
Abstract
Data from a unique survey of court-involved New Yorkers collected during the COVID-19 pandemic in 2020 provides evidence for a cycle of disadvantage involving penal control, material hardship, and health risk. We find evidence of chaotic jail conditions from March to May 2020 in the early phase of the pandemic, and high levels of housing and food insecurity, and joblessness for those leaving jail or with current criminal cases. The highest levels of material hardship—measured by housing insecurity, unemployment, shelter stays, and poor self-reported health—were experienced by those with mental illness and substance use problems who had been incarcerated.
The COVID-19 pandemic created significant threats to health and material well-being in low-income communities. The effects of the pandemic were especially severe for those involved in the criminal justice system. Prisons and jails experienced ferocious outbreaks of the virus (Hawks, Woolhandler, and McCormick 2020; Wang et al. 2020). The social and economic instability caused by incarceration and other criminal justice involvement also contributed to exposure to infection, reduced opportunities for safe quarantine, and added to economic insecurity.
This article examines the connections between criminal justice involvement, acute material hardship, and exposure to COVID-19. In our conceptual framework, these conditions are mutually reinforcing, creating serious challenges for implementing mitigation strategies among people who are incarcerated or otherwise involved in the criminal justice system. Criminal justice involvement may impair social and economic security (Wakefield and Uggen 2010; Travis, Western, and Redburn 2014), and socioeconomic insecurity can increase the risks associated with infectious disease (Riley et al. 2007). Disease can harm economic well-being, which can in turn put people at greater risk of involvement with police and penal facilities (Western 2018). Jails in particular—characterized by high population turnover and often located within municipalities—were centers of viral transmission and sources of social instability for those who were released to pandemic conditions (Puglisi et al. 2021).
Although our conceptual framework suggests that health risks and material hardship can escalate for people at risk of incarceration, population heterogeneity and social policy intervention suggest how spirals of sickness and poverty can be alleviated. Drawing on prisoner reentry research, we explore health status as an important dimension of population heterogeneity (Western 2018). Unusual material disadvantage has been found among formerly incarcerated people with dual diagnoses—histories of mental illness and substance use problems. We study the possibility of elevated hardship and health risk for that group. We also examine the use of safety net programs among justice-involved people, particularly for those with serious health problems.
In addition to contributing to a multidimensional perspective on poverty under pandemic conditions, this article also provides an account of reentry from incarceration. A number of data collection efforts provide a relatively clear picture of the ebbs and flows of decarceration efforts and of trends in incarceration and infection over the course of the pandemic, particularly in prisons (Lemasters et al. 2020; Wang et al. 2020). Less is known about the experience of leaving incarceration, returning to communities under pandemic conditions, and facing the cumulative effects of disease, social control, and economic insecurity.
Capturing the social dynamics of pandemic life for people involved in the criminal justice system requires a research design that observes experiences of incarceration and community conditions. This analysis takes advantage of a unique data collection from a sample of people who faced criminal charges, and in some cases incarceration, in New York City during the pandemic. The interviews with people incarcerated and released during the pandemic provide information on conditions inside New York’s Rikers Island jail complex. The interviews are supplemented with reports and grievances collected by the New York City Board of Corrections, which conducted investigative interviews at Rikers throughout 2020. Interviews with people who were released from jail during the pandemic or remained in the community throughout the study period also shed light on community conditions for people with open criminal cases; respondents discussed in great detail the pandemic’s effects on their income, housing, health care, and program participation.
We begin by presenting a conceptual framework that motivates our analysis, which links material hardship, health, and criminal justice involvement. After discussing the early spread of COVID-19 in U.S. prisons and jails and the responses of correctional systems and legislatures to the pandemic, we describe our research design. The empirical analysis examines jail conditions by studying respondents’ qualitative reports of Rikers Island in early 2020, augmented by investigative reports from the New York Board of Corrections. It then looks into conditions of socioeconomic insecurity, comparing the experiences of respondents who we recruited in jail with those we recruited at court (who were not incarcerated following their arraignments), focusing on employment, health, housing and social program participation. A closing thematic analysis of qualitative interview data provides deeper context for the quantitative results.
The results indicate chaotic conditions inside Rikers Island in early 2020 when the COVID-19 pandemic first hit New York. Initially, few systematic protocols were in place, and reports from incarcerated people point to very high risks of COVID-19 exposure. Those released from Rikers and other court-involved individuals also experienced very high rates of joblessness, poor health, and housing instability. Socioeconomic insecurity was significantly greater among jail-recruited respondents than court-recruited respondents, particularly so for those reporting mental illness and a history of substance use. Qualitative interviews provide additional details underlining the extreme social isolation experienced by those with criminal cases at the height of the pandemic. Despite dire conditions in New York City for people with criminal cases, we also find substantial participation in social programs that reduced the level of material hardship.
MATERIAL HARDSHIP, CRIMINAL JUSTICE INVOLVEMENT, AND HEALTH
Sociological research indicates the close connections between penal control, poverty, and risks to health (Wakefield and Uggen 2010; Wakefield and Wildeman 2013; Western 2018). A large research literature studies the connections between criminal justice involvement, including incarceration, and poverty and socioeconomic insecurity. One line of research describes how unemployment, poverty, low education, and housing insecurity expose the economically disadvantaged to elevated risks of police scrutiny and incarceration (see, for example, Bridges and Myers 1994; Sampson and Laub 1994; Wacquant 2009; Duneier 1999). In this account, economic disadvantage is associated with greater involvement in crime, but beyond the link between poverty and crime, criminal justice officials also focus their attention on poor people and communities, resulting in the “criminalization of poverty” (Bell, Garlock, and Nabavi-Noori 2020). Another line of research examines the opposite causal connection, studying the possible impact of criminal justice involvement on economic status, and finds that police contact and incarceration confer stigma and disrupt major life activities thereby undermining economic opportunities (Western 2006; Pager 2007; Mueller-Smith 2015; Dobbie, Goldin, and Yang 2018).
Although criminal justice involvement, in general, has been found to be closely connected to poverty and its correlates, there is evidence that incarceration is particularly harmful. Jeffrey Grogger (1995) analyzes California court data, comparing the effects of arrest, probation, jail incarceration, and imprisonment on employment. He finds that the largest negative effects were associated with incarceration in jail and prison. Closer to the current analysis, a recent study of New York City court records also finds that jail incarceration was associated with reduced employment (Dobbie, Goldin, and Yang 2018). Consistent with research on the negative socioeconomic consequences of incarceration, studies of prisoner reentry also find that incarceration is severely disruptive, breaking connections to family, housing, and employment. Release from incarceration thus creates challenges of rebuilding familial and social bonds, finding a stable job, and acquiring a safe and affordable residence (Western 2018; Harding, Morenoff, and Wyse 2019).
