
Abstract
We argue that partisan polarization in public support of the Affordable Care Act (ACA) is affected not only by policy design but also by which party makes those decisions. Using an innovative dataset that measures state-level quarterly ACA support from 2009 through the start of the 2016 presidential election, we find that opinions toward the ACA are less polarized in states with misaligned partisan environments where Republican governors support Medicaid expansion. We also find evidence that Republican opposition intensifies when a Democratic governor supports expansion. We do not find consistent evidence of such patterns for governors’ positions on state health insurance exchanges. Our research sheds light on a key aspect of how health policy preferences respond to shifting political contexts in a polarized, federated polity.
President Barack Obama’s decision to devolve policymaking related to the Affordable Care Act (ACA) to the subnational level and the Supreme Court’s decision to grant states the choice to refuse Medicaid expansion have led to a checkerboard of ACA policy designs across the fifty states. Most notably, states were given autonomy over two major policy choices: whether to implement the Medicaid expansion and whether their health insurance exchange is established and managed by the state, the federal government, or a mixture of both. The most common explanation for variation in these choices is elite partisanship. Republican-led, conservative states have tended to delay decisions, default to a federal marketplace, and opt out of Medicaid expansion. In contrast, more liberal Democrat-led states have been more likely to establish their own insurance marketplace and expand Medicaid (Barrilleaux and Rainey 2014; Callaghan and Jacobs 2014; Lanford and Quadagno 2016; Rigby and Haselswerdt 2013; Jones, Singer, and Ayanian 2014). States continue to experiment with ACA policy designs. At the time of this writing, eighteen states—the majority being conservative—have approved or pending provisions for Medicaid work requirements.1
Some instances, however, have been surprises—when Republican-led, conservative states proceed with expansive policy choices. For example, Iowa, Michigan, Arizona, and Indiana adopted Medicaid expansion early.2 More recently, ACA advocacy groups have used the ballot initiative to expand Medicaid in previously non-expansion, conservative states such as Idaho, Utah, and Nebraska.3
Despite the willingness of some Republican policymakers to implement parts of the law, the partisan split in attitudes toward the ACA has been one of the most salient and crucial aspects of U.S. politics (Jacobs and Mettler 2011, 2016, 2018). To the extent that political elites are responsive to public opinion, the partisan chasm in ACA attitudes has implications for policy outcomes. Alternatively, to the extent that elites play a role in driving public opinion, partisan attitudinal differences are instructive indicators of policymakers shaping the political context and potentially affecting electoral outcomes. Either way, partisan attitudes toward the ACA have implications for policy feedback processes and democratic responsiveness (Jacobs and Mettler 2011, 2018). We argue that ACA polarization—the partisan gap in public support for the ACA—is affected not only by the decisions states make about implementing parts of the ACA, but also by which party makes those decisions. We expect ACA opinion polarization to be largest in states with aligned partisan environments, where Democratic policymakers support and Republican policymakers oppose ACA implementation, and lowest in misaligned partisan environments, where Republican policymakers support some aspects of implementation.
Understanding variation in state-level ACA attitudes among partisans has significant implications for health policy. Although both the public and politicians have been highly polarized on health reform at the national level, state-level exceptions have been large and consequential. Such subnational dynamics have the potential to reshape national politics from the bottom up (Pacheco and Maltby 2019). However, whether and when this happens depends upon how citizens respond to shifting political contexts in a polarized, federated polity (Jacobs and Mettler 2018; Lerman and McCabe 2017; Michener 2018). Our research sheds light on a key aspect of this larger picture by investigating how health policy preferences are affected by partisan political environments.
We use an innovative dataset that measures Republicans’ and Democrats’ state-level quarterly ACA support from 2009 through the start of the 2016 presidential election. Our approach differs from previous research using small area estimation techniques in that we include partisanship in the poststratification stage and estimate ACA support among Democrats and Republicans within each state. To do this, we gathered monthly data from national surveys including the Kaiser Family Foundation (KFF), Gallup, Pew, and CBS/NYT. We then measure the percentage of state residents who favor the ACA and identify with the Republican (or Democratic) party, which allows us to quantify partisan polarization on the ACA in each state over twenty-seven time points.
Drawing on such rich data, we find that ACA attitudes are less polarized in states where Republican governors have announced support for Medicaid expansion. We also find suggestive evidence that opinion is more polarized in states where Democratic governors announce support for a state-based health insurance exchange, but here the case is less clear cut. Although we implement a number of empirical strategies to rule out issues of endogeneity, it is entirely possible that Republican governors had more leeway in political environments where mass polarization was particularly low. We contextualize this finding in a broader theoretical framework, describe it in more detail, make the case for why it matters, and outline the additional questions it raises going forward, including how to interpret our results in the face of endogeneity.
MISALIGNED PARTISAN ENVIRONMENTS
Misaligned partisan environments at the state level (when state political elites adopt a salient policy position that does not align with partisan expectations) are theoretically and substantively consequential. In an era of intense partisan polarization, it is risky and difficult for state partisan elites to make decisions that run counter to the expectations of either their elite copartisans (at the state or national level) or their core constituencies. Nonetheless, a misaligned partisan environment is indicative of precisely such a paradoxical political position. With respect to the ACA, scholars have now begun to consider the reasons why state political elites have pursued policy routes that rub against popular partisan expectations and expose them to various kinds of risk (Fording and Patton 2020; Jacobs and Callaghan 2013; Nicholson-Crotty 2012; Rose 2015; Scott 2013). In this article, we turn to another question: what are the consequences of misaligned partisan environments for mass public opinion?
Investigating the effect of misaligned partisan environments on popular political attitudes opens a crucial avenue for advancing understanding of the complex relationships between democracy, public policy, and public opinion in a polarized, federated polity. Scholars have increasingly discovered that the linkages between public opinion and public policy are not at all straightforward. Policymakers do not simply respond to public preferences. Instead, democratic responsiveness is conditioned by a number of factors including class, race, electoral context, partisan alignments, and much more (Canes-Wrone 2015; Bartels 2008; Grogan and Park 2018). Moreover, the relationship between public opinion and political responsiveness can be reciprocal: cues from political elites shape public attitudes (Zaller 1992; Jacobs and Shapiro 2000). Notwithstanding these broad strokes, much is still unknown about the conditions under which elites sway mass attitudes. We highlight an especially illuminating line of inquiry by investigating how state contexts of partisan misalignment affect popular policy attitudes.
