
Abstract
Attention-deficit/hyperactivity disorder (ADHD) is America’s most common childhood disorder. Although an ADHD diagnosis can bring positives, recent research uncovers potential negatives associated with diagnosis. This study examines understudied racial-ethnic heterogeneity in the relationships between an early elementary school ADHD diagnosis—with or without medication treatment—and children’s future perceived self-competence, teacher-rated school behaviors, and parent-rated educational expectations. Findings are consistent with the notion that diagnosis can trigger racialized patterns of stigma. That is, relative to undiagnosed matches of the same social class and regardless of medication use, diagnosed Black children demonstrate worse teacher-rated school behaviors, diagnosed White children report poorer perceived self-competence, and parents of diagnosed Hispanic children report poorer educational expectations. Racialized patterns of stigma might amplify the consequences of negative-ability stereotyping on Black children, academic pressure on White children, and mental health stigma on Hispanic children. Findings also highlight the challenges of identification posed by differential unobserved selection into diagnosis.
This study examines previously understudied patterns of racial-ethnic variation in the association between a diagnosis of attention-deficit/hyperactivity disorder (ADHD)—with or without accompanying medication treatment—and children’s later socioemotional well-being. ADHD is the most common neurodevelopmental disorder of American childhood. ADHD is characterized by difficulty paying attention or controlling impulsive behaviors or both. As of 2016, 2.4 million (9.6 percent) children ages six to eleven and 3.3 million (13.6 percent) American adolescents ages twelve to seventeen were diagnosed with ADHD (Xu et al. 2018). Rates of diagnosis vary across race-ethnicity, from 12.0 percent among White children to 12.8 percent of Black children and 6.1 percent of Hispanic children (Xu et al. 2018).
An ADHD diagnosis can be a key disruptive event of childhood. Diagnosis can bring both positives, such as access to medications to help control behavior problems and educational services or accommodations (Molina et al. 2009; Swanson, Baler, and Volkow 2010), and some negatives, such as stigma (Link et al. 2001). Studies show that, when one compares the later test scores and well-being of diagnosed children and their otherwise observably comparable undiagnosed matches, the downsides can outweigh the benefits—even with receipt of medication following diagnosis (Owens 2020a; Owens and Jackson 2017). These negatives are found to be especially salient for diagnosed children who had less severe pre-diagnosis ADHD-related behaviors and for children from high socioeconomic backgrounds (Owens 2020a, 2020b). Yet research has not investigated racial-ethnic heterogeneity in these documented net negative marginal relationships between diagnosis and later child outcomes.1
Considering racial-ethnic heterogeneity in the marginal relationship between ADHD diagnosis in early elementary school and later child well-being is important for both substantive and theoretical reasons. Substantively, such heterogeneity could have important implications for inequality since it is unclear whether diagnosis serves as a social and academic support or a further stigma among racial-ethnic minority children, who already face a range of barriers to academic success and socioemotional well-being at school. Theoretically, exploring racial-ethnic variation also provides a valuable case for unpacking a tension in the literature highlighted by Florencia Torche, Jason Fletcher, and Jennie Brand (2024, this issue) for understanding how disruptive events can have heterogeneous effects across different subpopulations. On the one hand, Torche and colleagues point to a large body of social scientific evidence on the compounding effects of cumulative disadvantage for child well-being. Yet, another strand of studies the authors discuss suggests that when “negatively assessed events [are] more normative . . . the stigma associated with them becomes less severe”—thus potentially ameliorating the impacts of these negatively assessed events on later child well-being.
These diverging theories have direct application to the case of racial-ethnic heterogeneity in the marginal relationship between ADHD diagnosis and later child well-being. Much research documents the large negative effects of racial discrimination on the well-being of Black children (Ferguson 2001; Okonofua and Eberhardt 2015; Owens 2022). At the same time, other studies shed light on the resilience of Black children and communities in the face of structural and interpersonal discrimination, partly owing to the normalization of such negatively assessed experiences and thus the lesser stigma associated with them (Burt, Lei, and Simons 2017; Myers and Taylor 1998).
These bodies of research can lead to differing predictions about the marginal relationship between diagnosis and later well-being for Black versus White children, each relative to their undiagnosed counterparts. One possibility is that diagnosis will compound the already negative effects of racial discrimination for Black children. Another is that the diagnosis will ameliorate the negative effects of prior experiences of discrimination among Black children.
To help make sense of these differing predictions, we propose that both theories can be true depending on the outcome (and its rater) of interest. When teachers’ negative-ability stereotyping of Black students (Ferguson 2001) is compounded by teachers’ diagnostic stigma (Owens 2020a), we predict that teachers will also more negatively rate the behaviors of diagnosed Black children versus diagnosed White children, contributing to cumulative disadvantage. Crucially, medication receipt following diagnosis may not fully offset—and may in some cases even heighten—the potential negatives associated with diagnosis. Although medication is designed to help control the behaviors of ADHD (Swanson, Baler, and Volkow 2010), it may increase the visibility—and thus the stigma—of the diagnosis, including among teachers.
By contrast, when it comes to children’s perceived self-competence, diagnosed Black children (and in some cases, Black parents) may exhibit greater resilience than diagnosed White children, including when receiving medication, given the former’s greater likelihood of having previously normalized the experience of being negative labeled, such as through racial stereotyping. We focus on subjective ratings of well-being as a starting point rather than other relevant outcomes such as academic achievement, grade retention, and educational attainment. We suspect that well-being is more proximately related to the psychological processes associated with diagnosis and thus more likely to produce the largest relationships.
Much less is known about relationships between diagnosis and later well-being among Hispanic children in general, and thus between Hispanic versus Black and Hispanic versus White children. However, several studies do find substantial mental health stigma and resistance to the use of ADHD medications on the part of Hispanic families (Cummings et al. 2017; Dosreis et al. 2003; Perry, Hatton, and Kendall 2005). In our study, we include Hispanic children and parents as an important but largely overlooked group in this area of research.
To isolate processes associated with race-ethnicity rather than with family social class given the high correlation between race and class in the United States, we compare diagnosed and undiagnosed matches of the same social class. Research discussed by Torche, Fletcher, and Brand (2024, this issue) highlights social class-based mechanisms that advantage White children—who are on average more socioeconomically advantaged than Black and Hispanic children. By contrast, we focus on the psychological processes that can shape the experiences of ADHD diagnosis for children of a given race-ethnicity across the socioeconomic spectrum. To do so, we use the Early Childhood Longitudinal Study–Kindergarten Cohort of 2010–11 (ECLS-K: 2011). These data include a rich set of pre-diagnosis measures—including lagged outcomes and important child, family, and school context characteristics—which improve matching and limit nonrandom selection on observables.
To explore these potentially heterogeneous relationships requires first contending with the issue of differential selection into diagnosis (and potential medication treatment) on observed and unobserved characteristics. Research emphasizes differential selection into diagnosis by family socioeconomic status and the strictness of school sanctions for poor performance on state-mandated achievement tests—each of which are correlated with race-ethnicity (Fulton, Scheffler, and Hinshaw 2015; King, Jennings, and Fletcher 2014). Black and Hispanic children are respectively 69 percent and 50 percent less likely than White children to be diagnosed even net of differences in family social class, pre-diagnosis behavioral problems, prior academic achievement, family structure, child sex, health insurance coverage or noncoverage, native language, and region (Morgan et al. 2013). Conditional on diagnosis, selection into medication treatment is also nonrandom: Black and Hispanic children are likewise 65 percent and 47 percent respectively less likely to receive medication treatment following diagnosis than White children, net of controls (Morgan et al. 2013). Although a randomized controlled trial would be the ideal method for addressing nonrandom selection into diagnosis and treatment, the experimental gold standard is not feasible in this context (for example, it would be unethical to withhold diagnosis). Yet researchers cannot stop at simply documenting differential selection processes given the important potential implications of diagnosis. We must also examine—albeit descriptively—if and how the benefits and consequences associated with ADHD diagnosis balance out differently by child race-ethnicity.