Health problems are also closely linked to economic disadvantage and criminal justice involvement. The connection between health and economic well-being is the starting point for research on the social determinants of health (Marmot and Wilkinson 2005). Infectious disease specifically is found to have a strong economic gradient, related to both access to medical care and the health risks directly connected to the conditions of poverty, including factors such as unhealthy housing and poor nutrition (Riley et al. 2007; Braverman 2011). Health problems associated with criminal justice involvement are also well documented. Research in this area has focused on the health status of incarcerated people, although researchers have also examined the links between mental health and police contact (Sugie and Turney 2017; Massoglia and Pridemore 2015; Geller et al. 2014). Aggressive policing and incarceration are closely associated with poor physical and mental health (Sewell, Jefferson, and Lee 2016; Sewell and Jefferson 2016; Schnittker, Massoglia, and Uggen 2012). Poor health in the incarcerated population is often related to enduring poverty and risky health behaviors such as needle use, heavy alcohol use, and smoking (Fazel and Baillargeon 2011). Researchers have observed rates of chronic conditions such as hypertension, asthma, and arthritis around 50 percent higher in prison than in the community (Binswanger, Krueger, and Steiner 2009; Fazel and Baillargeon 2011). Mental health among incarcerated people is also poor, as evidenced in surveys showing high rates of mood disorders and serious mental illness (Raphael and Stoll 2013).
Although people involved in the criminal justice system are likely to be in poor health even before incarceration, some of the strongest evidence of a causal relationship between incarceration and health relates to infectious disease. Researchers have examined outbreaks of infectious disease in prison, focusing on the spread of tuberculosis, influenza, and varicella (Beaudry et al. 2020). Each of these diseases is airborne and spread through aerosol transmission (droplets) and contact with surfaces. The congregate living areas, dining halls, and recreation areas that make up the physical plant of prisons and jails facilitate the spread of airborne pathogens, particularly in overcrowded conditions. Population turnover raises the risk of both bringing infections in from surrounding communities, and also transmitting disease back to the communities from which the incarcerated population (and correctional staff) is drawn.
The criminal justice system has a complex relationship with the health status of court-involved and incarcerated people. The public’s contact with police and jails significantly increased beginning in the 1980s as drug enforcement and order maintenance policing intensified, and incarceration rates grew precipitously (Gelman, Fagan, and Kiss 2007; Kohler-Hausmann 2018; Western et al. 2021). Such policing efforts may have increased criminal justice contact with people with substance use disorders and other health problems. Certainly, police and jails are among the frontline responders to mental health crises and drug overdoses among poor people, particularly in public space (Irwin 1985; Stuart 2016; Beckett and Herbert 2010; Lara-Millán 2021). Although penal facilities are a significant provider of medical care, about one in five prisons in 2019 was under a consent decree or court order, and court oversight in about half of those cases related to allegations of inferior medical or mental health care.
The triangular relationship between criminal justice involvement, material hardship, and poor health is likely mutually determining. Criminal justice involvement becomes more likely under social conditions of poverty, and the stigma of a criminal record and the harms of incarceration can also undermine economic well-being. Poor physical and mental health are risk factors for contact with police and the courts, and incarceration can impair health, particularly through transmission of infectious disease. Poor health, in turn, imposes limitations on physical and cognitive functioning and on daily activities. Poor health is a deficit of human capital that threatens regular employment and stable housing.
Poverty scholars have often observed that the correlates of economic hardship reflect not causal relationships, but the multidimensional character of socioeconomic disadvantage (Desmond and Western 2018). Sociologists analyzing poverty at the ecological and individual level have observed that “things go together” (Sampson 2012; Simes 2021) creating conditions of “correlated adversity” (Western 2018).
From this perspective, the COVID-19 pandemic created severe conditions of correlated adversity, compounding the relationships between criminal justice involvement, health risk, and material hardship. Although these conditions clustered together, conditions of material hardship and elevated health risk are likely to vary with what has been called “human frailty” (Western 2018). The idea of human frailty emphasizes heterogeneity among people involved in the criminal justice system, in which the worst conditions of material hardship and risks to health were likely experienced by people with histories of incarceration, mental illness, and substance use disorders. Examining variation in outcomes by health status helps illuminate how criminal justice policy operates as a de facto response to untreated health problems among poor people.
Research indicates that incarceration raises the risks of infectious disease and creates the challenge at reentry of finding a job and housing after release from jail. Among those who are incarcerated, severe hardship has been observed among those contending with life histories of substance use and mental illness. These dimensions of ill-health among poor men and women raise the risks of criminal justice involvement and impede social integration after incarceration (Western 2018; Sirois 2019; Harding, Morenoff, and Wyse 2019). In the following analysis, we explore the relationships between criminal justice involvement, material hardship, and poor health, comparing survey respondents we recruited in jail with those we recruited at criminal court (not incarcerated at arraignment). We examine whether people who were incarcerated at Rikers experience worse outcomes, and whether formerly incarcerated respondents with histories of mental illness and substance use are at unusually high risk of joblessness, housing instability, and poor health.
THE EARLY SPREAD OF COVID-19 IN PRISONS AND JAILS
Prisons and jails emerged early in the pandemic as hotspots of COVID-19 infection and transmission, resulting in disproportionately higher incidence and death rates among incarcerated people than among the general population (Wang et al. 2020). By the week of April 22, 2020, the infection rate in the prison population was more than 150 percent greater than among the general U.S. population (Park, Meagher, and Li 2020). By August that year, the cumulative case and COVID-19-related mortality rates were around four and two times higher among people incarcerated in prisons than in the general population (Schnepel 2020). Average rates hide a lot of variation between states. Age-adjusted prison to state mortality rate ratios, for example, ranged from zero in fourteen states to more than ten in four states in August 2020 (Schnepel 2020). Prison staff too experienced much higher COVID-19 case prevalence than the U.S. population overall: their cumulative case rate in fact more closely reflects that of the prison population (Ward et al. 2021; Nowotny, Seide, and Brinkley-Rubinstein 2021).
