatives.” RSF: The Russell Sage Foundation Journal of the Social Sciences 6(2): 154–78. DOI: 10.7758/RSF.2020.6.2.07. The authors acknowledge the University of Massachusetts Boston Doctoral Dissertation Grant program and the Department of Public Policy for providing funding for this research. The authors would also like to thank the editors and participants at the Russell Sage Foundation’s Social, Political, and Economic Effects of the Affordable Care Act conference for their invaluable insights. Direct correspondence to: Lisa Kalimon Beauregard at lkalimon{at}gmail.com, Massachusetts Executive Office of Elder Affairs, One Ashburton Place, 5th Floor, Boston, Massachusetts 02108.
Open Access Policy: RSF: The Russell Sage Foundation Journal of the Social Sciences is an open access journal. This article is published under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.
REFERENCES
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.