
Abstract
The Affordable Care Act was a landmark political achievement in reforming the American health insurance system but has been subject to considerable political pressure. Administrative actions, such as eliminating federal advertising, have served as a replacement for failed legislative repeal efforts. We use a county-level fixed-effects model with data for thirty-four states for the 2015 to 2018 open enrollment periods to measure dose-response relationships between health insurance and health-care-related political advertising and Marketplace enrollment. State-sponsored advertising is related to greater Marketplace enrollment, but we find no association between federal advertising and enrollment. We are, however, unable to account for the endogeneity of advertising decisions across media markets and potential federal coordination with other sponsor types. These results have implications for understanding public roles within privatized policy implementation.
The Patient Protection and Affordable Care Act of 2010 (ACA) was a landmark political achievement in reforming the American health insurance system, expanding coverage to the millions of uninsured through three primary channels. The dependent coverage provision, which took effect in 2010, allowed young adults to remain covered by their parents as a dependent up to age twenty-six. An expansion of Medicaid to everyone living below 138 percent of the federal poverty level was meant to cover low-income individuals uniformly in all states. A Supreme Court ruling in 2012, however, made this optional, leaving a coverage gap in those states that chose not to expand.1 The Marketplace, as the collection of federal and state-run health insurance exchanges is commonly known, began operation in late 2013 to provide guaranteed-issue private health insurance coverage to nearly everyone not eligible for employer-sponsored coverage (exceptions based on immigration status), offering premium subsidies available to those between 100 and 400 percent of the federal poverty level. These expansions led to about twenty million more people insured by the end of 2016 (Garrett and Gangopadhyaya 2016; Obama 2016). However, the polarized politics of the ACA—which has met uniform Republican opposition since before its passage—has continued to threaten these policy achievements.
President Donald J. Trump campaigned vigorously on repealing and replacing the ACA, but was unable to do so despite having a Republican-controlled Congress for the first two years of his term. Republicans have been fairly silent on repeal and replace since their failures in 2017 and 2018, but have pursued administrative retrenchment that might undermine the program in important ways. For example, the Trump administration eliminated federal television advertising for HealthCare.gov for the 2018 open enrollment period, reduced grants to community organizations for enrollment assistance, and shortened the open enrollment period (ninety to forty-five days) a year earlier than scheduled (Jost 2017; Johnson 2017; Kliff 2017; U.S. Department of Health and Human Services 2017)—actions that many view as designed to hobble the ACA and participation in the Marketplace (Patashnik and Oberlander 2018). This is to say nothing of the encouragement of state Medicaid waivers that have tested the limits of the program’s mission, resulting in litigation and holds on implementation of waivers in several states. Marketplace enrollment fell by only 4 percent during the 2018 open enrollment period (Kaiser Family Foundation 2019), falling short of the dire expectations of many in the face of these actions. Some argued that this demonstrated federal investments in outreach to be ineffective and unnecessary. Others countered that the enormous volume of free media, from near-constant news coverage of the repeal and replace efforts over the course of several months in addition to increased premium subsidies, due to the elimination of the cost-sharing reductions, helped buffer enrollment losses.
The public receives information about the ACA from a variety of sources. During the launch of the first open enrollment period for these new state and federal health insurance exchanges, survey data suggested that the top source of information for new enrollees on the Marketplace was television news (PerryUndem Research/Communication and Enroll America 2014). In October 2016, just before Election Day, respondents to the Kaiser Family Foundation Health Tracking Poll reported getting most of their information about the health-care law from newspapers, radio, or online news (45 percent), cable television (32 percent), national broadcast television (28 percent), and local television news (27 percent) (Kaiser Family Foundation 2016). Advertisements aired on national cable channels and local broadcast networks are also an important source of information and still a channel for reaching most Americans (Bialik and Matsa 2017; Pew Research Center 2018). Television advertising for health insurance includes not only federal and state advertising for the Marketplace but also advertising sponsored by insurance companies and nonprofit organizations for products that may or may not be available on the Marketplace, such as off-exchange plans, employer-sponsored coverage, Medicare supplement, and Medicare Advantage (Barry et al. 2018; Gollust et al. 2014; Gollust, Baum, et al. 2018). Political ads taking positions on the ACA—predominantly anti-ACA attacks in the earlier years—were also directly competing for air time with health insurance advertising during the fall open enrollment cycles that coincided with election years: 2014, 2016, and 2018 (Gollust, Baum, et al. 2018; Fowler, Baum, Barry, et al. 2017; Fowler and Ridout 2014; Fowler, Franz, and Ridout 2018). The information environment surrounding the ACA is thus quite complex, with a wide range of positive and negative messages coming from multiple sponsors who have different motivations to educate or persuade consumers (Gollust, Fowler, and Niederdeppe 2019).