The pandemic laid bare many of the public health risks posed by the criminal justice system to the people it targets and employs, and their families and communities. Overcrowding and the physical conditions of prisons and jails make it largely impossible for incarcerated people to maintain safe social distance. The court system also brings together large numbers of people in close quarters. Such congregate settings raise the risk of transmission for diseases that can be spread by personal contact (Niveau 2006; Bick 2007; Lofgren et al. 2020). Incarcerated people, their families, and communities are often in poor health and more likely to have diabetes and chronic heart and respiratory diseases that can exacerbate the effects of COVID-19 (Wildeman and Wang 2017; Williams et al. 2020; Howell et al. 2020). The elderly population in prisons and jails has also grown in recent decades, outpacing the rate of aging in the general population (Chan et al. 2021; Williams et al. 2012). Further, older adults in jail have higher rates of geriatric diseases than those in the general population (Greene et al. 2018). Finally, prisons and jails experience a daily churn of staff members, visitors, and new admissions that can interfere with viral containment and other public health efforts in surrounding communities.
Population turnover happens in all penal institutions but is especially prominent in jails, where admission rates are significantly higher than for prisons. Prisons are operated by state and federal governments and typically incarcerate people who are convicted of felonies and receive a sentence of at least a year. Jails, on the other hand, are county or municipal facilities that incarcerate people who are awaiting court action or serving sentences for low-level offenses. In 2019, the jail admission rate was eighteen times higher than the prison admission rate (Zeng and Minton 2021; Carson 2020). By many metrics, jail conditions are also worse than prison conditions. Jails do not typically offer programming and often fail to provide adequate accommodations for sleeping or eating. The jail population faces severe and immediate medical needs, often having been detained for low-level offenses amid mental health crisis or relapse to addiction. Because of the high level of population turnover, the lack of programming, and a population characterized by acute physical and mental health problems, jails are often more chaotic and dangerous than prisons. Because of their conditions and scale of admissions, jails as centers of outbreaks of infectious disease also pose significant transmission risks to surrounding communities.
Decarceration emerged early as an effective strategy to mitigate COVID-19 spread within correctional settings and in the community (Wang et al. 2020; ACLU 2020). Under pandemic conditions, prison and jail populations declined rapidly beginning in March 2020 but began to rebound by the end of the year. On average, jail populations declined more rapidly and substantially than prison populations. Whereas jail reductions resulted from decreases in admissions and releases in excess of admissions, prison decreases appear to have been achieved almost entirely by decreased admissions. New data released by the Bureau of Justice Statistics shows that U.S. prisons released 10 percent fewer people in 2020 than in 2019 (Harvey, Taylor, and Wang 2020; Sawyer 2022).
In the week following the White House’s March 16 call for “30 Days to Slow the Spread” in its “Coronavirus Guidelines for America,” jail populations decreased sharply and continued to decline for eight weeks before rising again in mid-May despite increasing local COVID-19 case rates (Harvey, Taylor, and Wang 2020). A national sample of 415 county jails saw an average decline of 33 percent from March to May of 2020, but by December 2021 that decrease shrunk to 10 percent, and there was a 0 percent average change between July and December of 2021 (Widra 2022). Vera Institute’s data collection of 1,309 jail jurisdictions shows similarly that the majority of the population decrease took place between March 15 and April 15 and that the pace of population decline slowed significantly by June 1, 2020 (Heiss et al. 2020).
Reductions in jail populations in 2020 were due to a combination of decreased admissions and increased releases achieved through court orders, actions by jail administrators and sheriffs, prosecutor discretion, and changes in policing (Prison Policy Initiative 2021). Reflecting the nonsystemic character of the U.S. criminal justice system (Rubin and Phelps 2017; Mayeux 2018), state and local penal authorities’ efforts to reduce jail populations varied in their level of coordination and aggressiveness. Jail population trajectories between March and June of 2020 reflect this variation, falling largely into three categories: rapid decline followed by stability, initial decline followed by a quick increase, or stability throughout (Heiss et al. 2020). Jails in the West saw the largest of the early population decreases; those in the South saw the smallest average decreases (Harvey, Taylor, and Wang 2020).
COVID, RIKERS ISLAND, AND MATERIAL HARDSHIP
New York City and its jails at Rikers Island were at the epicenter of the pandemic. The number of COVID-19 cases and the government response to the pandemic escalated rapidly in March 2020. Following the declaration of a state of emergency on March 7 and the closure of public schools on March 16, New York Governor Andrew Cuomo ordered a statewide “pause” on March 20. Businesses were shuttered, nonessential workers were directed to stay at home, and City residents were instructed to maintain a six-foot distance from others in public.
By the time of our field period in 2019 and 2020, the Rikers Island jail complex had accumulated a long history of institutional violence, staff misconduct, and federal oversight (Bharara et al. 2014; Martin et al. 2019). In the years before the pandemic, popular pressure to close the jail escalated following reports in 2015 that twenty-two-year-old Kalief Browder had committed suicide after being detained on Rikers Island for three years, including seventeen months in solitary confinement, while awaiting trial for allegedly stealing a backpack (Gonnerman 2014, 2015). In 2015, after four years of litigation and a Department of Justice investigation, the City agreed to major reforms, including restrictions on officer use of force and the appointment of a federal monitor. Despite the consent judgment, the monitor continues to document frequent staff violence toward incarcerated people and other facets of pervasive disorder. Homer Venters, chief medical officer of the New York City jail system from August 2015 to March 2017, described Rikers as dominated by a culture of violence in which detainees were regularly beaten by correctional officers, yielding large numbers of head injuries, facial fractures, and lacerations requiring sutures (Venters 2019, chap. 2). Solitary confinement was widely used at Rikers Island. About 7.5 percent of the population were held in punitive segregation on an average day in 2013, and an additional number diagnosed with mental illness in a facility dedicated to “restricted housing units” (Haney et al. 2016). Persistent problems of violence and mismanagement ultimately forced the New York mayor’s office to announce plans in 2017 to close Rikers Island by 2026 (Mayor’s Office of Criminal Justice 2018).
Conditions of violence, disorder, and physical dilapidation at Rikers Island created a fertile environment for infectious disease. When COVID-19 first arrived in New York City in early 2020, Rikers Island quickly became a hotspot. By April 23, a total of 1,027 Department of Corrections staff had tested positive, and 323 people remained incarcerated with confirmed cases. Three incarcerated people had died in jail of complications associated with COVID-19, and news reports counted eight staff deaths (New York City Board of Correction 2020; Paul and Chapman 2020). The infection rate among people incarcerated at Rikers was more than forty times the national rate and almost six times the rate in New York. By May, more than a dozen COVID-19 fatalities of staff and incarcerated people had been recorded (Ransom 2020). The risks of infection and death at Rikers were borne disproportionately by Black and Latino men, who face very high risks to jail incarceration in New York City (Western et al. 2021).