We expect misaligned partisan environments to influence public opinion on the ACA. More precisely, we hypothesize that opinions toward the ACA will be most polarized in states with aligned partisan environments (where Democrat officials support expansion and state exchanges and Republican officials oppose them) and least polarized in states with misaligned partisan policy environments (where Republican officials support at least some form of implementation). Our arguments rest on two assumptions. First, that state-level policy cues influence ACA attitudes at all. This assumption is corroborated by existing evidence that the adoption of the ACA influenced support for spending on health care at the national level (Morgan and Kang 2015) and that the timing and type of gubernatorial announcements of marketplace ACA decisions is related to state-level ACA attitudes (Pacheco and Maltby 2017, 2019).
The second assumption—which we empirically test in this article—is that partisanship affects the way that citizens react to state-level policy decisions made by political elites. The ACA is both a source of salient partisan debate and a policy that varies widely across states (Richardson and Konisky 2013). This suggests that state-level partisan cues should be particularly influential in shaping ACA policy preferences. Especially for complex policies like the ACA, citizens likely rely on partisan cues for information. Partisanship, thus, informs popular ideas about policies through selective information processes. One such process is motivated reasoning (Bolsen, Druckman, and Cook 2014; Druckman, Peterson, and Slothuus 2013; Leeper and Slothuus 2014; Taber and Lodge 2006). Motivated reasoning refers to the tendency to seek out information that confirms prior beliefs . . . view evidence consistent with prior opinions as stronger or more effective . . . and spend more time arguing and dismissing evidence inconsistent with prior opinions” (Druckman, Peterson, and Slothuus 2013, 59). Motivated reasoning is the psychological mechanism by which partisans often discount, counterargue, or ignore new information that challenges existing beliefs. Contrastingly, when citizens are presented with information congruent with predispositions, the information will be easily accepted because “it requires no effort to accept what one already knows is true” (Redlawsk 2002, 1023).
Given existing knowledge of motivated reasoning processes, we expect asymmetric shifts in ACA support based on partisanship. More precisely, Republicans in states where Republican governors announce pro-ACA decisions (misaligned partisan environments) will be uniquely motivated to reason more favorably about the ACA because an important Republican figure in their state has signaled that aspects of the law are acceptable. Also possible, though we suspect much less likely, is a backfire effect for Democrats against the ACA in states with Republican governors who push for implementation.
MEASURING ACA PARTISAN POLARIZATION IN THE STATES
To test our hypotheses about partisan polarization, we need measures of state-level ACA support over time among partisans. We start by gathering monthly data from national surveys, including the Kaiser Family Foundation (KFF), Gallup, Pew, and CBS/NYT. We selected these surveys for two reasons. First, the survey questions have similar wording. This increases our confidence that changes in opinion are not due to shifts in questionnaire design. Second, by combining questions across surveys, we increase the amount of information and therefore the reliability of our estimates both across states and over time.
We use the following question to measure support for the ACA: “As of right now, do you generally support or generally oppose the health care proposals being discussed in Congress?” Respondent answers ranged from strongly support to strongly oppose. As the ACA became law, the question stem changed slightly to “As you may know, a new health reform bill was signed into law.” In the end, we collected data on 122,103 respondents from 2009 to 2016. This tracks opinion a few months before the ACA became law through the beginning of the 2016 presidential election. We use an increasingly popular small area estimation technique called multilevel regression and poststratification (MRP) to estimate state opinions toward the ACA (Gelman and Little 1997; Park, Gelman, and Bafumi 2004, 2006). We are able to get subgroup opinion by augmenting the traditional approach and including partisanship in the poststratification stage (more details follow).
The MRP approach uses national surveys to produce accurate estimates of public opinion at low levels of aggregation such as the state (Lax and Phillips 2009) or congressional district (Warshaw and Rodden 2012). Multilevel modeling increases the reliability of less populous units via shrinkage toward the mean. Indeed, the MRP approach is superior to the aggregation method in terms of reliability, particularly when sample sizes are small, for instance, when N is less than 2,800 across all units (Lax and Phillips 2009). Traditional poststratification corrects for nonrepresentativeness due to sampling designs by adjusting estimates using census information.
Adding a Time Component
We add a time component by pooling surveys across a small time frame; in the following example, we use a three-quarter moving average to estimate quarterly opinion toward the ACA. For instance, to get point estimates for Q1 in 2014 using a three-quarter pooled window, we combine all available surveys from Q4 in 2013, Q1 in 2014, and Q2 in 2014 and then perform the MRP technique on this pooled dataset. We use all available surveys in each month. We want to be clear that we do not perform MRP on each month individually; this is not a two-staged approach. Instead, we pool individual level surveys three months at a time and repeat the MRP process for each pooled time window. By pooling and taking the median estimate, the first and last quarters are missing. This approach has been used in previous research to measure state opinion over time (see Pacheco 2012; Pacheco and Maltby 2017, 2019).
Modifying MRP to Estimate State Opinion for Subgroups
MRP is the “gold standard” by which public attitudes have been measured at the subnational level since its introduction in the late 1990s (Gelman and Little 1997), yet scholars continue to advance the method in a number of ways (Caughey and Warshaw 2019). One especially fruitful modification is to estimate subnational opinion for nondemographic subgroups (Kastellec et al. 2015; Caughey, Dunham, and Warshaw 2018). By estimating attitudes at the subnational level broken down by important subgroups, for instance, by partisanship, ideology, self-interest, or knowledge, scholars can explore whether policy designs affect certain segments of the population more than others or whether officials are responsive only to certain, select subconstituents. These types of explorations contribute to our understanding on policy feedback and representation more generally.
However, a major challenge with modifying MRP to estimate subgroup opinions is the lack of nondemographic variables in the census for poststratification. The traditional MRP approach uses population frequencies of states overall (for instance, the count of white, males, age eighteen to twenty-nine with a college degree in California) to improve the representativeness of the estimates in each state. Thus, one can estimate the level of ACA support among college-educated black males ages eighteen to twenty-nine in California, but cannot accurately estimate the level of support among partisans of the same demographic and state profile.