PUBLIC AND PRIVATE ROLES IN ACA IMPLEMENTATION: THE CASE OF MARKETING
The ACA presents a paradigm of public policy that engages significant private elements in policy implementation (Hacker 2004; Mettler 2011). Specifically, the plans available on the Marketplace are offered by private insurance companies, albeit with federal subsidies, without a public option—that is, a public health insurance option to compete alongside plans offered by private carriers, which was first considered in the 2009 congressional debate but did not advance to the final bill (Morgan and Campbell 2011a). The move to limit the federal role in marketing in 2017 and beyond, then, is consistent with broader conservative efforts to advance privatization goals since enactment, such as for the Medicare program (Morgan and Campbell 2011b; Patashnik and Oberlander 2018). Whether the federal government should promote private insurance options that are available as a direct result of federal regulation is a critical normative and philosophical question that we engage with later. This privatized policy context also raises the more pragmatic question of whether public advertising is more effective than private advertising at insuring Americans.
During the first (2014) open enrollment period, greater advertising for health insurance was associated with declines in the county-level uninsured rate among those younger than sixty-five, with every thousand ads shown corresponding to an approximate 0.1 percentage point decline (Karaca-Mandic et al. 2017). Disaggregating the advertisement types, Pinar Karaca-Mandic and colleagues (2017) show that state-sponsored ads had the strongest relationships with declines in the uninsured rate. Similarly, greater federal health insurance advertising was associated with higher self-reported shopping (odds ratio [OR]: 1.045, p < .05) and enrollment (OR: 1.067, p < .05) among non-elderly adults during the first open enrollment period (Gollust, Wilcock, et al. 2018). Because these studies covered only the first open enrollment period, it is not clear whether and how the findings might have been maintained in later enrollment cycles, when neither the information about insurance availability nor the opportunity to enroll were novel. Covered California, the state-based marketplace for California, has claimed a 3 to 1 return on investment on advertising and outreach under fairly conservative assumptions (Lee et al. 2017). The state-sponsored television campaign for the now defunct Kynect, the former state-based marketplace in Kentucky, was found to have accounted for approximately 40 percent of online applications, with private advertising functioning as a negative contributor to enrollment by potentially driving enrollees off-exchange (Shafer et al. 2018). The federal government developed internal models for predicting enrollment based on advertising through various channels (television, radio, digital) and reminder strategies, but these estimates are not publicly available (Cohn and Young 2018). Finally, new research also suggests the importance of direct individual outreach on enrollment. Letters sent by the Internal Revenue Service to those who went without health insurance in the previous year (when a financial penalty for doing so was still in place) led to increased subsequent enrollment (Goldin, Lurie, and McCubbin 2019).
Research directly on advertising and Marketplace enrollment is still limited, but we can draw on the much larger literature on the effects of direct-to-consumer (DTC) advertising for pharmaceuticals for several relevant conclusions about the potential effects of private-sector marketing on health-related behavior (Lyles 2002; Mintzes 2012). Results from a variety of research designs—including from randomized controlled trials, observational studies, and quasi-experimental studies leveraging variation across media market borders—all suggest that DTC advertising has effects on consumers’ demand for prescription drugs (Donohue, Cevasco, and Rosenthal 2007; Kravitz et al. 2005; Shapiro 2018; Spence et al. 2005). Importantly, pharmaceutical advertising may not only influence interest in the specific advertised drug, a brand name they may or may not recall, but for other drugs in the same class or for related conditions (Shapiro 2018; Sinkinson and Starc 2019). For example, Bradley Shapiro (2018) finds that television airings of ads for a particular drug for depression (Paxil) increases demand for all drugs in the depression category (Prozac, Wellbutrin, and Zoloft, for example), not just the branded product. Similarly, among the standardized patients in another study (Kravitz et al. 2005) who requested a particular advertised drug from their physician (also Paxil), 27 percent received that drug and 26 percent received an alternative antidepressant in response. Thus a theoretical rationale exists to anticipate that marketing for one type of “product” (such as an ad for Medicaid or an off-exchange plan) could still increase demand for health insurance in the Marketplace.
RESEARCH OBJECTIVE
In this study, we measure the relationship between different types of public and private television advertising and Marketplace enrollment, building on the limited evidence base thus far that relies on single states or a single open enrollment period. We observe changes in health insurance advertising by varied sponsors and enrollment over time at the county level, identifying which types of advertising are associated with enrollment. We also assess the extent to which health-care-related political advertising plays a role, given that perceptions can be shaped by politicians responding to local preferences (Fowler, Baum, Jesch, et al. 2019; Fording and Patton 2020; Pacheco, Haselswerdt, and Michener 2020), distinguishing between likely pro-ACA (pro-Democrat) and anti-ACA (pro-Republican) messages. Our study relies on a panel of counties and applies county fixed effects, exploiting variation in advertising and health insurance market environment within counties over time to assess the association of advertising with Marketplace enrollment. The within-county variation we use to explore changes in enrollment comes from changes in total dose and composition of advertising, insurer participation, plan availability, pricing, and population. Election cycles add an element of variation both within counties over time and across counties due to the offices at stake, competitiveness of race, and increased cost of advertising due to demand for airtime. Although we acknowledge endogeneity between advertising decisions and local characteristics, county fixed effects allow us to hold constant other time-invariant characteristics of counties that might also be correlated with enrollment, as they are with Marketplace vulnerability (Abraham 2020).