Seeking to avoid a public health disaster, correctional administrators, policymakers, and advocates devised strategies for diversion from incarceration and early release for those who were medically vulnerable (UCLA School of Law 2020). In New York, the jail population declined by 30 percent, from 5,458 on March 16 to 3,888 by April 23, 2020, the lowest it had been since the 1940s (Mayor’s Office of Criminal Justice 2020). New York’s bail reform law, passed in April 2019 and implemented on January 1, 2020, resulted in a nearly 25 percent reduction shortly before the pandemic. The most dramatic decrease, though, since at least 2014 occurred during the week of March 23 to March 29, when 630 people were released (Miller, Martin, and Topaz 2022).
The rapid decline in the jail population resulted partly from deliberate efforts to accelerate release and partly from a reduction in admissions due to a slowdown in the operation of New York City criminal courts. Specifically, three measures drove the early and precipitous drop in New York City. First, the Early Release Program designed by the Mayor’s Office of Criminal Justice led to the discharge of 296 people with less than a year remaining on their sentences, requiring them to do daily remote check-ins with case managers. Second, a March 27 decision in a Legal Aid Society lawsuit resulted in the release of 106 people held on parole violations. Third, Governor Cuomo ordered the Department of Corrections and Community Supervision to review further cases of people detained on technical violations. Subsequent Legal Aid Society lawsuits and case-by-case reviews, as well as public defenders’ efforts to argue bail writs, contributed to further population decline, which continued until the end of April (Rempel 2020).
Despite likely saving people from hospitalization and death, jail population reductions did not persist after April 29, 2020. Due to rollbacks to bail reform and a tapering off of emergency responses, the population began to increase gradually in May 2020, eventually surpassing its pre-pandemic level in February 2021 (New York City Board of Correction 2021; Chan et al. 2021). The number of confirmed COVID-19 cases in New York City’s incarcerated population also began to climb following a slow but steady decline between April and November 2020.
The onset of the pandemic in 2020 suggests three distinct lines of empirical study to explain the conditions of life and health risks faced by court-involved New Yorkers. First, we examine conditions inside the Rikers Island jail complex as the COVID-19 outbreak rapidly escalated in the first half of 2020. Second, we examine quantitatively several dimensions of material hardship, including joblessness, housing instability, poor health, and benefit receipt. In the quantitative analysis, we focus on the experience of people who were incarcerated at Rikers Island, including that subset with histories of mental illness and substance use problems. Finally, qualitative analysis helps describe how New Yorkers facing criminal charges experienced the lockdown period of the pandemic.
DATA
We report on new data collections from three main sources. First, we analyze data from the Rikers Island Longitudinal Study (RILS), a panel interview study of 286 New Yorkers facing a new criminal charge. We recruited half the respondents from arraignment courts in Brooklyn, Manhattan, and the Bronx between July and November 2019 and half from three jails on Rikers Island between November 2019 and January 2020.
Prospective respondents were eligible for the study if they were charged with a violent felony or reported at least three prior arrests in the previous five years. We focused on these two groups because people charged with violent felonies or with multiple prior arrests form two key groups whose incarceration rates must be reduced as part of the plan to close the Rikers Island jail complex.
We used real time charge data from the New York State Office of Court Administration to identify eligible potential respondents in arraignment courts. When a potential respondent received nonfinancial release (rather than remand or bail hold), a member of the research team approached them outside court and attempted to recruit them into the study. Those who agreed to participate typically completed the baseline survey immediately, in a courthouse public seating area.
We identified and recruited eligible respondents at Rikers Island with the assistance of the New York City Department of Corrections (DOC), which sent us a list of eligible potential respondents at the start of each of our recruitment weeks. Members of the research team went in pairs to each of the three jails where potential respondents were held and provided DOC officers the lists of potential respondents. DOC officers brought research team members to one of the jail’s communal spaces, typically the chapel or visiting room, to wait while the officers located the potential respondents and attempted to recruit them into the study on our behalf. Those who agreed to participate were brought to the communal area, where they completed the baseline survey. Officers respected respondents’ privacy and waited outside of the communal areas until the interviews were complete. Incarcerated respondents received $30 for the baseline survey, which, depending on their stated preference, we deposited into their commissary accounts, sent to a designated friend or family member, or gave them on their release from jail.
The study followed each respondent for about one year after their initial court appearance or immediate post-arraignment incarceration, interviewing them at three months, six months, and twelve months following the initial baseline survey. Each follow-up survey contained the same set of core questions focused on respondents’ housing, income, family arrangements, criminal legal system contact, and health and health care. Each survey wave also included a topical module that asked questions about lifetime criminal justice system contact, health and health care, and childhood experiences. An oversample of respondents age eighteen to twenty-five years old also received extended qualitative interviews.
On March 15, 2020, Columbia University (where RILS is based) announced that in-person research was to be “ramped down.” The RILS shifted from conducting interviews in person to doing them by telephone. We designed a COVID-19 survey to obtain data on health status and living conditions during the lockdown. From this point on, all interviews with community-based respondents were conducted by telephone. Incarcerated respondents could not be interviewed because we could not guarantee the confidentiality of calls to the jail. Respondents who were incarcerated at the time of their scheduled twelve-month interview received a paper survey. Respondents received $30 for the baseline survey and $50 for each subsequent survey. The subsample of qualitative interview respondents received an additional $20 per survey. The RILS completed data collection in March 2021 with an overall retention rate of about 70 percent.
The second source of data reported below came from administrative records on social service use. Around 75 percent of RILS respondents consented to the use of their Social Security numbers to obtain administrative records from the New York City Department of Social Services, which included monthly Supplemental Nutritional Assistance Program (SNAP) benefit amount and monthly nights-in-shelters administered by the New York City Department of Homeless Services (DHS). Of the 216 matched respondents, 103 spent at least one night in shelter between July 2014 and December 2020, and 189 received SNAP benefits in at least one month during that period. New York does not consider drug felony convictions when determining SNAP eligibility (Sheely 2021).
Finally, to obtain information on jail conditions during the pandemic, we rely on data collected by New York City’s Board of Corrections (BOC), which regulates jail conditions and correctional health care in New York City jails. In May 2020, it began conducting targeted on-site inspections of jail facilities to supplement its remote monitoring of the Department of Corrections’ COVID-19 response. During each of their on-site visits since the start of the pandemic, BOC staff has interviewed two to four incarcerated people about their physical, emotional, and psychological well-being, jail sanitation and hygiene, access to health care, personal protective equipment, and mandated services. The BOC shared with the research team audio recordings of thirty-six interviews they conducted with forty-five incarcerated people, some of whom participated in pairs, and detailed notes of four interviews they conducted with four incarcerated people who did not want to be audio recorded. We also obtained complaints to the BOC about jail conditions from incarcerated people, family, and friends.