Jonathan Kastellec and colleagues (2015) tackle this challenge by using a two-stage MRP technique where in the first stage they use MRP to estimate partisanship as the response variable. Doing so simulates the number of partisans by each demographic type in each state. In the second MRP, they use the synthetic partisan-demographic geographic types created in the first stage for poststratification after fitting a multilevel model to their main variable of interest, which is public support for judicial nominees.
We take a different, much simpler approach and use a number of large-scale academic surveys to weight our MRP estimates for each partisan-demographic geographic type rather than the census. We first batched the multilevel model estimation into different groups, essentially splitting the analyses based on partisanship. For example, to estimate state opinion toward the ACA for Democrats in each state, we limit the multilevel regression model to include those individuals who identified with the Democratic Party (this includes leaners). To obtain estimates for Republicans, we redo the estimates after selecting only individuals who identified with the Republican Party (including leaners). Next, we use MRP to estimate ACA support separately for Democrats and Republicans using traditional demographic and state-level covariates (Lax and Phillips 2009). Specifically, at the individual level, we use gender, race, age, and education; at the state level, we include region and state presidential vote share in 2012. We do this for each period (described earlier).
We then use a conglomerate of large national surveys to estimate the counts of the demographic and geographic types for each partisan group. These surveys include the cumulative Cooperative Congressional Election Surveys from 2006 to 2014 (N = 279,226), CBS surveys from 2009 to 2011 (N = 51,809), the 2008 and 2012 American National Election Surveys (ANES) (N = 8,015), and the 2006 to 2008 Annenberg Surveys (N = 25,235). We include these surveys for several reasons. First, all of the surveys include questions about partisanship and have the necessary individual level covariates needed in the poststratification stage. Next, the surveys boast large sample sizes; this helps ensure that our estimates are as accurate as possible across all states, but especially for the least populated ones. Finally, we select surveys to match the time frame of our ACA surveys, again, to help increase accuracy.
For this strategy to be successful, we must assume that counts obtained from these surveys approximate the actual population counts of each state. This assumption is a bold one, especially given that the surveys used in the poststratification stage were developed to be representative at the national, not the state, level. It is possible, for instance, for the raw, unweighted data to be quite unrepresentative at the state level. If true, the implication is that our estimates also fail to be an accurate representation of public opinion toward the ACA among partisans in the fifty states.
One way to check this assumption is to compare the demographic and geographic counts obtained from the combined surveys to the census files. Here, we temporarily ignore partisanship and look at how closely counts from the combined surveys are to census-based population targets for gender, race, education, and age in each state. We use the American Community Survey (ACS) five-year estimates for our comparison.