METHODS
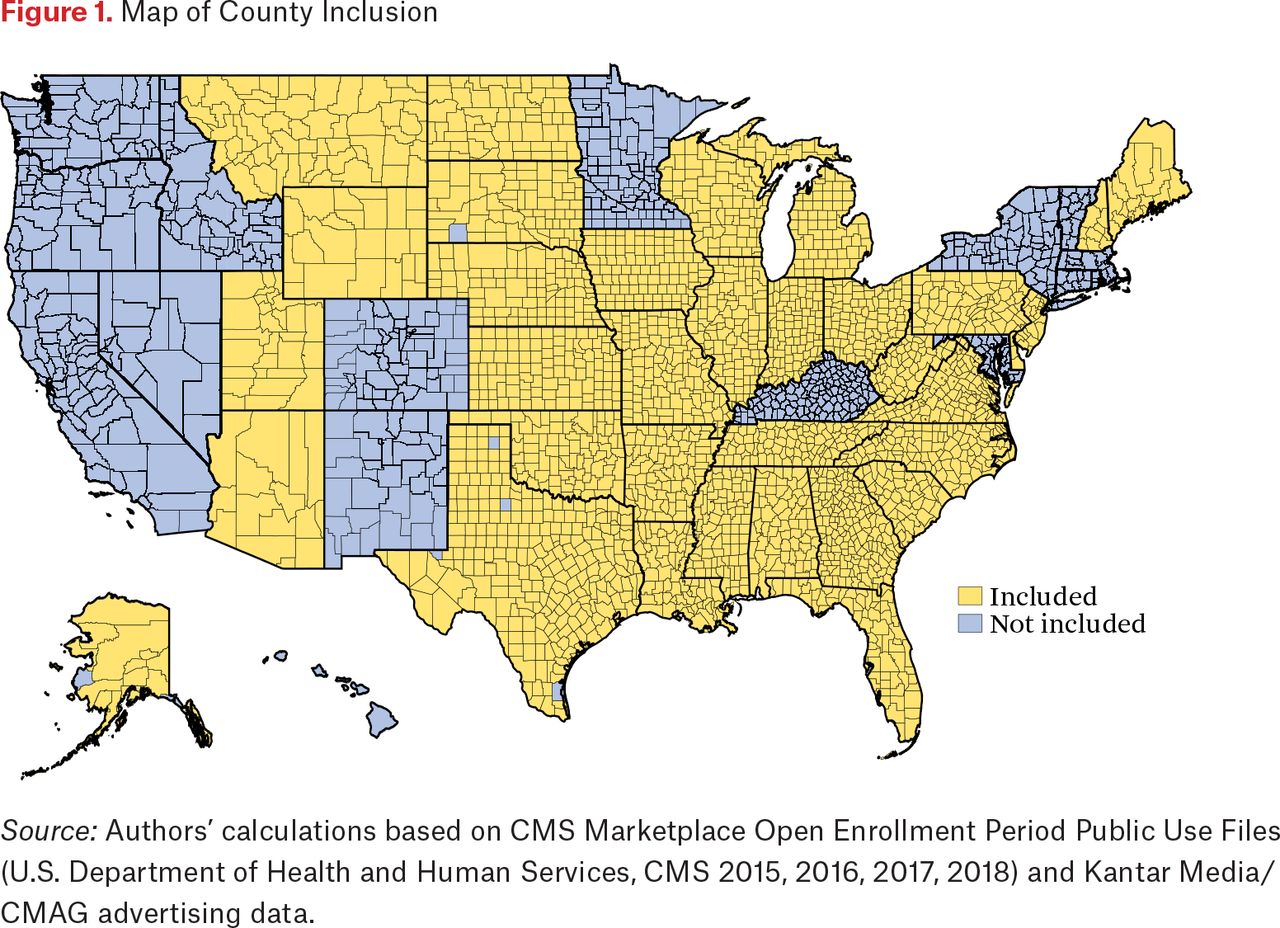
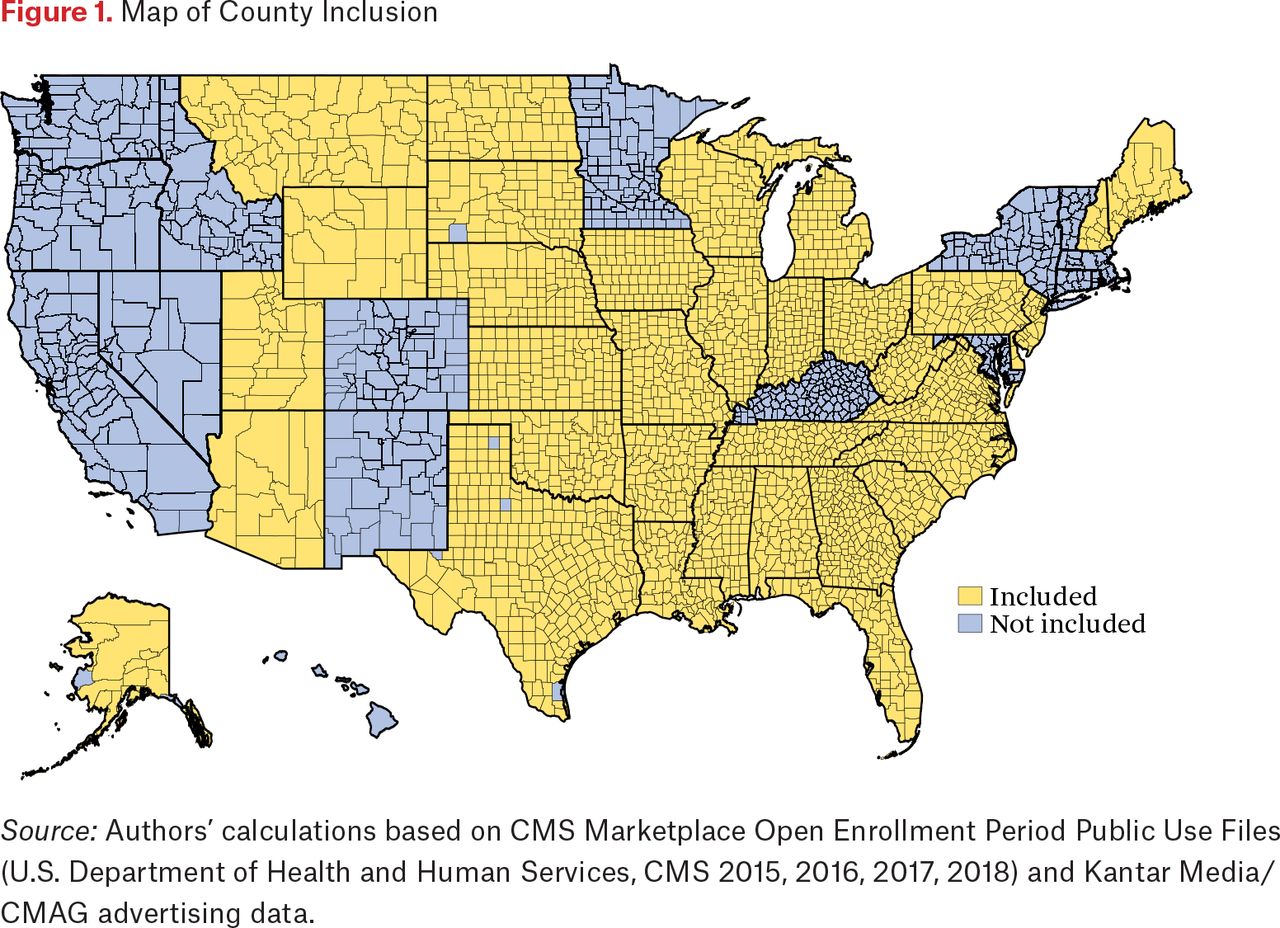
Our study relies on two key data sources, the Marketplace Open Enrollment Period Public Use Files from the Centers for Medicare and Medicaid Services (CMS) and advertising data from Kantar Media/Campaign Media Analysis Group (CMAG) available to us through the Wesleyan Media Project (WMP). We created a county-level panel by merging enrollment data for the 2015 through 2018 open enrollment periods from the Marketplace Open Enrollment Period Public Use Files, capturing on-exchange plan selections in each county over time. These capture plan selections that took place from November 15, 2014, to February 15, 2015 (plus “any in-line or other Special Enrollment Period activity” through February 22, 2015) for the 2015 open enrollment period, November 1, 2015, to January 31, 2016 (plus “any in-line or other Special Enrollment Period activity” through February 1, 2016) for the 2016 open enrollment period, November 1, 2016, to January 31, 2017, for the 2017 open enrollment period, and November 1, 2017, to December 15, 2017 (plus “cleanup for late Exchange activity” from December 16 to December 23, 2017) for the 2018 open enrollment period. We did not include 2014 because the public use data from the Office of the Assistant Secretary for Planning and Evaluation was only available at the zip code level instead of county. Our panel includes all states that used HealthCare.gov for enrollment exclusively during these four open enrollment periods, including federally facilitated marketplace, state-based marketplace–federal platform (SBM-FP), and state partnership marketplace states (see figure 1). States that operated state-based marketplaces (SBM) for enrollment throughout the study period are excluded from the study. Any county-open enrollment period with ten enrollees or fewer was suppressed in accordance with CMS policy to protect consumer privacy.