ASSOCIATIONS BETWEEN ADHD DIAGNOSIS AND FUTURE WELL-BEING
A diagnosis of ADHD can bring potential benefits for children. Diagnosis can connect children to medications that improve attention and concentration (Swanson, Baler, and Volkow 2010) and to educational accommodations and services (for example, extra time on tests and individualized assignments) that can help improve future academic and social success (Molina et al. 2009). Diagnosis can also offer a medical explanation for children’s inattention and hyperactivity that “legitimizes” parents’ struggles with their children’s behaviors and increases parent-school collaboration (Blum 2015).
However, an ADHD diagnosis may also be associated with some drawbacks, such as negative stereotyping and labeling (Link et al. 1989), stigma (Goffman 1963), experiences of disgrace (Francis 2012), and lower reading and math scores compared to undiagnosed peers (Owens and Jackson 2017). Diagnosed children may also experience increased scrutiny and lower expectations from teachers compared to undiagnosed peers (Eisenberg and Schneider 2007).
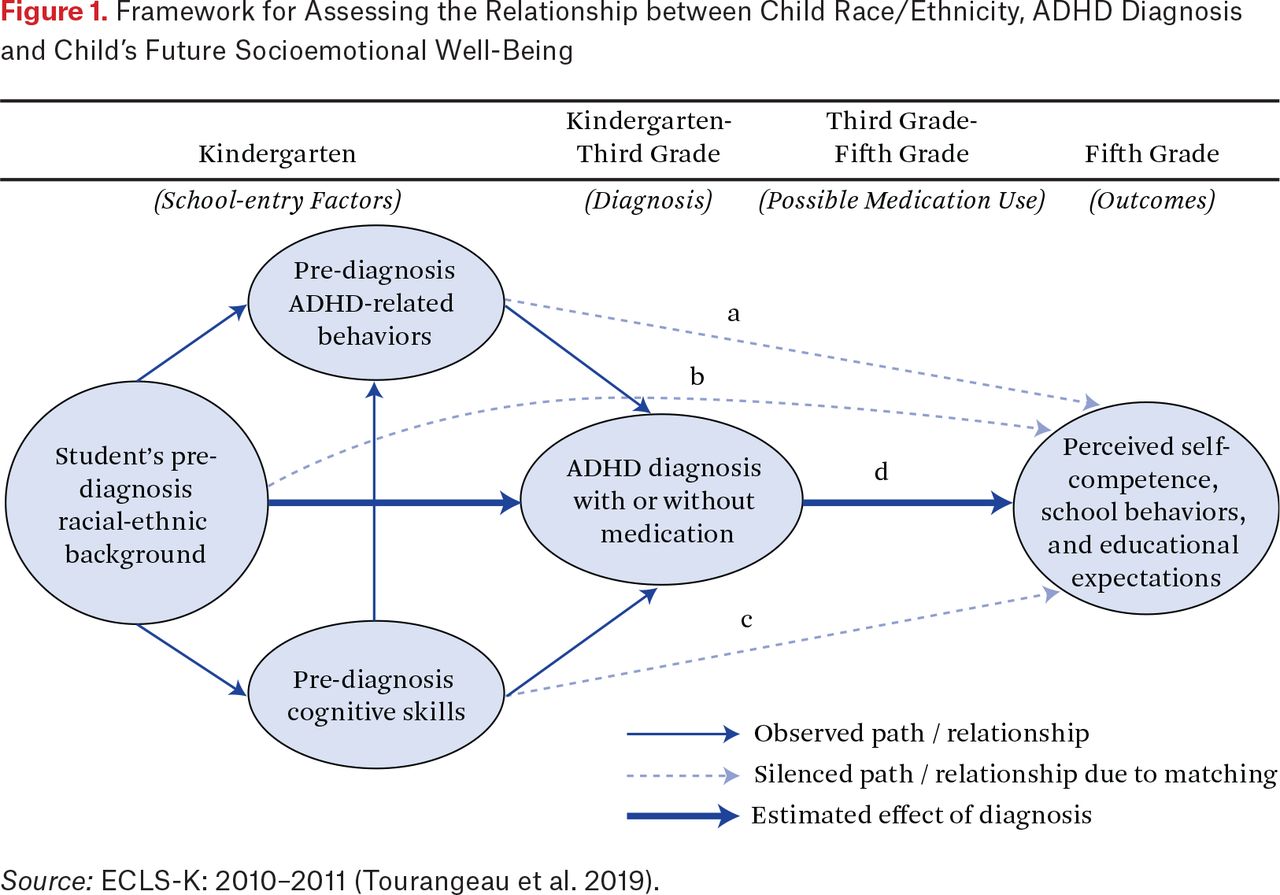
Most research on children with ADHD has compared children with high versus low levels of ADHD-related behavioral problems (path A of figure 1). This work found that children with more severe ADHD-related behavioral problems experience poorer social, educational, and health outcomes (Fletcher 2014; Fletcher and Wolfe 2008). By contrast, only a few studies have begun to describe the association between the ADHD diagnosis itself (path D of figure 1) and children’s later socioemotional well-being, net of pre-diagnosis teacher- and parent-reported behavioral problems (path A) and other observed academic and sociodemographic factors (paths B-C) (Owens 2020a; Owens and Jackson 2017). Although these analyses cannot control for all potential differences between diagnosed and potentially medicated children and their undiagnosed counterparts, documenting these associations begins to unpack the broader interrelated social, psychological, and medical factors that can underlie the social meaning of an elementary school ADHD diagnosis.

Framework for Assessing the Relationship between Child Race/Ethnicity, ADHD Diagnosis and Child’s Future Socioemotional Well-Being
Source: ECLS-K: 2010–2011 (Tourangeau et al. 2019).
Potentially Heterogeneous Associations
The potential positive and negative social, psychological, and medical factors associated with a childhood diagnosis of ADHD may balance out differently among children with differing status characteristics. Only one study to date examines such variation in the relationship between an ADHD diagnosis and children’s later well-being, in that case based on family socioeconomic status (SES) (Owens 2020b). That study compares diagnosed children and their otherwise comparable undiagnosed counterparts who had the same pre-diagnostic behavioral problems and other observed academic and demographic characteristics. The author descriptively finds that, relative to undiagnosed matches, “diagnosed and medicated” upper- and middle-SES children exhibit significantly poorer perceived self-competence, by 0.41 points (0.53 standard deviations, or SD) and 0.22 points (0.28 SD), respectively. Relative to their undiagnosed matches, diagnosed and medicated upper- and middle-SES children are also rated worse on teacher-rated positive learning behaviors by 0.31 to 0.46 points (0.43 to 0.67 SD) and on negative externalizing problems, by roughly 0.18 points (0.31 SD) each. But diagnosed and medicated low-SES children do not show significant differences relative to their undiagnosed matches. Although these estimates are for diagnosed and medicated children of a given social class, patterns are generally similar among same-SES diagnosed and unmedicated children. Crucially, Owens (2020b) focuses on the relationship between social class privilege and children’s well-being but does not examine variation along other important social-demographic factors, such as race-ethnicity.