COVID-19 ON RIKERS ISLAND
Interviews with RILS respondents after their release from jail and BOC respondents while they were incarcerated shed light on conditions inside New York City jails during the pandemic. In the early phase of the COVID-19 crisis on Rikers, cases were mounting rapidly and BOC and DOC hurriedly established new protocols to try and quarantine people who were medically diagnosed or had tested positive. Standard procedures for quarantining, cohorting, testing, and reducing the density of the population had begun to emerge by the summer. However, in the first half of 2020, jail staff and health-care workers were still learning how to control the spread of infection.
Medical complaints registered with the Board of Corrections reflected the chaotic conditions inside the jail at the onset of the outbreak. The BOC notes describe one phone call received from the jail: “Caller stated that he’s vomiting, coughing and defecating excessively. He feels he may have the virus. Caller said he’s been asking for medical treatment to no avail. Feels that since he’s been moved to a jail with a smaller population he should finally be able to get medical assistance.” A friend or family member of another incarcerated man called the BOC to express concern about the dehumanizing conditions at Rikers:
He along with other inmates are suffering poor unhealthy conditions in that facility. They are being denied proper care, getting minimum standards, inmates have not been let outside to get air in over three weeks, no library services, no religious services. . . . They are also bringing inmates who have tested positive for COVID. The inmates are not being paid for two weeks for the working services they are doing. Place is filthy unsanitary, they have rats coming out nowhere. These are humans we’re talking about; they are all being treated like animals.
Crowded conditions and poor sanitation were described in another call by an incarcerated person to the BOC: “Inmate stated there are 40 inmates in the housing area and it’s physically impossible to social distance. He also claims they have no hand sanitizer or masks. Inmate stated he’s spoken to the Captain and [Deputy Warden] of the jail to no avail. He does not know who else to talk to.”
Our own interviews also described unsanitary conditions, confusion, and anxiety during the outbreak. A week after her release, a twenty-two-year-old woman described quarantine in jail as “horrible. [We were] left in the same uniform, no toothbrush, no hot water. Medical team was horrible. Thirty other girls in the same cell.” The quarantine was supposed to last fourteen days, but since she had asthma, she was released after six days when she tested positive for COVID-19. She went to live with her mother after she left the jail.
An eighteen-year-old male respondent described the challenges of controlling the spread of the virus at the jail: “I was showing some similar symptoms to the coronavirus, and I was sent to EMTC [a jail on Rikers Island] as a precaution. The problem with that was that I was not tested at RNDC [his previous jail on Rikers Island]. I was tested at EMTC where I was exposed to the coronavirus because they had been sending people there who tested positive or who were awaiting and tested negative. . . . The pens weren’t being sanitized. There were no gloves, there were no masks.” Another eighteen-year-old respondent tested positive for COVID-19 while incarcerated at Rikers Island. A few months after being released in late March of 2020, he said “the way corrections handled the pandemic was . . . absolutely disgusting, inhumane, and it showed that there was no real care and no real preparation.” He described how unsanitary conditions, inadequate medical care, quarantine procedures, and isolation took a “heavy mental toll.”
They wouldn’t sanitize or disinfect the rooms. . . . It was very tough to stay healthy, to stay clean. When I was there, I did a three-day quarantine . . . and I was only allowed out of the cell for one hour a day. And on top of that, I hadn’t showered for those four days because somebody who had tested positive actually vomited blood in the shower and the correctional officers there refused to get a team inside the unit and start cleaning it up. And on top of that, they didn’t have the solution to give us ourselves so we could clean it. . . . So, it was very tough to keep your mind positive and stay healthy in such conditions.
As in other outbreaks of infectious disease, DOC staff struggled to provide a high standard of care for a population already in poor health, elevating their risk of exposure.
HEALTH AND HARDSHIP OUT OF JAIL
Incarcerated people faced high risks of COVID-19 infection and death in the first few months of the pandemic, but release from incarceration and the social conditions of poverty presented their own health risks. Our survey data provide information about the conditions of life in the community for those going through the criminal courts. We divide our sample into two groups. The first includes respondents who were recruited to the study in court and never incarcerated during the study period. To examine the elevated risks of material hardship among the incarcerated and those in poor health, we define a second subsample of respondents who were incarcerated at baseline and recruited at Rikers Island who also reported a history of mental illness and substance use disorders. We refer to this subset of respondents as the AIM subsample, named for the characteristics of addiction, incarceration, and mental illness.
Table 1 reports descriptive statistics from the RILS sample, dividing the sample into those who were never incarcerated during the study period, the incarcerated subsample recruited at Rikers Island, and the AIM subsample, which includes people recruited at Rikers who reported mental illness and addiction at the baseline interview. The sample is mostly male with a median age of thirty-two. Four in five respondents were Black or Hispanic. As is common in samples of justice-involved respondents, we found high rates of self-reported mental illness and substance use problems. More than half reported they had prior diagnoses of mental illness and 42 percent reported that “drugs or alcohol had been a problem for them.” Court-recruited respondents were demographically similar to those recruited at jail, but tended to have slightly lower self-reported rates of mental illness and drug use.