Similarly, we created a county-level panel data set of health insurance and health-care-related political advertising over the same time period to merge with our Marketplace enrollment panel. This advertising panel was derived from airing level data from Kantar Media/CMAG that captures the media market, date, time, and sponsor for each advertisement on local broadcast networks and national advertisments on cable channels. For health insurance advertising, each ad airing during open enrollment was categorized based on its sponsor name into one of four sponsor types: federal government, state government, private (for example, insurance companies, insurance brokers), and other (for example, nonprofits). This categorization scheme is consistent with earlier work (Karaca-Mandic et al. 2017; Gollust, Wilcock, et al. 2018; Shafer et al. 2018). We excluded ads by other sponsors, mainly advocacy or other nongovernmental organizations from the analyses as they were very low volume, 0.9 percent of total health insurance and health-care-related political ads during this period.
To capture a more nuanced categorization of advertising consistent with our interest in potential spillover from product types, each ad creative was viewed by multiple coders and assigned to one of three health insurance products: private non-Medicare, non-Medicaid (Marketplace, non-ACA compliant plans, employer-sponsored coverage); Medicare (Medicare Supplement, Medicare Part D, Medicare Advantage; may mention Medicaid coincidental with a Medicare focus); and Medicaid (state Medicaid programs, Medicaid managed-care plans, Children’s Health Insurance Program [CHIP]). We excluded ads that could not be assigned to one of the three products, only a small portion of the ads in our sample (0.5 percent). Inter-reliability was reasonably high, with a kappa of 0.85 for Medicare coding and over 0.7 for ads that mentioned or focused on Medicaid.
The airing level data were collapsed to the sponsor type–media market–open enrollment period level with the product totals also captured. For federal and state sponsors, we refer to the private non-Medicare, non-Medicaid ads as Marketplace ads; however, for the private sponsors, we maintain the more descriptive label because the private ads may cover products that are not offered on-exchange or are not ACA compliant (such as short-term plans). Further, we differentiated state-sponsored advertising by whether it was from its own or another state relative to each county (given that ads aired from another state may appear in media markets that cross state lines), as ads referring to consumers’ own state may be more salient to consumers.
For health-care-related political advertising, we totaled ads during these years that mention health care (based on whether Kantar or WMP coders identified it as such) and either support or oppose a specific candidate for president, U.S. Senate, U.S. House of Representatives, or governor. This includes ads sponsored by candidates, political parties, outside groups (such as political action committees), and ads coordinated between candidates and political parties. We only included ads identifiable as pro-Democrat or pro-Republican, excluding those for other affiliations (such as Green, independent). The date range of ads captured as relevant to each open enrollment period varied by year. We included ads from the day after Labor Day (the traditional start of the general election period) through Election Day in federal election years (2014 and 2016, for the 2015 and 2017 open enrollment periods) and from the day after Labor Day through the end of open enrollment in off-cycle years (2015 and 2017, for the 2016 and 2018 open enrollment periods) as advertising for primaries would have extended beyond Election Day. The airing level data were collapsed to the party–media market–open enrollment period level similar to the health insurance ads. We did not differentiate between own and other state health-care-related political ads as we did for state-sponsored health insurance advertising because we are not modeling the political dynamics of each state. This will help account for other health-care-related information that consumers are encountering in addition to health insurance advertising.