In the present study, we use the same analytic technique as Owens (2020b) but examine racial-ethnic variation in the relationships between ADHD diagnosis, with or without subsequent medication use, and later child well-being—net of differences in family social class. We hypothesize that these relationships may vary between diagnosed and undiagnosed children of the same social class based on both child race-ethnicity and the outcome (and its rater) of interest.
Within schools, qualitative research finds that an ADHD diagnosis among Black children is likely to be seen as a sign of intellectual deficiency and negative ability (Harry and Klingner 2007). Consistent with the theory of cumulative disadvantage, this negative perception may be compounded by the reality that, in many schools, administrators and teachers are less culturally responsive to the instructional needs of Black students (Ferguson 2001; Owens 2022; Shedd 2015). Many even hold explicit and implicit racial biases toward Black and Hispanic students (Starck et al. 2020; Welch et al. 2011). By contrast, among White students, a diagnosis is more likely to be viewed as signaling an unmet need—a call for additional support in order for the child to reach their full potential (Blanchett 2010; Blum 2015). As a result, regardless of medication receipt, diagnosed Black students may be even more likely to be defined as low achievers with inherently limited school potential, whereas diagnosed White students may be more likely to be seen as having greater school potential despite low school achievement (Blum 2015). Thus:
Hypothesis 1: Regardless of medication receipt, teachers will rate the behaviors of diagnosed Black children more negatively than those of diagnosed White children, each relative to their otherwise similar undiagnosed counterparts of the same social class.
By contrast, for children’s self-perceptions, the normativity of being negatively assessed (such as from teachers’ race-based negative ability stereotyping) may increase Black children’s resilience and reduce any stigma associated with their diagnosis relative to White children (Owens 2022; Rios 2017; Starck et al. 2020). White children, on the other hand, are less likely to have previously experienced negative-ability stereotyping but are more likely to have experienced academic pressure from young ages (Hinshaw and Scheffler 2014; King, Jennings, and Fletcher 2014; Russell 2011). As a result, White children may be more likely to internalize expectations for high achievement to come “effortlessly” (Mueller and Abrutyn 2016). In this context, an ADHD diagnosis, even with medication treatment, may be perceived by White children as a sign of having failed to meet these high academic expectations, thus leading to lower perceived self-competence. In addition, diagnosed and medicated White children are more likely to concurrently use at least two classes of psychotropic medications (Comer, Olfson, and Mojtabai 2010). Polypharmacy may also potentially increase negative side effects and lower self-image as compared to diagnosed and medicated minority children (Bussing and Winterstein 2012). Taken together:
Hypothesis 2: With or without medication treatment following diagnosis, diagnosed White children will experience lower perceived self-competence than diagnosed Black children, each relative to their otherwise comparable undiagnosed counterparts of the same social class.
Parents’ educational expectations for their children may also vary across racial-ethnic groups, reflecting differing social meanings underlying ADHD diagnosis. For Black parents, studies suggest that diagnosis can be seen as reflecting the school’s beliefs about their child as having a fundamental behavioral or intellectual deficiency and thus using the diagnosis to “displace” their child from school learning opportunities (Blum 2015; Harry and Klingner 2007). As a result, Black parents may experience skepticism toward—and resist—the diagnosis by maintaining equally high expectations of their diagnosed child. Alternatively, Black parents may view the diagnosis as reflecting the added barriers their child will face at school and thus lower their academic expectations for their child in turn. For Hispanic parents, similar competing processes may be at play, but the greater average presence of stigma toward mental health diagnoses and treatment within Hispanic immigrant communities may further lower Hispanic parents’ educational expectations relative to Black parents (Cummings et al. 2017; Dosreis et al. 2003; Ji et al. 2018). On the other hand, given the greater average academic pressure from young ages within White communities, White parents may be more likely to view diagnosis and medication treatment as a route for their child to gain additional academic supports (Hinshaw and Scheffler 2014; King, Jennings, and Fletcher 2014; Schwarz 2017). Thus:
Hypothesis 3a: Hispanic parents will report lower educational expectations for diagnosed children relative to their undiagnosed matches of the same social class, regardless of medication receipt following diagnosis.
Hypothesis 3b: Regardless of medication receipt, Hispanic parents’ educational expectations for their diagnosed children will be lower than White and Black parents’ expectations for their diagnosed children; Black parents will report either comparable or lower expectations as White parents, also regardless of medication.
DATA AND METHODS
To explore racial-ethnic heterogeneity in the patterns of association between ADHD diagnosis and future child well-being, we use the restricted-use ECLS-K:2011, an initially nationally representative sample of kindergarteners in 2010 followed through fifth grade. Our longitudinal sample includes the 8,700 children who remained in the study through fifth grade, were not missing data on the outcomes, diagnosis, or race-ethnicity, and were either diagnosed (N = 820) or plausible undiagnosed matches who had comparable early ADHD-related behavioral problems despite not being diagnosed (N = 7,880). Sample restrictions, sample trimming, and attrition are detailed in the online appendix; cell sizes are rounded to the nearest 10 per the restricted-use data agreement.2
These data offer several substantial strengths for examining the role of ADHD diagnosis (path D of figure 1)—defined as the average difference in the outcomes of diagnosed and otherwise comparable undiagnosed children who had the same propensities to be diagnosed. First, given the dramatic rise in diagnosed ADHD prevalence in recent decades, these data offer the most updated estimates of social class differences in the marginal effects of ADHD diagnosis on future well-being among U.S. children. Second, given that ADHD diagnoses require functional impairment from inattention or hyperactivity-impulsivity in at least two settings (American Psychiatric Association 2013), both teachers and parents rate children’s behaviors. Moreover, ratings occur in children’s naturalistic settings (school and home), independent of diagnostic evaluation and less subject to reporting bias than might be the case if these ratings were collected when parents or teachers were making the case for or against the child’s needing diagnosis.
Third, these reports capture the core behaviors of ADHD—inattention and hyperactivity-impulsivity—as well as conduct or oppositional defiance disorder and depression, ADHD’s two most common comorbid conditions (Hinshaw and Scheffler 2014). Although imperfect, items resemble those used in ADHD screeners such as the Connor’s, SNAP-IV, and DSM-IV (Currie and Stabile 2006; Swanson, Baler, and Volkow 2010). Fourth, these ratings are provided for all sample children, including the roughly 91 percent of children with developmentally normal behaviors who are never diagnosed with ADHD, thus providing a wide range of suitable undiagnosed “matches.” Table A.1 presents counts of children by race-ethnicity and diagnosis and medication treatment status. Finally, behavior ratings are collected in the wave before diagnosis, offering an advantage to measuring pre-diagnosis behaviors in a static period. Because behavior problems typically decrease with age, exclusively measuring behaviors in kindergarten would understate behavior problems for children whose problems worsen after school entry and before diagnosis. Conversely, drawing exclusively on third grade measures (the end of the diagnosis observation period) could introduce reverse causality if diagnosis prompts behavior change.