Percentage Distribution in Sample of Court-Involved New Yorkers, Rikers Island Longitudinal Study
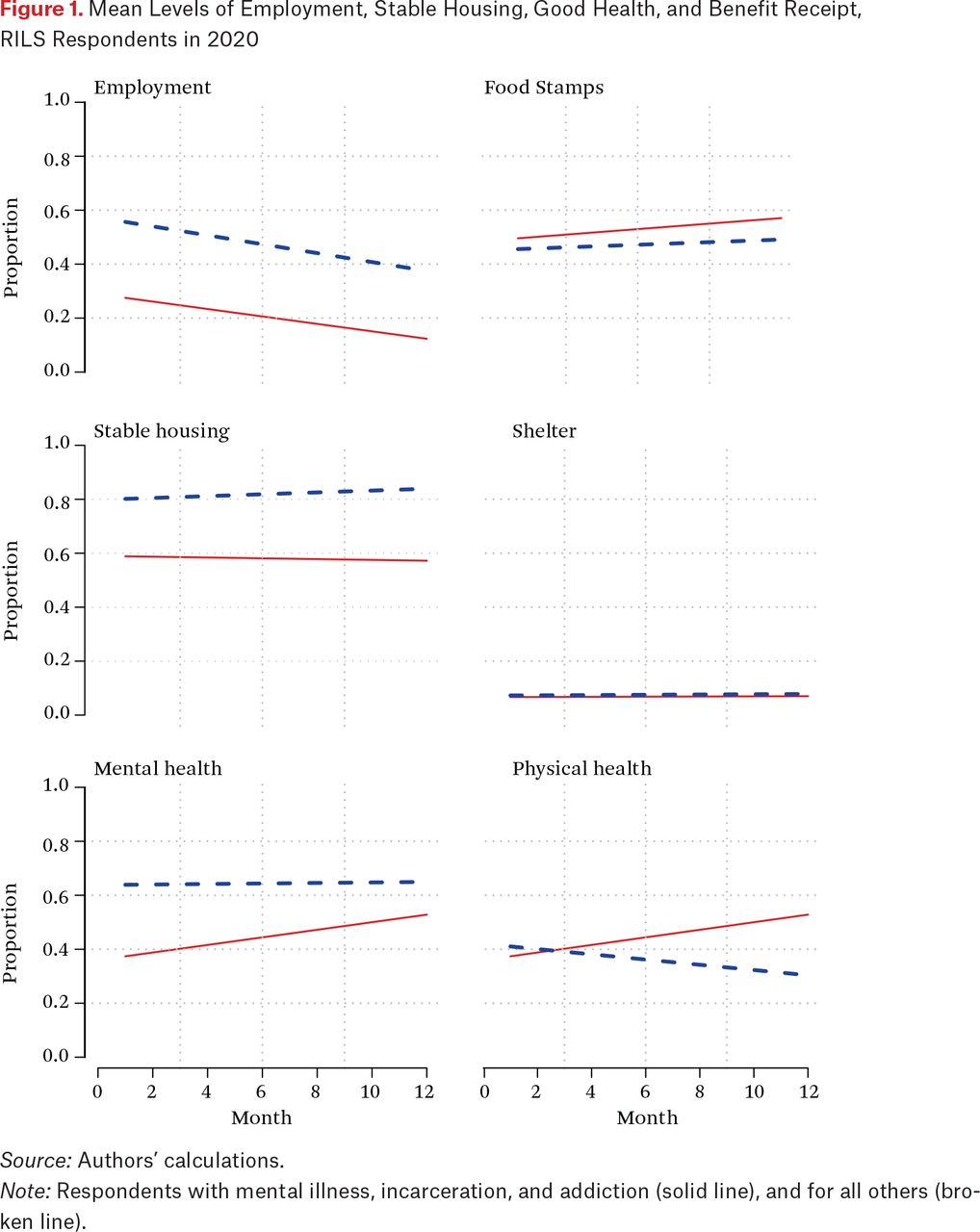
Respondents were interviewed several times in overlapping interview waves. We can get a picture of life conditions over the pandemic year of 2020 by organizing the data chronologically. Figure 1 shows the proportion of respondents reporting their employment, housing, and health status each month. All the data in these figures reflect results from community-based telephone interviews, so respondents who were incarcerated at baseline and interviewed at follow-up were reporting on their status following release from incarceration. In figure 1, we separate the AIM subsample from all others. Both groups’ employment rates declined over the year. By December 2020, less than 20 percent of the AIM subsample and 40 percent of the rest were reporting any employment income. About half the sample, with little difference by AIM status, were enrolled in food stamps each month. The AIM subsample reported a very high level of housing instability defined as living at several different addresses, in a shelter or other group quarters, or on the streets. We were unable to detect this self-reported housing instability in administrative records on DHS shelter use, however. The entire sample reported monthly shelter use at similar rates. Finally, the AIM subsample reported relatively poor mental but not physical health.
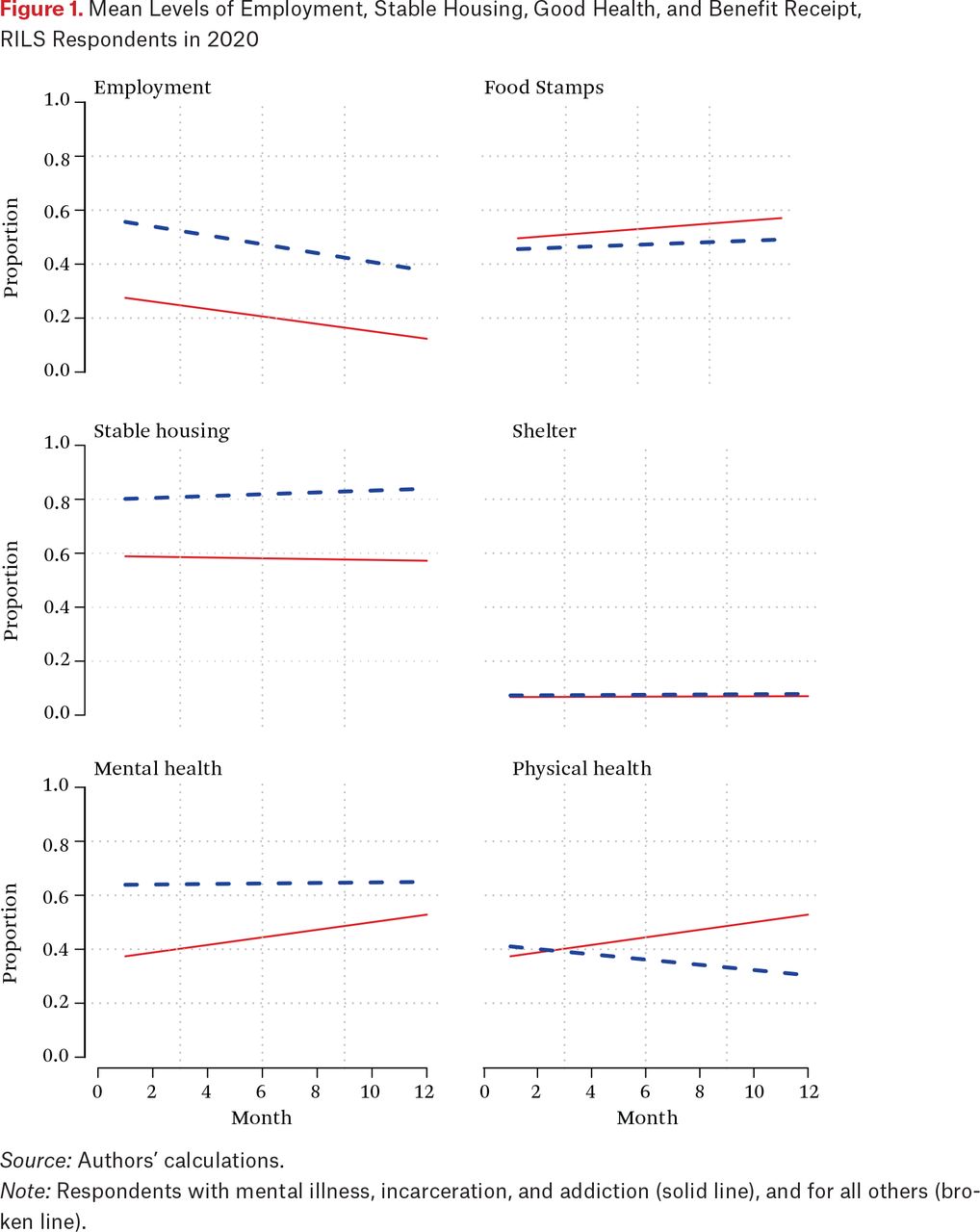
Mean Levels of Employment, Stable Housing, Good Health, and Benefit Receipt, RILS Respondents in 2020
Source: Authors’ calculations.