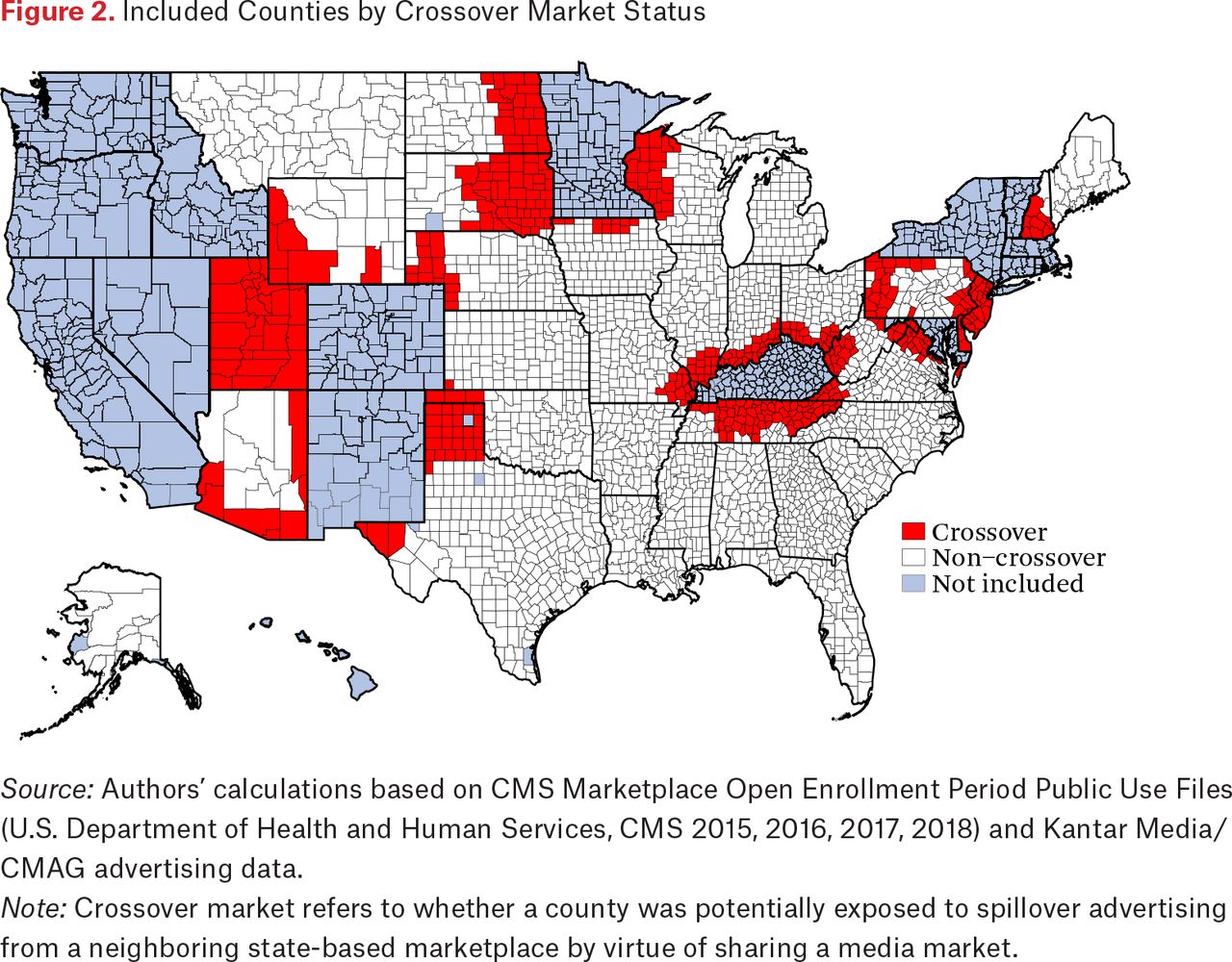
We merged our county-level Marketplace enrollment data with the health insurance and health-care-related political advertising panel using a crosswalk of counties and media markets that assigns each county to a single media market. We also differentiate by whether a county was potentially exposed to spillover advertising from a neighboring state-based marketplace by virtue of sharing a media market with an SBM, referring to these as counties within a crossover market (see figure 2). The political environments and associated messaging about the ACA are substantively different in state-based marketplaces than in those that are not. As discussed elsewhere in this issue, perceptions of the ACA are closely tied with the political configuration of the state government (Pacheco, Haselswerdt, and Michener 2020). Although our analysis does not directly address the underlying political dynamics within these local geographies, advertising spillovers and public perceptions within media markets that overlap with state-based marketplaces may highlight differences in consumer responsiveness to advertising for the federal Marketplace. We used this crossover market construct to stratify our analysis based on where federal advertising would have been the more dominant mode of government-sponsored advertising aired (counties not in a crossover market) versus a heavier weight on own and other state sponsors (counties within a crossover market) (see table A1).