We use multiple imputation of twenty datasets to address item-missingness on matching variables for the implicated 17 percent (N = 1,740/9,990) of the longitudinal sample (Rubin 2004). Item-missingness is more common among children who are Black, uninsured, have low baseline academic achievement, have high baseline behavioral problems, or come from low-SES, single-mother families. ADHD diagnosis and the outcomes are included in the imputation equation but children originally missing on these measures are excluded from all analyses (following Von Hippel 2007).
Analytic Strategy: Doubly Robust Matching for Sample Balance
To contend with the fact that neither diagnosis nor subsequent medication receipt are randomly assigned, matching techniques are used to help address key observed confounders that may influence both diagnosis-medication treatment and the outcomes. In addition to race-ethnicity (Morgan et al. 2013), potential confounders include differences in diagnosed and undiagnosed children’s social class; insurance coverage status; pre-diagnosis ADHD-related behaviors; baseline academic achievement; sex; age-for-grade, whether they are older or younger than their classmates (Layton et al. 2018); internalizing behavior problem score, because internalizing is a common comorbidity of ADHD; parents’ concerted cultivation child-rearing styles; kindergarten classroom type; average peer classroom behavior, which might shape reference group effects; the presence of strict state-mandated consequential educational accountability, given that strict accountability standards create pressure for ADHD diagnosis (Bokhari and Schneider 2011; King, Jennings, and Fletcher 2014); and region of residence, given well-established regional differences in ADHD diagnostic prevalence (Hinshaw and Scheffler 2014). If unobserved, differences along these child, family, classroom-school, and state-region factors may influence both diagnosis and the outcomes and yield biased estimates of the marginal effect of diagnosis, both with or without subsequent medication receipt.
To address some of these potential observable confounders, standard multiple regression techniques would introduce controls to adjust for consequential observable differences between diagnosed and undiagnosed children. However, standard controls within ordinary least squares (OLS) regressions may not be adequate if overlap, or balance, is insufficient in the distributions of characteristics between diagnosed and undiagnosed children (Imbens and Rubin 2015). Thus researchers have turned to matching techniques to help achieve sample balance on key observed variables for which OLS models may yield estimates that lack sample support or balance (Gangl 2010).
This study uses two types of matching to obtain estimates that are “doubly robust” to confounding between diagnosed and undiagnosed children on observed variables: coarsened exact matching (CEM) and propensity score matching (PSM) (Stuart et al. 2009). First, we use the CEM package in Stata 14 to pre-process the data and ensure that diagnosed and undiagnosed children are “exact matches” on three theoretically motivated characteristics on which differences in diagnosis and future well-being are well established: race-ethnicity (three groups); quartile of pre-diagnosis behavioral problems based on parent- and teacher-rated subscales for inattentive or hyperactive-impulsive behavioral type (sixteen groups); and child sex (two groups).
Temporarily “coarsening” the continuous variables for social class and pre-diagnosis ADHD-related behaviors into the categories means that matching occurs within the ninety-six groups (3x16x2 = 96). Figure A.1 highlights substantial overlap in the pre-diagnosis ADHD-related behaviors distributions of both diagnosed and undiagnosed children. With 9.4 percent of sample children ages four through ten diagnosed with ADHD, 90.5 percent of children are not diagnosed, offering many potential undiagnosed matches who nonetheless had the same propensity to be diagnosed. Both groups’ pre-diagnosis behavioral ratings span the full range from never to almost always. All 820 diagnosed children are successfully matched to otherwise comparable undiagnosed children. By contrast, three hundred undiagnosed children (3.3 percent) are implausible matches because their ADHD behaviors fall below those of diagnosed children. They are trimmed to improve sample balance and efficiency and reduce bias (Iacus, King, and Porro 2011).
Nonetheless, CEM is limited by the number of exact matching dimensions it can accommodate. Even after CEM, additional differences are observable between diagnosed and undiagnosed children within coarsened groups (Imbens and Rubin 2015). Thus, as detailed in the appendix, PSM is used after CEM to help address additional possible confounding by achieving balance between diagnosed and undiagnosed children on thirty-four child, family, classroom, and state or region variables included in the PSM equation: all seven behavioral measures and the twenty-seven other variables detailed in table 1. The doubly robust combination of CEM followed by PSM does not remove the risk of selection on unobserved variables and measurement error.
Descriptive Statistics for All Variables Used in the Analyses, by Race-Ethnicity (N = 8,700)
Models
To examine racially and ethnically heterogeneous associations between an early elementary school ADHD diagnosis and future child well-being, we match diagnosed children with their undiagnosed counterparts who are otherwise comparable on observed characteristics within racial-ethnic group. To investigate whether medication treatment status following diagnosis further internally moderates these associations, we additionally match diagnosed and undiagnosed children within racial-ethnic group based on whether they received medication treatment following diagnosis. Balance statistics are presented in table A.2. Sample stratification by child race-ethnicity occurs after CEM but before PSM (Stuart et al. 2009).
Key Measures
Table 1 provides summary statistics for all variables used in the analyses: child perceived self-competence, teacher-rated school behaviors, and parent-rated educational expectations from fifth grade (“outcomes”). Teacher-rated frequency of “positive approaches to learning,” or attentiveness, task persistence, eagerness to learn, learning independence, flexibility, and organization is a subscale from the social rating scale (Tourangeau et al. 2019). Child-reported self-competence is from the following (reverse-coded) self-description questionnaire items: worry about doing well in school, finishing homework, and taking tests; struggle to finish schoolwork; and feeling ashamed about mistakes at school. Both teacher and child ratings were reported from 0 = rarely to 3 = always. Ratings were averaged across items to construct the final scales. Parent-rated educational expectations come from an item asking parents about how far they expect their child to go in school, with responses ranging from 0 = less than high school, 1 = high school diploma, 2 = attend two-year college, 3 = complete two-year college, 4 = bachelor’s degree, 5 = master’s degree or equivalent, 6 = PhD, MD, JD, Other advanced degree.
ADHD diagnosis between kindergarten-third grade (primary predictor) was identified when the parent answered yes to all three of these questions in a given wave: (1) Has the child been evaluated by a professional in response to a problem in paying attention, learning, behaving, or in activity level? (2) Has the child received a diagnosis by this professional? (3) Was the diagnosis for ADHD, ADD, or hyperactivity? (see Morgan et al. 2013; Tourangeau et al. 2019). Children whose parents answered no to any item were coded as “not diagnosed with ADHD.” Diagnosis was confirmed using parent report of “year of first [ADD/ADHD] diagnosis.” Children first diagnosed with ADHD after third grade were coded as undiagnosed.
Medication treatment receipt between third and fifth grades (moderator) comes from parent report of whether the child was taking medication to control their behavior in third or fifth grade. In fifth grade, 90 percent of children receiving medication were taking one of three ADHD medications, based on parent report: Ritalin, Adderall, or Concerta.
Child race-ethnicity from kindergarten (predictor-moderator) comes from the primary caregiver’s report of the child’s race-ethnicity: Black, not Hispanic; Hispanic; White, not Hispanic; Asian, not Hispanic; Native Hawaiian or Other Pacific Islander, not Hispanic; American Indian or Alaska Native, not Hispanic; or Two or More Races. Dummy variables were constructed for Black, Hispanic, White, and Other, and Other was dropped prior to analyses given the theoretical focus of this study.