We find that the correlation between the population weights created from the combined surveys to those obtained from the census is a healthy 0.89 across all states and demographic types. Utah has the highest correlation (r = 0.95) and Mississippi the lowest (r = 0.78). When we take the difference for each demographic and geographic type between the population weights created from the combined surveys and those obtained from the census, the mean difference is very small (8.9 × 10–12) with a range of –0.04 to 0.05. Differences for only 157 of the 3,264 possible demographic and geographic types fall outside the 0.02 margin of error. Via these diagnostics, we are confident that using the combined surveys to weight our opinion estimates across demographic and geographic types across partisans is a reasonable approach.
Validity Check
State opinions toward the ACA across partisan groups, if valid as we have measured them, should correlate with other variables that attempt to measure the same concept. Two state surveys asked residents about ACA favorability and partisanship: the Kentucky Health Issues Poll (KHIP) 2010–2014 and the Ohio Health Issues Poll (OHIP) 2011. Both surveys were conducted by the Institute for Policy Research at the University of Cincinnati and funded by the Foundation for a Healthy Kentucky and the Healthy Foundation of Greater Cincinnati.4 When used with proper weights, aggregate estimates from KHIP and OHIP are representative of state populations. A key difference between our estimates and KHIP and OHIP is that the latter are yearly surveys, while our surveys are quarterly. Additionally, recall that our estimates are based off a small moving average, which introduces additional error, albeit to improve reliability. Given this, it would be unlikely for our estimates to correspond exactly with measures from KHIP or OHIP. Nonetheless, we can still get a sense of how well MRP performs by comparing our subgroup estimates with those obtained from KHIP and OHIP.
Table 1 shows the percentage of Kentucky and Ohio Democrat and Republican residents who support the ACA according to KHIP or OHIP relative to the MRP subgroup estimates. We find that the correlation between the MRP subgroup estimates and the estimates from KHIP is 0.82 (very strong) for Republicans and 0.39 (moderate) for Democrats, if the most dissimilar estimate in 2010 is excluded. MRP does a worse job for Democrats than Republicans in both states; this may have to do with the fact that multilevel regression pulls state averages toward the national mean in order to increase reliability. This suggests that it will be more difficult to obtain statistical significance in dynamic analyses that use these estimates, providing a more stringent test of the hypotheses outlined in this article.5
Partisans Favoring the ACA in Kentucky and Ohio Relative to MRP Subgroup Estimates
Descriptive Analyses of ACA Partisan Polarization in the States
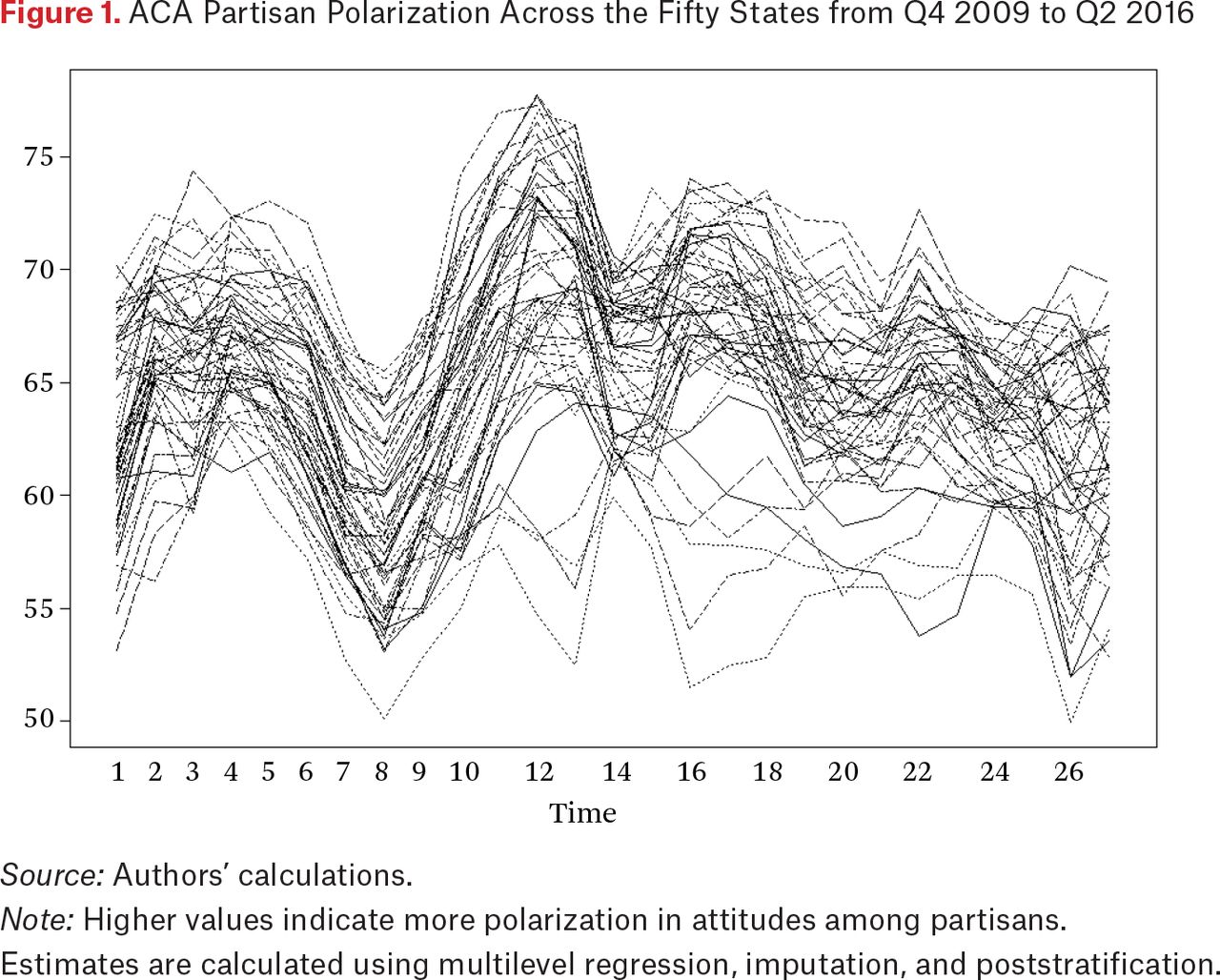
We quantify partisan polarization on the ACA—our dependent variable—by taking the difference in ACA favorability between the Democrats and the Republicans. Higher values indicate higher polarization in ACA attitudes. Figure 1 shows variation both across states and time in partisan polarization toward the ACA. ANOVA analyses confirm significant variation at both units of analyses with 55 percent of the variance within states and 45 percent of the variance between states.
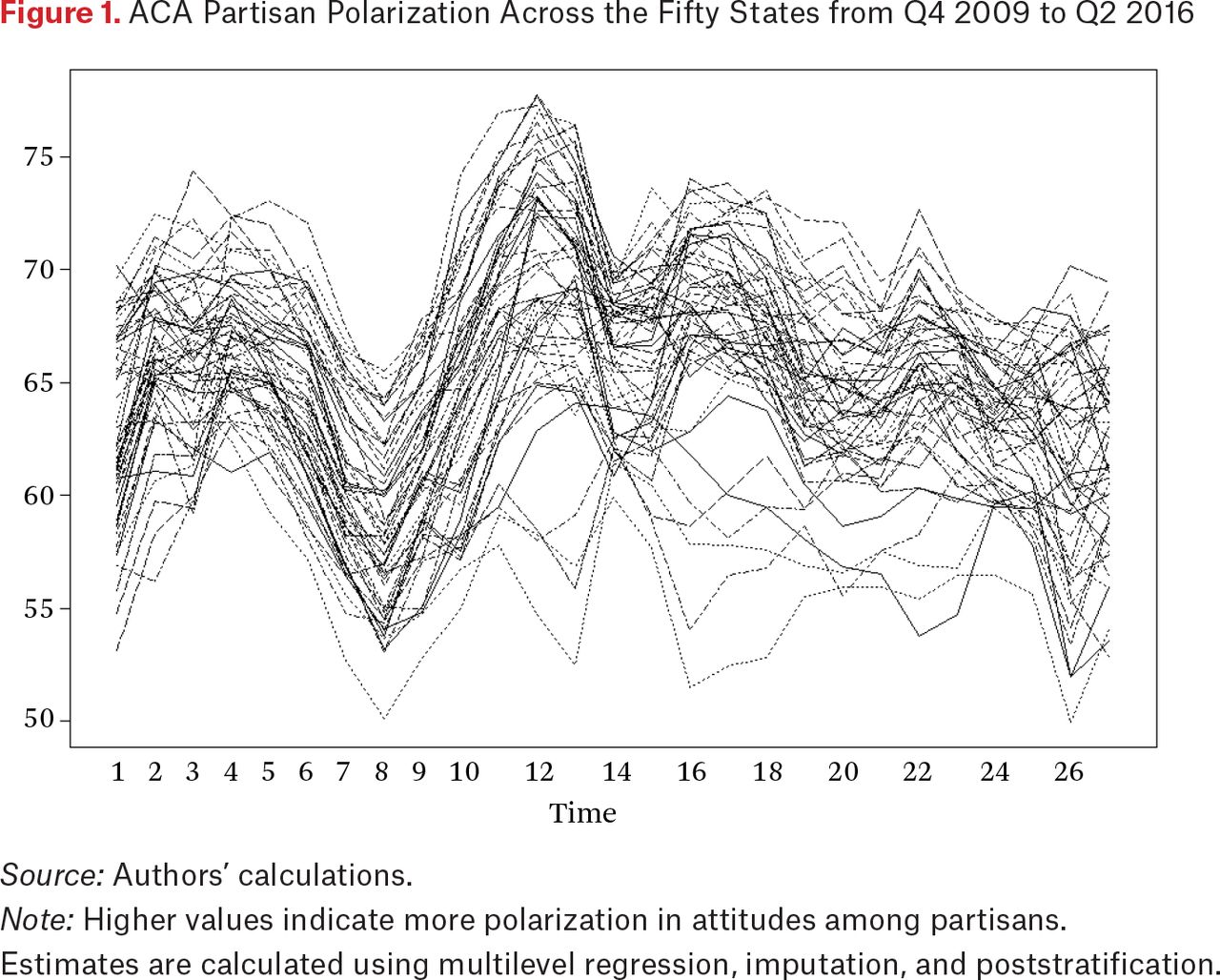
ACA Partisan Polarization Across the Fifty States from Q4 2009 to Q2 2016
Source: Authors’ calculations.