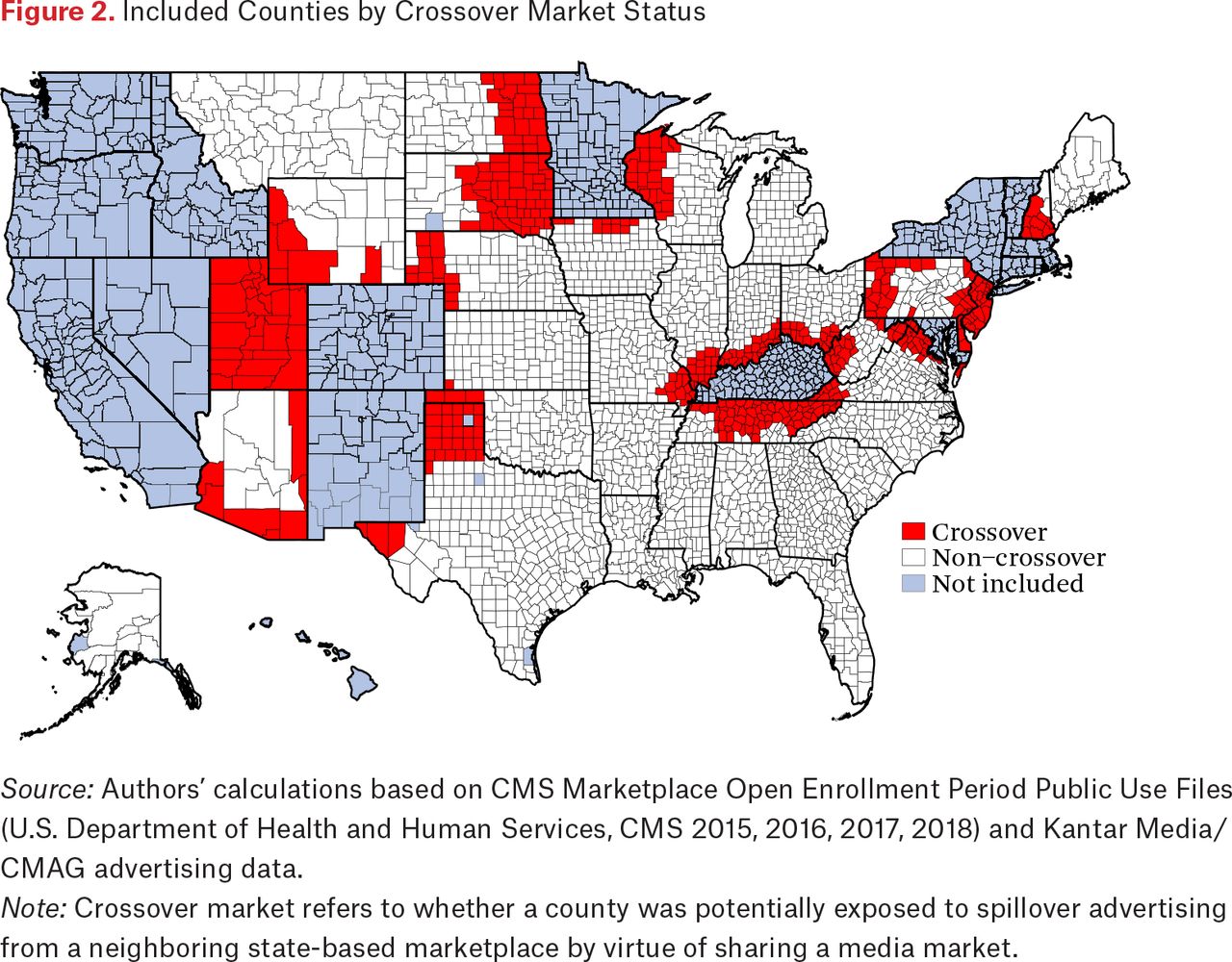
Included Counties by Crossover Market Status
Source: Authors’ calculations based on CMS Marketplace Open Enrollment Period Public Use Files (U.S. Department of Health and Human Services, CMS 2015, 2016, 2017, 2018) and Kantar Media/CMAG advertising data.
Note: Crossover market refers to whether a county was potentially exposed to spillover advertising from a neighboring state-based marketplace by virtue of sharing a media market.
Finally, we incorporated data from the HealthCare.gov Qualified Health Plan Landscape files to describe Marketplace plan availability and pricing. These variables include county-level benchmark premium (for a single, nonsmoking forty-year-old), silver spread (difference in annual premium between second cheapest and cheapest silver plan), number of plans (unique number of plans, catastrophic excluded), and number of carriers (unique number of corporate parents) by open enrollment period. We obtained county-year population under age 65 from the Census Population Estimates Program and county socioeconomic characteristics from the Health Resources and Services Administration Area Health Resources Files.
Statistical Analysis
Our study design exploits the panel nature of the data, using variation in advertising and health insurance market environment within each county over time to understand their association with Marketplace enrollment. Our analytic sample (see figure 1) includes 2,504 counties in thirty-four states over the 2015 to 2018 open enrollment periods, totaling 10,016 observations. We use a county-level fixed-effects model to estimate the association between the volume of health insurance and health-care-related political advertising on Marketplace enrollment per hundred thousand people younger than sixty-five during the 2015 through 2018 open enrollment periods. County fixed effects account for the time-invariant characteristics of counties that may be associated with differences in enrollment, such as health-care provider supply, state scope of practice laws, underlying population health, rurality, and other characteristics that change very slowly or not at all over a short period. Another article in this issue highlights that characteristics of counties are key to insurer participation and market stability (Abraham 2020), leading some areas to be more vulnerable to disruption in their Marketplace that could also shift perceptions about the ACA.