Pre-diagnosis ADHD-related behavioral problems from first grade or wave prior to diagnosis (behavior problems or ADHD behaviors; predictors). Teacher and parent behavioral ratings are taken as shortly before diagnosis as possible, usually earlier in the same school year or the previous spring to help guard against inappropriate matches resulting from possible increases in behavior problems after school entry and before diagnosis. Undiagnosed children’s behavior problems came from first grade, nearly the midpoint of the kindergarten through third grade diagnostic observation period, given that behavior problems among typically developing children decrease with age. Nevertheless, estimates change by less than 10 percent when all behaviors are measured in kindergarten. ADHD-specific items were separated from the externalizing problems and positive approaches to learning scales of the psychometrically validated social rating scale (following Owens 2020b), but sensitivity analyses using the complete externalizing behaviors and approaches to learning scales yielded virtually identical results (Tourangeau et al. 2019). The inattentive subscale included two items measuring attention and concentration skills, which were reverse coded so that higher values reflected more problems. The hyperactive subscale included two items on impulsiveness (acts without thinking) and restlessness (overly active, cannot sit still). Subscales averaged across their items and ranged from 0 = rarely to 3 = always (–1 to 2 after sample mean centering).
Commonly co-occurring pre-diagnosis behavioral problems from first grade or wave prior to diagnosis (predictors). The oppositional defiant disorder (ODD) subscale involves separate teacher and parent reports of seven behaviors: arguing, fighting, getting angry, throwing tantrums, ease in joining in play (reverse-coded), ability to make and keep friends (reverse-coded), and positive interactions with peers (reverse-coded). The internalizing problems scale includes eight items measuring sadness, loneliness, and anxiety (for details, see Tourangeau et al. 2019). Timing of measurement and item ranges are the same with those for ADHD-related behavioral problems.
Other predictors in PSM equation from kindergarten. To help ensure that diagnosed and undiagnosed children are as comparable as possible on observed characteristics, thirty-four key child, family, classroom, and school state-region context covariates from table 1 are included in the PSM. These include pre-diagnosis academic achievement, family social class (a composite, standardized scale of female and male guardians’ educational attainment, household income, and occupational prestige; the bottom quartile representing lower-SES, the middle two quartiles middle-SES, and the top quartile upper-SES [per Tourangeau et al. 2019]), average classroom behavior (teacher-rated, from 0 = extremely poorly behaved to 4 = extremely well behaved), whether the child’s school is in a state with strict consequential accountability standards using the dummy variable from King, Jennings, and Fletcher (2014), and the child’s region of residence.
RESULTS
The primary goals of this analysis are to examine any racial-ethnic heterogeneity in the patterns of association between an early elementary school ADHD diagnosis and children’s fifth-grade perceived self-competence, teacher-reported school behaviors, and parent education expectations; and to explore the role of medication treatment receipt following diagnosis in further moderating any of these racial-ethnic differences in the associations between diagnosis and later well-being.
Descriptive Differences by Child Race-Ethnicity
To understand racial-ethnic differences in the relationships between an ADHD diagnosis and later child well-being in the ECLS-K: 2010–11 sample, table 1 presents descriptive statistics for all variables used in the analysis by child race-ethnicity. Consistent with prior research (Owens and McLanahan 2020), both Hispanic children and, in particular, Black children have significantly poorer outcomes on average than White children on three of the four fifth-grade outcomes of interest—two teacher-rated school behaviors and child-rated perceived self-competence (two-tailed tests). Specifically, Black and Hispanic children exhibit significantly lower positive approaches to learning scores in the fifth grade than their White counterparts. Black children exhibit significantly higher negative externalizing behavioral problems than both their White and Hispanic counterparts. Likewise, both Black and Hispanic children on average report significantly lower self-competence than their White peers. By contrast, both Black and Hispanic parents hold significantly higher educational expectations for their children on average than do White parents, with Hispanic parents holding even higher expectations than Black parents.
Consistent with previously documented prevalence rates (Xu et al. 2018), rates of ADHD diagnosis between kindergarten and third grade are highest among Black children (14 percent) followed by White children (11 percent). Hispanic children are significantly less likely to receive an ADHD diagnosis (6 percent) than either Black or White children. Similarly, absolute rates of medication receipt following diagnosis are highest among Black children (8 percent) and White children (7 percent), and lowest among Hispanic children (3 percent). However, when it comes to proportions receiving medication of those diagnosed, Whites have the highest rates of medication use (63 percent of those diagnosed), followed by Blacks (57 percent of those diagnosed), and then Hispanics (50 percent of those diagnosed).
Racial-Ethnic Variation in the Associations Between an Early Elementary School ADHD Diagnosis and Later Child Well-Being
To test for racial-ethnic variation in the patterns of association between an early elementary school ADHD diagnosis and later child well-being, table 2 presents estimates of differences in the future outcomes between diagnosed children and their undiagnosed counterparts of the same racial-ethnic group who had comparable propensities for diagnosis but were not diagnosed. Estimates are irrespective of medication use. On teacher-rated school behaviors, results are partially consistent with hypothesis 1. An ADHD diagnosis is associated with significantly poorer later teacher-rated positive approaches to learning in fifth grade among both Black and White children (models 1 and 3). The magnitude of the relationship, however, is 62 percent smaller among White children than among Black children. Diagnosed Black children are rated 0.29 points (0.29/0.79 = 0.37 SD) significantly lower on positive learning-related behaviors than their undiagnosed matches (model 1), whereas diagnosed White children are rated a significant 0.11 points lower (0.11/0.76 = 0.14 SD, model 3). Moreover, consistent with hypothesis 1, White children do not differ significantly on negative externalizing problems from their same-race undiagnosed matches (model 6) in fifth grade, whereas Black children are rated 0.23 points (0.23/0.65 = 0.35 SD) significantly worse than their undiagnosed matches (model 4). Diagnosed Hispanic children do not score significantly differently from their undiagnosed matches on either positive approaches to learning (model 2) or negative externalizing problems (model 5).
Relationships Between an Early Elementary School ADHD Diagnosis and Future Teacher-Rated Social and Academic Behaviors, Child Perceived Self-Competence, and Parent Educational Expectations in Fifth Grade, By Child Race-Ethnicity (N = 8,700)
When it comes to child perceived self-competence, results are consistent with hypothesis 2. Estimates shown in models 7 through 9 of table 2 reveal that an early elementary ADHD diagnosis is correlated with significantly lower perceived self-competence in fifth grade, but only among White children. White children exhibit 0.22 points (0.22/0.75 = 0.29 SD) significantly lower perceived self-competence than their undiagnosed matches (model 9). As predicted, this 0.22 points is significantly lower than that among diagnosed Black children. Neither diagnosed Black nor diagnosed Hispanic children score significantly differently from their undiagnosed matches (models 7 and 8).
Finally, in terms of parent educational expectations, results are consistent with hypothesis 3a. Estimates shown in models 10 through 12 reveal that an ADHD diagnosis is associated with significantly lower education expectations, but only for Hispanic children. Hispanic parents report 0.32 points (0.32/1.31 = 0.24 SD) statistically significantly lower education expectations for diagnosed children than Hispanic parents of undiagnosed children do (model 11). Also consistent with hypothesis 3b, Hispanic parents report significantly lower educational expectations for their children than White parents do of their children (–0.32 points versus –0.07 points). Findings are also directionally consistent with lower expectations among Hispanic than Black parents (also –0.32 points versus –0.07 points), but the difference does not reach statistical significance due to the larger standard error around the estimate for Black parents.