Note: Respondents with mental illness, incarceration, and addiction (solid line), and for all others (broken line).
We further explore descriptive differences within the sample with regressions that include indicators for respondents who were in jail at baseline, who were in jail and reported histories of addiction and mental illness, and who were recruited in court. The regression analysis pools together four waves of survey data for dichotomous measures of employment, stable housing, and self-rated mental and physical health, adding controls for age, race, and gender. In regressions of SNAP benefit receipt and DHS shelter stays, we analyze monthly administrative records.
To study outcomes in the period of pandemic restrictions, we add a dummy indicating observations in the time period after March 20, during pandemic restrictions, and add interactions with incarceration and AIM status. In these models, the regression intercepts are the pre-pandemic means of the dependent variables for the reference groups: non-AIM or nonjail respondents, white, male, and in their twenties.
The interaction effect describes the well-being of the jail and AIM respondents relative to those who were recruited at court. In the results for employment, the regression results indicate that nearly 60 percent of court-recruited respondents were employed over four survey waves in 2020 (table 2). Employment was nearly 15 percentage points lower for the incarcerated respondents, and 23 percent lower for those who were incarcerated at baseline and had histories of mental illness and addition. The pandemic main effect indicates that employment dropped significantly, by about 10 to 15 points, in the pandemic period for the fraction of the sample who were court-involved but not incarcerated. The point estimate of the interaction effect shows the incarcerated respondents experienced a relatively large employment decline, but not the AIM group, whose jobless rate was very high to begin with.
Regression Results for Measures of Well-Being, 2020, Rikers Island Longitudinal Study
We observe similar patterns for housing and health. Incarcerated and AIM respondents were less likely to report living in stable housing, and housing stability did decline for those two groups, although the drop during the pandemic period was not statistically significant. The deficit in self-rated physical health is clear for the AIM respondents, but not for those who were incarcerated at baseline. Health status generally declined during the pandemic period, but the decline in health status was concentrated among those whose health was relatively good at baseline: court-recruited respondents and incarcerated respondents without histories of addiction or mental illness.
The final two columns of the table show results from administrative records for SNAP benefit receipt or a stay in a DHS shelter. About three-quarters of the reference group were enrolled in SNAP in any given month before the pandemic. The most vulnerable who were incarcerated at baseline or incarcerated with histories of addiction or mental illness, enrolled at rates 8 to 10 points higher than the rest of the sample. Benefit receipt increased during the pandemic but the increase was not significantly larger among the incarcerated or AIM respondents. DHS shelter stays, although less prevalent, followed a similar pattern. Jail and AIM respondents used the DHS shelter system more than court-recruited respondents, although shelter usage did not significantly increase for any group during the pandemic.
In sum, the quantitative results generally indicate lower levels of employment, stable housing, and health status after release from jail incarceration, and material hardship was greatest among formerly incarcerated respondents with histories of mental illness and substance use. Hardship was greater for the sample as a whole during the pandemic, although, contrary to our expectations, the increase in hardship was not significantly larger for the formerly incarcerated. SNAP was widely used by the entire sample, and especially by the incarcerated and AIM subsample. The use of safety net programs also increased significantly in the pandemic period for the sample as a whole.
QUALITATIVE RESULTS
How pandemic conditions were subjectively experienced by the sample respondents can be gleaned from qualitative interview data. Three themes that help illuminate the dimensions of material hardship emerged. Respondents spoke about housing insecurity, emotional hardship, including health-related stress, and economic effects. These themes were coded inductively by a team of three qualitative interviewers. All names are pseudonyms. Direct quotes are taken from contemporaneous field notes and audio recordings and have been edited for verbal tics and clarity.
Homelessness and Housing Insecurity
In any given month, about one in three of all respondents were unstably housed: residing in the shelter system, between several addresses, or on the street. Homelessness created significant challenges to meeting a variety of basic needs. Brian, a forty-five-year-old homeless man whose mental illness had resulted in conflicts with neighbors and arrests, previously warmed up at restaurants or used bathrooms that were mostly closed at the time he was interviewed. “There’s one place that is used to me coming in that still lets me use the bathroom, so that’s the one bathroom I have,” Brian said. “The park bathrooms are closed. . . . To get out of the cold—it was almost freezing—I’ve been having to go into vestibules of buildings from 1 a.m. to 6 a.m. before people wake up. But now they’ve been locking outer doors so it’s been harder to find buildings I can actually access.”
Michelle, a homeless forty-year-old woman who suffered from anxiety, reported that “Everything is closed. . . . Places I go to eat are closed. Places I sit down at . . . You can’t get money. You can’t use the bathroom. You can’t sit and rest anywhere because you’re scared people could cough on you. You can’t trust people.” But, she said, she was not giving up: “I feel my life is worth fighting for.”
Those without stable housing interrupted housing searches and moved between shelters and family members’ homes. Sasha, a twenty-two-year-old homeless respondent, had been sleeping on the floor of a friend’s apartment. After COVID-19, she moved into a shelter. “I don’t have the luxury of quarantining,” she said. These accounts of respondents with unstable housing highlight the hardships accompanying a public health strategy that assumes the availability of secure households that can support isolation.
Emotional Hardship and Health Stress
Some 38 percent of respondents reported emotional hardship (feelings of anxiety, depression, or irritability), and another 34 percent reported health-related stress. Respondents postponed or canceled doctor’s appointments, surgeries, and children’s vaccinations. Some lost access to counseling and mental health services. For others, new restrictions on visits to facilities such as nursing homes interrupted care for loved ones.
Daniel, a forty-seven-year-old formerly incarcerated man, rode the subway to help his mother with groceries, but worried about exposing himself and his pregnant partner to COVID-19. “My mom lives in another borough, and going on the train is dangerous. . . . I need to see my mom to help her, but I don’t want to go because of my kid and my family. . . . I have twins on the way, due in July.” Because medical and other caring work typically involves personal contact, isolation disrupts the networks of care for people who live alone.