Note: Higher values indicate more polarization in attitudes among partisans. Estimates are calculated using multilevel regression, imputation, and poststratification.
Substantively, figure 1 shows significant partisan polarization toward the ACA. At no point is any state below the 50 percent mark, indicating large differences across partisans in their favorability toward the ACA. At the same time, several states have much higher levels of partisan ACA polarization than others. New Mexico exhibits the highest level of partisan polarization, in the third quarter of 2012, for instance, and West Virginia the lowest, in the first quarter of 2016. To explore the demographic correlates of partisan polarization toward the ACA, we present an exploratory random-effects regression. We include region, percentage of state residents who are uninsured, household median income, natural log of population, percentage of state residents who are nonwhite, and time. These variables are obtained from the Census Bureau’s ACS one-year estimates. Even though our unit of analysis is state by quarter, the majority of our independent variables vary at the year level. Given the time dependence of the outcome variable, we also include a lagged dependent variable. Results are presented in table 2.
Random-Effects Regression of Partisan Polarization
Table 2 shows that partisan polarization toward the ACA is unrelated to several of the traditional demographic state variables that are of importance to scholars of state politics. Partisan polarization toward the ACA is not statistically related to region, the percentage of uninsured state residents, or state population. According to the model, state partisan polarization to the ACA is higher in states that have a higher percentage of nonwhite residents; it is also higher in states that have a higher household median income, which is consistent with the findings of Elizabeth Rigby and Gerald Wright (2013). Finally, the model in table 2 shows that partisan polarization has generally declined from the fourth quarter in 2009 to the second quarter in 2016.
CAPTURING THE STATE PARTISAN POLICY ENVIRONMENT
We are interested not only in descriptively exploring the state correlates of ACA partisan polarization, but also in how state policy decisions influence public opinion. Recall that we expect the gap between partisans’ evaluations of the ACA to be larger in aligned partisan environments (states where Democrats have pushed for implementation and Republicans have opposed it) and smaller in misaligned partisan environments (states where Republicans have backed implementation).
This requires time-varying indicators of the stated policy positions of key state partisan elites. In this study, we focus on governors. As the most visible state public officials and the most important to implementation of both the exchanges and Medicaid expansion, governors have the greatest potential to move public opinion with their stated positions. Starting with the policy briefs provided by the Kaiser Family Foundation, we tasked trained research assistants with verifying (through media reports) when governors in each state made clear public announcements of their preferred policy for both the exchanges and Medicaid expansion. For the exchanges, we created dichotomous variables for gubernatorial announcements in favor of state-run exchanges (the most “pro-ACA” implementation option, implemented in eleven states and the District of Columbia), federally run exchanges (which amount to a refusal to commit state resources to implementation, implemented in twenty-eight states), and state-federal “partnership” exchanges (a hybrid model between the two, implemented in the remaining eleven states). For Medicaid expansion, we created a single variable capturing whether the governor announced support for any variant of Medicaid expansion, whether the full expansion envisioned under the original law, or the compromised Section 1115 waiver versions negotiated by most Republican-controlled states that went forward with expansion.6
Our theoretical framework assumes that a high-profile announcement by a key partisan figure such as a governor creates a lasting change in the political environment in a state. Thus, in states where the governor expressed support for a particular policy option, the relevant variable is coded 0 for all quarters before the announcement and 1 for the quarter in which the announcement was made and in all quarters thereafter. For each of these variables, the baseline is a low-information environment in which the governor has not yet taken a position on implementation.
Because we expect the effect of cues to differ based on the partisanship of the governor, we also include a dichotomous variable indicating whether the governor in each state was a Republican in each quarter. By interacting this variable with the announcement variables, we are able to differentiate between aligned and misaligned partisan policy environments. The constituent terms for the state exchange, partnership exchange, and Medicaid expansion variables indicate that a Democratic governor has made the announcement in question (aligned partisan policy environment). The interaction terms of each of those variables with the Republican governor variable identifies the difference between that scenario and one in which a Republican governor made the same announcement (misaligned partisan policy environment). The interaction term of the Republican governor variable and the federal exchange announcement variable identifies another aligned partisan policy environment.7
Control Variables and Fixed Effects
We include a number of time-varying control variables. The most important of these is a one-quarter lag of our ACA polarization measure, because we expect some degree of “stickiness” in public attitudes about the law. We also control for whether and when the state filed or joined an anti-ACA lawsuit, most of which were eventually consolidated into the NFIB v. Sebelius case.8 The decision to file or join such a suit is itself a signal of a state government’s intentions toward the ACA, albeit a more ambiguous one, given that in many states the initiator was not the governor but the state attorney general. Because anti-ACA and Republican state governments were more likely to file or join lawsuits, failing to account for this variable could bias the polarizing effect of governors’ later announcements on Medicaid expansion or the exchanges. This variable is coded similarly to the announcement variables, in that it is equal to 0 until the quarter the state filed or joined a suit, and 1 thereafter.
We also control for state economic and demographic characteristics and trends using data from the American Community Survey. Specifically, we include estimates of population (logged), the percentage of the population that lacks health insurance, the median household income (in thousands), and the nonwhite percentages of the population given that state race and diversity have been shown to play a role in ACA politics (per Grogan and Park 2018). Because the ACS provides only annual estimates, we “smooth” changes in these variables across the quarters of each year.
Of course, this set of control variables is unlikely to properly account for the heterogeneity between states. In addition to random-effects models that examine variation both within and between states, we also specify state fixed-effects models that focus strictly on within-state variation.
We also account for time in two ways. In some models, we include a linear time trend to account for secular trends, ACA polarization having declined somewhat over time. We also include a specification with quarter fixed effects, which should account for both long-term trends and any state-level responses to national events.