Altogether, results in table 2 reveal that the relationships between an early ADHD diagnosis and later well-being differ based on both child race-ethnicity and the outcome-rater under consideration. Consistent with literature suggesting that behavioral diagnoses may function as mechanisms of social control that further marginalize Black children at school (Blanchett 2010; Harry and Klingner 2007), teachers evaluate diagnosed Black children’s behaviors more poorly than they do either diagnosed White or diagnosed Hispanic children. By contrast, only diagnosed White children report lower perceived self-competence relative to their undiagnosed matches, perhaps because they are least likely to have previously experienced negative labeling. Finally, on parent education expectations, Hispanic parents report lowered expectations for diagnosed children, perhaps owing to greater mental health stigma in Hispanic communities (Perry, Hatton, and Kendall 2005). We return to this point in the discussion.
Differing Associations Between an ADHD Diagnosis and Later Well-Being, by Child Race-Ethnicity and Medication Treatment Status Following Diagnosis
Table 3 further distinguishes between children who did versus did not receive medication following diagnosis, relative to undiagnosed matches. Consistent with hypothesis 1, diagnosis with medication is associated with significantly lower teacher- and parent-rated outcomes among Black children. Relative to undiagnosed matches, diagnosed and medicated Black children appear 0.20 points (0.25 SD) lower on positive learning behaviors, 0.18 points (0.23 SD) higher on externalizing problems, and 0.21 points (0.15 SD) lower on parent education expectations (models 1, 4, and 10). Diagnosed and unmedicated Black children are also rated 0.44 points (0.56 SD) lower than undiagnosed matches on positive learning behaviors and 0.32 points (0.42 SD) higher on externalizing problems than undiagnosed matches (model 1 and 4). Although teachers likewise rate diagnosed and unmedicated White children significantly worse than undiagnosed matches on positive learning behaviors (by 0.14 points, or 0.18 SD, per model 3) and on negative externalizing problems (by 0.12 points, or 0.19 SD, per model 6), these estimates are 68 percent and 63 percent smaller than those for diagnosed and unmedicated Black children. The difference between diagnosed and unmedicated Black and diagnosed and unmedicated White children reaches statistical significance (model 1 versus model 3).
Average Relationships Between an ADHD Diagnosis and Future Teacher-Rated Social and Academic Behaviors, Child Perceived Self-Competence, and Parent Educational Expectations in Fifth Grade, by Child Race-Ethnicity and Medication Treatment Status Following Diagnosis (N = 8,700)
By contrast, and consistent with hypothesis 2, neither diagnosed and medicated nor diagnosed and unmedicated Black or Hispanic children report significantly lower perceived self-competence relative to their undiagnosed matches, whereas both groups of White children do. This difference in difference reaches statistical significance for diagnosed and medicated White children versus their Black counterparts (model 7 versus model 9). Specifically, diagnosed and medicated White children fall a significant 0.25 points (0.33 SD) lower on perceived self-competence than their undiagnosed matches (model 7), whereas diagnosed and unmedicated White children fall 0.14 points (0.19 SD) lower (model 9).
When it comes to parent educational expectations, results are also consistent with hypothesis 3a. Parents of diagnosed and medicated Hispanic children report significantly lower educational expectations (by 0.45 points, or 0.34 SD) than their undiagnosed matches (model 11). Diagnosed and unmedicated Hispanic children likewise appear worse on parent education expectations by 0.30 points (0.23 SD) relative to undiagnosed matches (model 11). When it comes to comparisons across racial-ethnic groups, results are directionally consistent with hypothesis 3b, even though diagnosed and medicated Hispanic children do not fall significantly lower than either their Black or White counterparts. Parents of diagnosed and medicated Black and White children also report significantly lower educational expectations than undiagnosed matches (by roughly 0.20 points, or 0.18 SD, each), but this estimated magnitude is approximately 50 percent that among Hispanic parents (models 10 and 12). When it comes to parents of diagnosed and unmedicated children, results are significant and consistent with hypothesis 3b: Hispanic parents report significantly lower expectations for their children than both Black and White parents. In fact, Black parents actually hold 0.27 points (0.20 SD) higher expectations for their children than their undiagnosed matches (model 10); parents of diagnosed and unmedicated White children do not hold different expectations than their undiagnosed matches (model 12).
Overall, these results are consistent with the idea that medication can help control ADHD-related behavioral problems without necessarily addressing potential downsides, such as labeling and stigma. Labeling and stigma can vary based on both the child’s race-ethnicity and the outcome under consideration. Even when medicated, diagnostic associations are consistent with the possibility of negative disability labeling by teachers toward Black (but not White) children. Although diagnosed and unmedicated White children do experience worse teacher-rated behavioral ratings than undiagnosed matches, consistent with some teacher-based negative disability labeling, these estimates are one-third the size as among diagnosed and unmedicated Black children.
Nonetheless, both diagnosed and medicated and diagnosed and unmedicated White children experience lowered perceived self-competence. For Black children, despite lower behavioral ratings by teachers, neither diagnosed and medicated nor diagnosed and unmedicated Black children experience lowered perceived self-competence than their undiagnosed matches, and diagnosed and unmedicated Black children also do not experience lowered parent expectations. Although diagnosed and medicated Black children and diagnosed and medicated White do experience lowered parent expectations relative to undiagnosed matches, these lower expectations are half as large as those experienced by Hispanic children.
Contextualizing the Magnitude of Diagnostic Relationships Across Race-Ethnicity
To contextualize the magnitude of these estimates, we note that the variation we document by race-ethnicity is comparable with previously documented variation by social class (Owens 2020b). For example, diagnosed Black children experience 0.29 points (0.37 SD) lower teacher-rated positive approaches to learning, similar to the 0.36 points (0.52 SD) previously documented among upper- and middle-SES children (Owens 2020b). Likewise, diagnosed White children report 0.22 points (0.28 SD) lower perceived self-competence, similar to the 0.25 to 0.27 points (0.32 to 0.34 SD) lower perceived self-competence previously documented among upper- and middle-SES children (Owens 2020b).
Our estimates are also comparable to other studies examining similar outcomes, but different predictors. For instance, we found that diagnosed and unmedicated Black children are rated 0.42 SD worse on teacher-rated externalizing behaviors than their undiagnosed matches. Comparably, Adam Wright, Michael Gottfried, and Vi-Nhuan Le (2017) find that teacher-student race matching was associated with 0.40 SD lower teacher-rated externalizing behaviors for Black children. Jennifer Jennings and Thomas DiPrete (2010) find that moving a student from a below-average to an above-average kindergarten teacher could increase students’ social and behavioral skills by 0.28 SD.
Our estimates include as potential undiagnosed matches those children who develop ADHD later in childhood. Doing so likely underestimates diagnostic relationships because these children may have had undiagnosed ADHD during our diagnostic observation period and were thus more similar to our diagnosed children than other undiagnosed matches.