Economic Effects
Respondents widely described the recession conditions that accompanied the shutdown. Forty-four percent of respondents reported reductions in income, or disruptions to employment or job searching. Twenty-four-year-old Tyler said, “I was supposed to have a job at a carrier company in Manhattan. They told me to come back after corona is over.” “There’s a Family Dollar by here that’s still hiring,” he continued. But when he went to submit an application, the long line outside was “like a club.” By April, job searching had largely ended among unemployed respondents. Essential service workers, often conducting deliveries or working in health care (as janitorial staff in hospitals, for example), were among a small group with employment continuity.
Associated with the economic effects of the shutdown, 10 percent of respondents had difficulty obtaining food or had been to a food pantry in the week before the interviews that took place in June and July of 2020. Khalid, a twenty-nine-year-old man who lived in public housing with his girlfriend, their newborn, and two older stepchildren, expressed anxiety to us about feeding his family. In the week before the interview, Khalid and his girlfriend traveled from New York to visit a Rhode Island hospital where they heard they could get free food. The hospital, however, turned them away, having suspended their food service in response to COVID-19.
The experiences of Tyler and Khalid illustrate the material vulnerability of those involved in the criminal justice system. Although housing security provides some protection against pandemic conditions, economic hardship was widespread and survival strategies drew respondents into public space.
DISCUSSION
Poverty scholars have argued for a multidimensional concept of material hardship, where a variety of life adversities cluster together (Sampson 2012; Desmond and Western 2018; Western 2018). The COVID-19 pandemic created intense conditions of correlated adversity in which incarceration, acute health risks, and economic disadvantage clustered together amid subjective feelings of isolation and severe stress.
Evidence from inside Rikers Island jail and from community-based surveys of court-involved New Yorkers point to three main empirical findings. First, Rikers Island clearly elevated the risk of coronavirus infection, particularly from March through May of 2020, when jail conditions were chaotic. In this period, the jail struggled to provide basic sanitation, protective clothing, and effective quarantine to stem the spread of infection. Second, community conditions for all court-involved New Yorkers were characterized by a high level of material hardship. Around 75 percent of the sample reported food stamp enrollment in any given month during the yearlong study period. About 25 percent of the entire RILS sample reported living in shelter or unstable housing and about 20 percent of the DSS matched sample spent at least one night in a DHS shelter during the study period. Third, one group in the sample who had been incarcerated at baseline, and reported histories of mental illness and addiction, experienced extreme material hardship related to housing security, unemployment, and poor self-reported health.
The pandemic, criminal justice system involvement, and poverty appeared to operate in a self-reinforcing cycle. COVID-19 spread throughout the jail early in the spring of 2020. People were often released in these early months without stable housing or income and had little way of safely isolating. Unemployment increased significantly during the pandemic months, and health status declined. Notably, and contrary to our expectations, the most vulnerable respondents—who had been incarcerated at Rikers Island—did not suffer unusually large losses of employment, stable housing, or health relative to the sample as a whole.
To what extent are the observed health risks related specifically to incarceration and other criminal justice involvement, and to what extent are the risks related to the life conditions of poverty? The rapid spread of infectious disease in prisons and jails has been well documented, and penal facilities were COVID-19 hotspots across the country. Strong evidence indicates that incarceration increased the risk of infection, and this seems especially likely at Rikers Island for staff and incarcerated people alike. Although incarceration is correlated with poverty, incarceration at Rikers Island in the spring of 2020 added to the risk of infection with the novel coronavirus.
Beyond the dynamics of disease transmission, incarceration is closely associated with an array of insecurities and disadvantages that make up the social conditions of poverty. For those who faced criminal charges or who had a record of incarceration, it is more difficult to say that criminal justice exposure caused additional health risks on top of all the correlates of poverty that criminal justice involvement commonly entails. Isolating the effect of criminal justice on health risk, however, probably raises the wrong policy question. The close correlation among a variety of risky conditions points to the importance of a multipronged approach that addresses the main sources of disadvantage for court-involved people—unstable housing, low income, and poor health care. If criminal justice policy under pandemic conditions has a task, it would be to mitigate negative effects of the criminal justice process on housing, income, and health care, and minimize exposure to disease in the criminal justice process.
Like other articles in this issue (Bell et al. 2023; Bitler, Hoynes, and Schanzenbach 2023), this analysis indicates that the cycle of disadvantage was clearly attenuated by social policy intervention. SNAP enrollment was generally high in the sample, and DSS data show the proportion of respondents receiving SNAP in any given month increased in the pandemic period. SNAP provided a near-cash, in-kind benefit of around $200 a month for most of those in the sample. Qualitative interviews indicated food insecurity and hunger over the course of the year, and food stamps offered some relief. Some jurisdictions deny SNAP eligibility to people with felony drug convictions, despite their evident value in reducing extreme hardship during the pandemic. Consistent with the disruptions to housing as a result of incarceration, the shelter system was used at a significantly higher rate by respondents who had been incarcerated.
These results point to an alternative policy regime that might address the conditions of correlated adversity observed among the survey respondents. In this alternative regime, jail populations are small, jail stays are brief, sanitation and health care in jail are high quality, and income support in the community can buffer the effects of reentry on material hardship. Stable housing emerged as an acute need for court-involved New Yorkers in the pandemic year, and housing problems were associated with health risks, material hardship, and criminal justice involvement. The City’s shelter system provided emergency housing that was regularly made available to those leaving incarceration. Research suggests the importance of continuous residence in private households for social integration after incarceration (Sirois 2019; Western 2018). An encompassing regime of social support should also address the problem of unstable housing that was common among those who navigated the pandemic after incarceration while contending with poor physical and mental health.
- © 2023 Russell Sage Foundation. Plummer, Samantha, Timothy Ittner, Angie Monreal, Jasmin Sandelson, and Bruce Western. 2023. “Life During COVID for Court-Involved People.” RSF: The Russell Sage Foundation Journal of the Social Sciences 9(3): 232–51. DOI: 10.7758/RSF.2023.9.3.10. This research was supported by grants from the William T. Grant Foundation, the Robert Wood Johnson Foundation, the Russell Sage Foundation, the J.C. Flowers Foundation, and the Tiger Foundation. We thank the New York City Departments of Social Services and of Corrections for providing data used in this research and our study participants for sharing their stories with us. Direct correspondence to: Bruce Western at bruce.western{at}columbia.edu, Department of Sociology at Columbia University, United States.
Open Access Policy: RSF: The Russell Sage Foundation Journal of the Social Sciences is an open access journal. This article is published under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.
REFERENCES
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.