RESULTS
Table 3 displays the results of our analysis of state-level ACA polarization. Because our dependent variable is continuous, we use linear regression with both random and fixed effects to account for the panel structure of the data. The regression includes clustered robust standard errors to account for both heteroskedasticity and within-cluster serial correlation (Arellano 1987), the latter of which would also be mitigated by the lagged dependent variable. The results suggest some qualified support for our expectations. First, the constituent term for state exchange announcement is associated with a statistically significant increase in partisan polarization on the ACA, but only in the random-effects specifications. These results suggest a Democratic governor announcing support for a state exchange (establishing an aligned partisan policy environment) increases the gap between Republicans and Democrats by about half of a percentage point in the short run. Although this is a modest effect, the strong positive effect and statistical significance of the lagged dependent variable indicate that the polarization gap between states where governors announced support for a state-based exchange and those where they did not should grow over time, if the random-effects result is valid. In the fixed-effects models, this apparent effect vanishes. In another scenario indicating an aligned partisan policy environment, a Democratic announcement of support for Medicaid expansion (identified by the Medicaid expansion announcement constituent term), we do not see evidence of a polarizing effect in any specification.
State-Level Polarization on the Affordable Care Act
Because we are interested in the effects of misaligned as well as aligned partisan policy environments, we now turn to the variables indicating a Republican governor announcing support for a state exchange and Medicaid expansion. Again, the results are mixed. We see no evidence in any specification that a Republican governor announcing support for a state exchange reduced polarization. On the other hand, the Republican governor Medicaid expansion variable is consistently negatively signed, as predicted, and is statistically significant at the p < .1 level in the fixed-effects specifications. When a Republican governor announces support for expansion, the fixed-effects models predict that polarization will decrease about three-quarters to 1 full percentage point in the short term, an effect that should grow over time due to the significant effect of the lagged dependent variable. The fact that his effect is stronger in the fixed-effects than the random-effects specification suggests that a Republican governor announcing support for Medicaid expansion has a stronger effect on public opinion over time within a state than it does in a comparison of states where this did and did not occur.
We also note a puzzling finding—in three of the four specifications, the increase in polarization when a Republican governor announces support for a partnership exchange is statistically significant. Given the ambiguous political signal sent by the partnership exchanges, and that we did not predict such an effect ex ante, we are reluctant to speculate about the mechanisms that might be driving this apparent correlation.
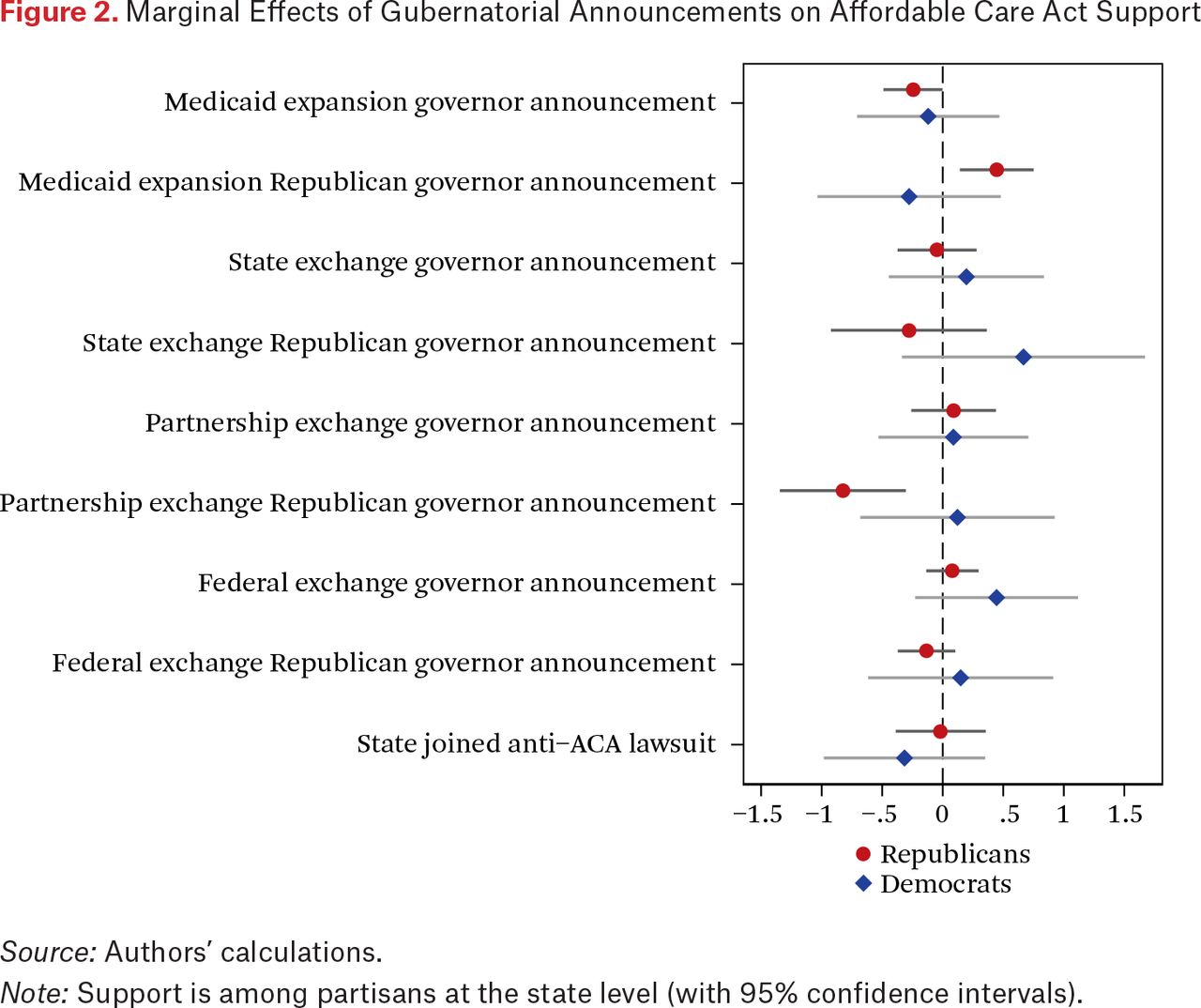
Because the findings of our polarization analyses are ambiguous, we go one step further in table 4 by treating Republican support and Democratic support for the ACA as separate dependent variables. For the sake of space, we use the most rigorous of our specifications, with state and quarter fixed effects, for both dependent variables. We also display the coefficients with 95 percent confidence intervals in figure 2. The results provide some more support for our theoretical expectations in the case of Medicaid expansion: among Republicans, a Democratic governor announcing support for Medicaid expansion decreases ACA support by a quarter of a percentage point, while a Republican governor backing expansion increases support by a little less than half a percentage point (p < .05 in both cases). In short, Republicans appear to respond to both “aligned” and “misaligned” partisan policy environments as the theory predicts, at least where Medicaid expansion is concerned. For Democrats, we see no effects that come close to statistical significance.