A Descriptive Look at Overall Winners and Losers Based on Predicted Scores
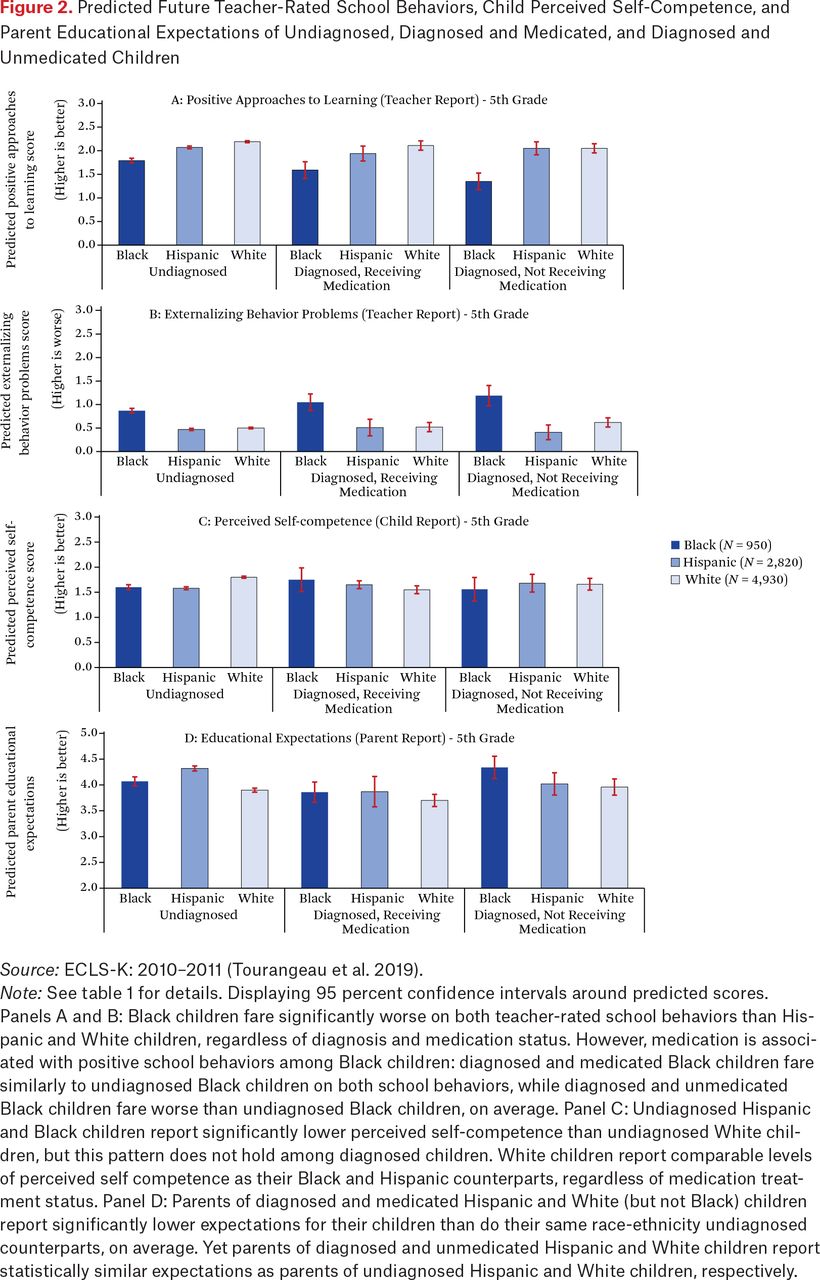
Figure 2 shows how the marginal relationships between diagnosis and later well-being shape overall predicted scores on each outcome, by race-ethnicity, diagnostic status, and medication treatment status following diagnosis. Figure 2 summarizes three main descriptive findings. First, Black children fare significantly worse overall on both future teacher-rated school behaviors than both Hispanic children and White children, irrespective of diagnosis and medication treatment status (figure 2, panels A and B). However, medication is associated with positive school behaviors among Black children: diagnosed and medicated Black children fare similarly to undiagnosed Black children on both school behaviors, whereas diagnosed and unmedicated Black children fare worse than undiagnosed Black children, on average.

Predicted Future Teacher-Rated School Behaviors, Child Perceived Self-Competence, and Parent Educational Expectations of Undiagnosed, Diagnosed and Medicated, and Diagnosed and Unmedicated Children
Source: ECLS-K: 2010–2011 (Tourangeau et al. 2019).
Note: See table 1 for details. Displaying 95 percent confidence intervals around predicted scores.
Panels A and B: Black children fare significantly worse on both teacher-rated school behaviors than Hispanic and White children, regardless of diagnosis and medication status. However, medication is associated with positive school behaviors among Black children: diagnosed and medicated Black children fare similarly to undiagnosed Black children on both school behaviors, while diagnosed and unmedicated Black children fare worse than undiagnosed Black children, on average. Panel C: Undiagnosed Hispanic and Black children report significantly lower perceived self-competence than undiagnosed White children, but this pattern does not hold among diagnosed children. White children report comparable levels of perceived self competence as their Black and Hispanic counterparts, regardless of medication treatment status. Panel D: Parents of diagnosed and medicated Hispanic and White (but not Black) children report significantly lower expectations for their children than do their same race-ethnicity undiagnosed counterparts, on average. Yet parents of diagnosed and unmedicated Hispanic and White children report statistically similar expectations as parents of undiagnosed Hispanic and White children, respectively.
Second, on perceived self-competence, undiagnosed Black and Hispanic children report significantly lower perceived self-competence than undiagnosed White children (figure 2, panel C). Consistent with the negative relationship between diagnosis and perceived self-competence among White children, this pattern does not hold among diagnosed children. Diagnosed White children report statistically similar levels of perceived self-competence as their diagnosed Black and Hispanic counterparts, regardless of medication treatment status.
Third, on education expectations, parents of diagnosed and medicated Hispanic and White children report significantly lower expectations for their children than their same race-ethnicity undiagnosed counterparts do (figure 2, panel D). Yet parents of diagnosed and unmedicated Hispanic children and of diagnosed and unmedicated White children report statistically similar expectations as parents of undiagnosed Hispanic and White children, respectively. Furthermore, parents of diagnosed Black children do not report different expectations from parents of undiagnosed Black children, regardless of medication treatment status.
Sensitivity Analyses
Research documents the underdiagnosis and lesser medication receipt of Black and Hispanic children relative to White children net of observed characteristics (Morgan et al. 2013), highlighting the risk of unobserved selection into diagnosis and potential medication receipt. To gauge how large the unobserved effect would need to be to nullify our findings, we conducted the bounding analysis proposed by Kenneth Frank and his colleagues (2013). Results summarized in table A.3 reveal that, depending on the group and outcome under consideration, estimates would have to be biased by between 2 percent on the low end, for teacher ratings of diagnosed and medicated Black children’s externalizing problems, to 69 percent on the high end, for diagnosed and medicated White children’s self-competence, to invalidate our findings. Estimates are most sensitive to the risk of unobserved confounding for diagnosed and medicated Black children, likely because the relatively small pool of (N = 820) potential undiagnosed Black matches yields somewhat poorer quality matches even with these best available data. We discuss implications in the discussion.
Moreover, differential selection into diagnosis may partly reflect differential selection into evaluation based on unobservable factors within race-ethnicity. To help address this potential differential selection, supplemental matching analyses restricted the pool of potential undiagnosed matches to those children who were evaluated by a medical professional for a learning difficulty but who were not ultimately diagnosed with ADHD. These supplemental analyses contained only 20.3 percent of children (N = 1,770) in the full sample. With the exception that the lower perceived self-competence of diagnosed White children is no longer statistically significant, results lend confidence that unobserved selection into evaluation does not drive results (see the appendix and table A.4). Finally, to test the robustness of our results to alternate specifications of our outcomes, we examine—and find—that the same pattern of results when using binary outcomes (0 when the teacher or child reports 0 or 1 and 1 when they report 2 or 3), per table A.5.