State-Level Support for the Affordable Care Act
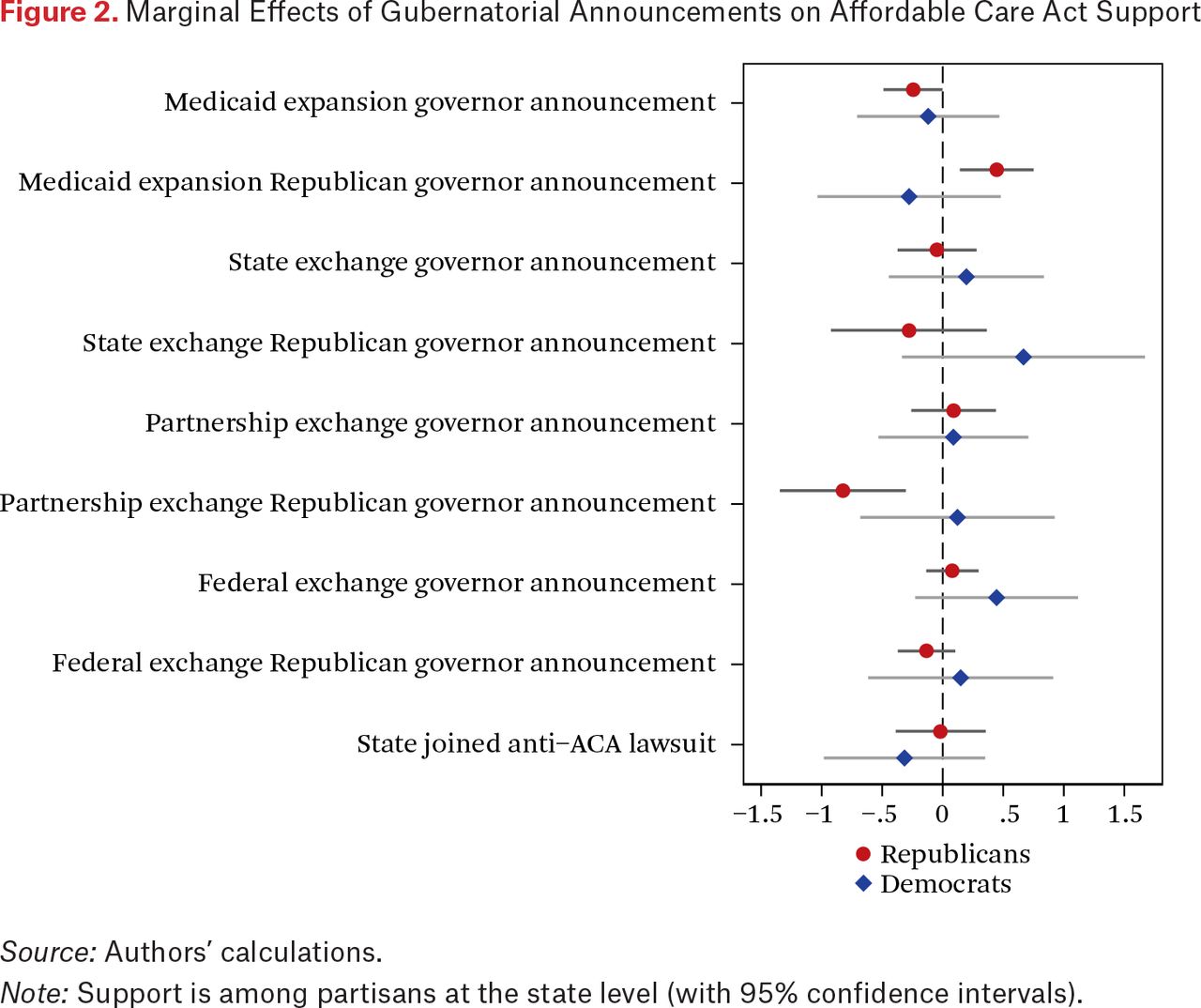
Marginal Effects of Gubernatorial Announcements on Affordable Care Act Support
Source: Authors’ calculations.
Note: Support is among partisans at the state level (with 95% confidence intervals).
For the exchanges, we do not observe any significant effects in any announcement scenario, aside from the significant negative effect for Republicans of a Republican governor supporting a partnership exchange, which accords with the puzzling polarization finding.
In terms of magnitude, what statistically significant effects we do observe are modest. Although the lagged dependent variable suggests these effects will compound over time, even the long-run effects would be in the range of a few percentage points, not enough to bridge the formidable gap between the parties, which approached 80 percentage points in some states. The relevance of these effects will differ with the size of partisan subgroups; a percentage point bump in support from Republicans in Alabama, where Republicans dominate, means more than a similar bump in Connecticut where they are relatively scarce.
LIMITATIONS
Although our over-time measures provide unique data on how state partisans change their opinions of the ACA, our results are mixed. We encourage scholars to continue exploring how preferences respond to shifting political contexts in a polarized, federated polity. Yet we also are cognizant of the limitations of our analyses.
The MRP approach is limited in a number of ways, which also limits the confidence of our inferences. Although when combined with a three quarter moving average it helps solve issues of reliability, our estimates still vary in reliability in connection with state population (see Pacheco 2012). In addition, we are likely smoothing over short-term shifts in ACA opinion that occur month by month. As important, MRP may not be the best approach to studying policy feedback effects. As Devin Caughey and Christopher Warshaw (2019) note, coefficients are generally biased toward zero in models where MRP is used to measure the dependent variable (see also Clinton and Sances 2018). This bias may account for the small or nonexistent effects of state policy decisions on ACA polarization that we observe in our paper. If there is more error in our estimates of Democratic opinion, as our validation exercise in table 2 suggests, this bias toward null findings is likely greater in the Democratic subgroup, which is consistent with the results in table 4 and figure 2.