DISCUSSION
This study advances our understanding of racial-ethnic heterogeneity in patterns of association between ADHD diagnosis, medication treatment, and future child well-being. We build on prior research on the benefits and drawbacks associated with ADHD diagnosis and potential medication use (Owens 2020b) by examining how positives and negatives can balance out differently for Black, Hispanic, and White children. Because the experimental gold standard is unfeasible in this context (for example, it is unethical to withhold diagnoses), we match children who are diagnosed (and subsequently medicated or unmedicated) with same race-ethnicity undiagnosed children who are otherwise comparable on observed characteristics, including social class. Although documenting correlations, matching helps us disentangle racial-ethnic differences in the role of ADHD diagnosis (with or without treatment) apart from underlying ADHD-related behaviors.
The study reveals three findings. First, an early elementary school ADHD diagnosis is associated with poorer future teacher-rated school behaviors among Black children; the magnitude is over twice as large among Black as among White children. This finding persists regardless of medication treatment status. Second, although a diagnosis is not consistently associated with poorer teacher-rated school behaviors among White children, White children uniquely report poorer child-perceived self-competence regardless of medication status. Third, even though diagnosed Hispanic children do not on average experience poorer teacher-rated behaviors or lower perceived self-competence than their undiagnosed matches, diagnosis is uniquely associated with lower educational expectations among Hispanic parents regardless of children’s medication treatment status following diagnosis.
When it comes to teachers’ behavioral ratings of Black children, teachers may perceive the diagnosis with or without medication as reinforcing expectations of poor behaviors or lack of academic commitment, themselves grounded in negative stereotypes (Okonofua and Eberhardt 2015; Owens 2022). By contrast, although diagnosed and unmedicated White children are also rated more poorly by teachers than their undiagnosed matches (whereas diagnosed and medicated White children are not), this relationship is half as large as among Black children. This may be because diagnosed and unmedicated White children are uniquely seen as having an unmet need for medication (Blanchett 2010; Ong-Dean 2006). These findings are consistent with the notion that diagnosis among Black children may function as a mechanism of social control within schools. But, for White children, diagnosis may be seen as a sign that additional support is needed for them to reach their full potential.
Hispanic parents may report lower educational expectations for their diagnosed versus undiagnosed children, regardless of medication status, for several reasons—even though neither teachers nor children themselves respectively report poorer ratings on school behaviors and self-competence. One possibility is that Hispanic parents have lesser knowledge of ADHD and lesser familiarity with how to help overcome associated schooling barriers, for example, due to possible language barriers (Rothe 2005). Hispanic parents’ lesser knowledge combined with mental health stigma (Pescosolido et al. 2008) may lead to larger negative associations between diagnosis and education expectations. Medication may reinforce the visibility of the mental health label among Hispanic parents, further lowering their expectations.
Our study also has a number of limitations and areas for future extension. First, race-based diagnostic reporting error among parents is possible. For example, White parents are more likely than other parents to seek out an ADHD diagnosis and medication treatment (Bussing et al. 2003; Morgan et al. 2013). Although research using the ECLS-K data considers parents to be valid and reliable reporters of ADHD diagnosis, symptoms, and medication receipt (Cumming et al. 2022; Morgan et al. 2013; Mulligan et al. 2019), research has not examined potential race-based diagnostic reporting error. Second, the associations we uncover may result from race-ethnicity-specific reference group effects, for example, if Black children have worse-behaved classmates than White children, leading teachers of Black children to be more agitated by minor deviations from desired behavior. However, these results appear even among teachers with comparable ratings of average classroom behavior.
Third, the associations we uncover should be treated as suggestive in nature and interpreted in light of potential unobserved racial-ethnic differences in selection into diagnosis and potential medication receipt. Differential unobserved selection may occur, for example, because our measures of ADHD-related behaviors (and internalizing and oppositional-defiant behaviors) do not align perfectly with those used by clinicians, and do not capture other clinical aspects beyond behavioral frequency, such as intensity or duration. Fourth, our results also extend only to the young children diagnosed between kindergarten and third grade. Fifth, these data also lack a direct measure of ADHD-related stigma or internalized shame. However, results are consistent with previous findings that ADHD diagnosis is associated with stigma and negative labeling among diagnosed children (Pescosolido et al. 2008). Future qualitative or experimental research should investigate this mechanism directly. In addition, future research should examine the relationships between an ADHD diagnosis and future test score outcomes by child race-ethnicity. Finally, for researchers, this study highlights the challenges of identifying diagnostic effects given the need to address differential selection into diagnosis despite the infeasibility of a randomized controlled trial in this context.
Taken together, our findings carry important implications for racial-ethnic disparities in children’s future mental health and well-being. The differing associations between ADHD diagnosis (with versus without medication) and later well-being by child race-ethnicity may reflect different underlying social meanings of diagnosis, what we refer to as racialized patterns of stigma. When it comes to diagnosed White children’s lower perceived self-competence, diagnosis with or without medication use may be seen as a sign that the child has failed to meet expectations for seemingly effortless academic excellence (Mueller and Abrutyn 2016). Although we cannot be sure of underlying mechanisms, that even diagnosed and medicated White children report poorer perceived self-competence is consistent with theories of negative diagnostic labeling: even when medication effectively controls ADHD-related behaviors, medication is not designed to address labeling. Diagnosed Black and Hispanic children do not report lowered perceived self-competence regardless of medication receipt, perhaps owing to their greater resilience given prior exposure to the realities of racial-ethnic discrimination and negative ability stereotyping.
FOOTNOTES
↵1. By marginal relationships, we refer to the role of the diagnosis rather than that of the pre-diagnosis ADHD-related behaviors and associated factors themselves. We examine the association between diagnosis and later well-being by comparing diagnosed and undiagnosed children who were otherwise comparable on pre-diagnosis ADHD-related behaviors, test scores, and other observed characteristics.
↵2. See online appendix (https://www.rsfjournal.org/content/10/1/205/tab-supplemental).
- © 2024 Russell Sage Foundation. Owens, Jayanti, and Xinyan Cao. 2024. “Racial-Ethnic Heterogeneity in the Relationship Between an Early Elementary School ADHD Diagnosis and Later Child Well-Being.” RSF: The Russell Sage Foundation Journal of the Social Sciences 10(1): 205–28. DOI: 10.7758/RSF.2024.10.1.09. The authors thank Florencia Torche, Jennie Brand, Jason Fletcher, Suzanne Nichols, Nick Papageorge, and the participants of the Russell Sage Foundation workshop, the William T. Grant Foundation Scholars Award (PI: Owens), the Foundation for Child Development Young Scholars Award (PI: Owens), and Brown University’s Population and Training Center, which receives funding from the NICHD (Grant no. P2CHD041020), for invaluable feedback on this manuscript. Direct correspondence to: Jayanti Owens, at jayanti.owens{at}yale.edu, 165 Whitney Ave., New Haven, CT 06511, United States.
Open Access Policy: RSF: The Russell Sage Foundation Journal of the Social Sciences is an open access journal. This article is published under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.
REFERENCES
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.