Last is an issue of endogeneity. We do not claim that governors are unmoved movers in this story—it is likely that many or most of them considered public opinion about the ACA in their states before staking out their positions on the law. The findings of Richard Fording and Dana Patton (2020) on governors’ decisions to pursue Medicaid work requirements suggest that implementation decisions respond to public opinion. By including lagged dependent variables and state fixed effects, we are able to partially address this concern; both approaches narrowly focus the analysis on quarter-to-quarter change and make it more likely that the coefficients for the announcement variables reflect causal effects rather than artifacts of past public opinion.9 Because the measures themselves are imperfect, however, we cannot completely rule out the endogeneity issue. Governors and their advisors have access to information (including internal polling) and insights about the political climate in their states that go beyond the simple survey questions we use in our analyses.
DISCUSSION AND CONCLUSION
Do state political elites shape mass polarization in their states by taking positions on policy? Our results suggest that they may, in some circumstances. In the case of the ACA, a highly polarized topic nationally, Republicans seem to respond negatively when a Democratic governor announces support for Medicaid expansion, and positively when a Republican governor does so. Democrats appear unmoved in either scenario, but these Republican subgroup effects could have a modest effect on the overall level of polarization. Some evidence also indicates that a Democratic governor supporting a state-based health insurance exchange may increase polarization, but this effect does not hold up to the most rigorous specifications. Overall, we find scant evidence that governors announcing their positions on the exchanges drove opinion in either partisan subgroup.
Given these results, we assert a basic “proof of concept” for the notion that state-level partisan political elites may shape polarization on policy issues in their states. The overall picture, though, is one of fairly consistent national polarization on the ACA. If governors play a role in this story, they do so at the margins. It may be that the statements and actions of governors or other state-level figures have larger effects on the opinions of partisan subgroups on issues that are less polarized at the national level.
Although this study focuses on the role of governors’ announcements in shaping such opinions, this is just one possible application. Future work should incorporate other relevant actors, such as state legislators, and explore the possibility of policy feedbacks following implementation. State-level public opinion also has explanatory power as an independent variable, as Fording and Patton (2020) show in this issue, and using MRP to estimate opinion among partisan subgroups offers the potential for a more complete view of whether and how officials respond to different constituents.
FOOTNOTES
↵1. This includes Arkansas, Kentucky, and New Hampshire, but court orders in these states have halted implementation of work requirements. In addition, several states have received approval for work requirements but have delayed implementation, in some cases due to administrative and political hurdles (Arizona, Utah, Wisconsin, and Michigan). Most generally, decisions about work requirements are in flux, messier, occur at a later point in the policy process than we focus on in this article, and operate based on a distinct set of processes that are in part affected by the patterns we study but also driven by separate processes. For insights on this, see Fording and Patton 2020. For the most recent developments, see Kaiser Family Foundation, “Medicaid Waiver Tracker: Approved and Pending Section 1115 Waivers by State,” December 20, 2019, https://www.kff.org/medicaid/issue-brief/medicaid-waiver-tracker-approved-and-pending-section-1115-waivers-by-state (accessed December 27, 2019).
↵2. These states expanded in the context of Section 1115 demonstration waivers (Grogan, Singer, and Jones 2017) that included relatively restrictive provisions such as premiums, increased copayments, the reduction of retroactive eligibility and later in the policy process—work requirements (for insights on the political processes that drive such provisions, which are distinct from what we explore, see Fording and Patton 2020).
↵3. Legislators in Utah and Idaho subsequently took measures to attenuate the reach and generosity of these expansions.
↵4. The sample size for KHIP varies across time, but averages around 1,500 with statewide estimates being accurate to plus or minus 2.5 percent (for more information, see http://www.healthy-ky.org). The sample size for the 2011 OHIP survey is 908; statewide estimates will be accurate to plus or minus 3.3 percent (for more information, see “Ohio Health Issues Poll,” https://www.interactforhealth.org/whats-new/category/ohio-health-issues-poll).
↵5. In addition to overall polarization, we also analyze the opinions of each partisan subgroup separately. The analysis of Republican opinion is not affected by the lower reliability of the Democratic measure.
↵6. Although it would be interesting to distinguish between statements in favor of full implementation and those in favor of waiver implementation, too few Republican governors supported the former to allow for comparisons.
↵7. Each interaction term is coded based solely on the partisanship of the announcing governor. For example, in Massachusetts, Democratic Governor Deval Patrick’s announcement of support for Medicaid expansion is coded 0 for the Republican governor and Medicaid expansion interaction term even after Patrick left office in the first quarter of 2015 and Republican Governor Charlie Baker took over.
↵8. National Federation of Independent Business v. Sebelius, 567 U.S. 519 (2012).
↵9. Lagged dependent variables may bias the coefficients of other independent variables in random- and fixed-effects models toward zero, militating against finding significant effects. Excluding the lagged dependent variables from the analyses reported here generally leads to larger and more significant effects that are consistent with our hypotheses (for example, larger effects for both Democratic and Republican Medicaid expansion announcements, most of which are statistically significant at the p < .01 level), and some that are not (for example, the counterintuitive findings for the partnership exchange announcements grow stronger). In this article, we err on the side of caution and report the more conservative lagged dependent variable estimates.
- © 2020 Russell Sage Foundation. Pacheco, Julianna, Jake Haselswerdt, and Jamila Michener. 2020. “The Affordable Care Act and Polarization in the United States.” RSF: The Russell Sage Foundation Journal of the Social Sciences 6(2): 114–30. DOI: 10.7758/RSF.2020.6.2.05. The authors thank the participants of the Russell Sage Foundation’s conference, The Social, Political, and Economic Effects of the Affordable Care Act, for their thoughtful comments and suggestions. We also thank Jacob Authement for research assistance. Direct correspondence to: Julianna Pacheco at julianna-pacheco{at}uiowa.edu, 341 SH, University of Iowa, Iowa City, IA 52242.
Open Access Policy: RSF: The Russell Sage Foundation Journal of the Social Sciences is an open access journal. This article is published under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.
REFERENCES
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.