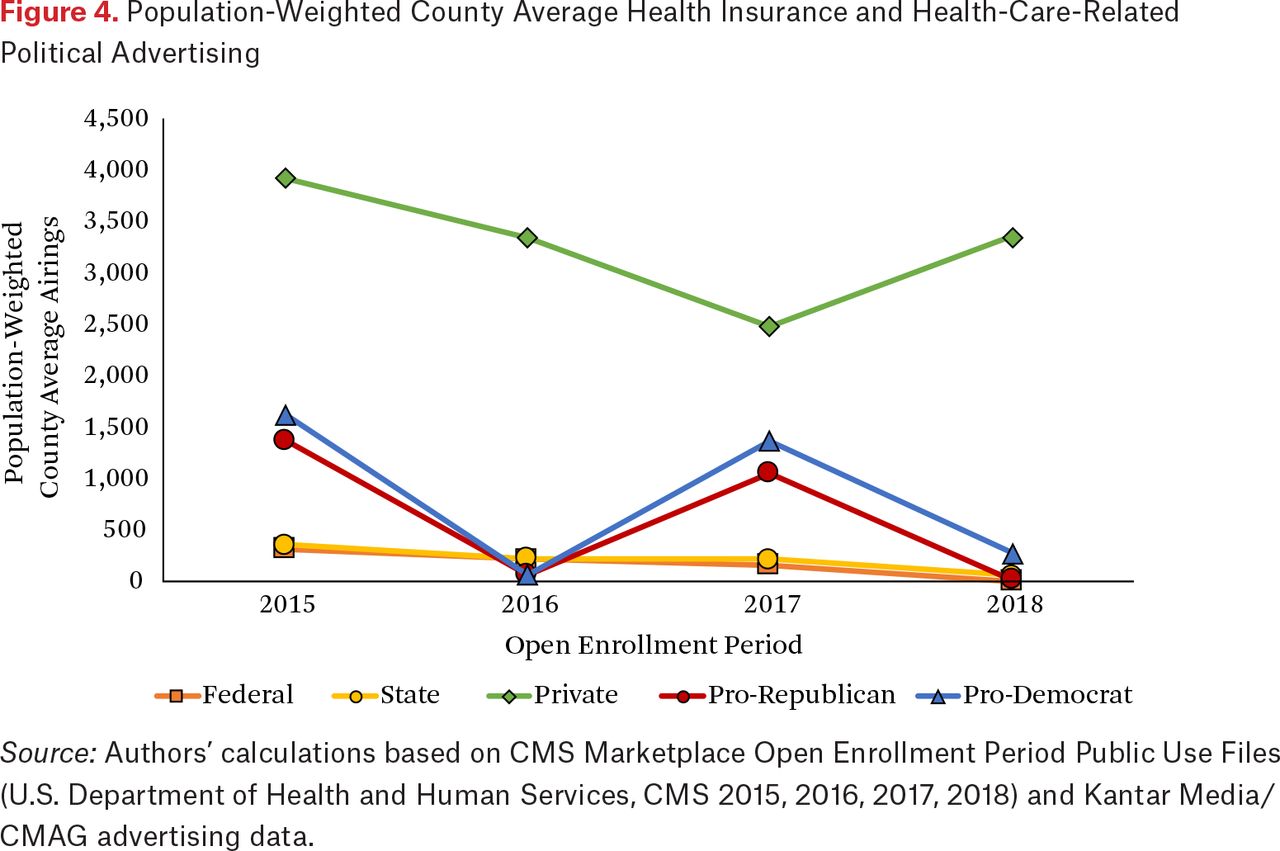
Our models include measures of several types of advertising. We rescaled the measures to provide an interpretation in units of one hundred ad airings rather than one, to provide a more practical interpretation of the change in dose of advertising in each county during open enrollment. We include total ad airings by federal, own state, and other state sponsors by county-open enrollment period (see figure 4 and table A1). Given the lower (and declining) volumes of federal and state ads, we chose to include these at the sponsor level rather than further distinguishing them by product (such as Medicaid versus Medicare). In contrast, the volume of private ad airings was consistently large enough over time to split into separate volumes for Medicaid ads, Medicare ads, and the remainder (non-Medicaid or Medicare). We include pro-Democrat and pro-Republican health-care-related political ad airings by county-open enrollment period. Finally, we also include benchmark premium, silver spread, number of plans, and number of carriers at the county-open enrollment period level to account for variation in Marketplace plan availability and pricing over time. Indicators for each open enrollment period were interacted with each advertising variable to allow for differing associations across years.
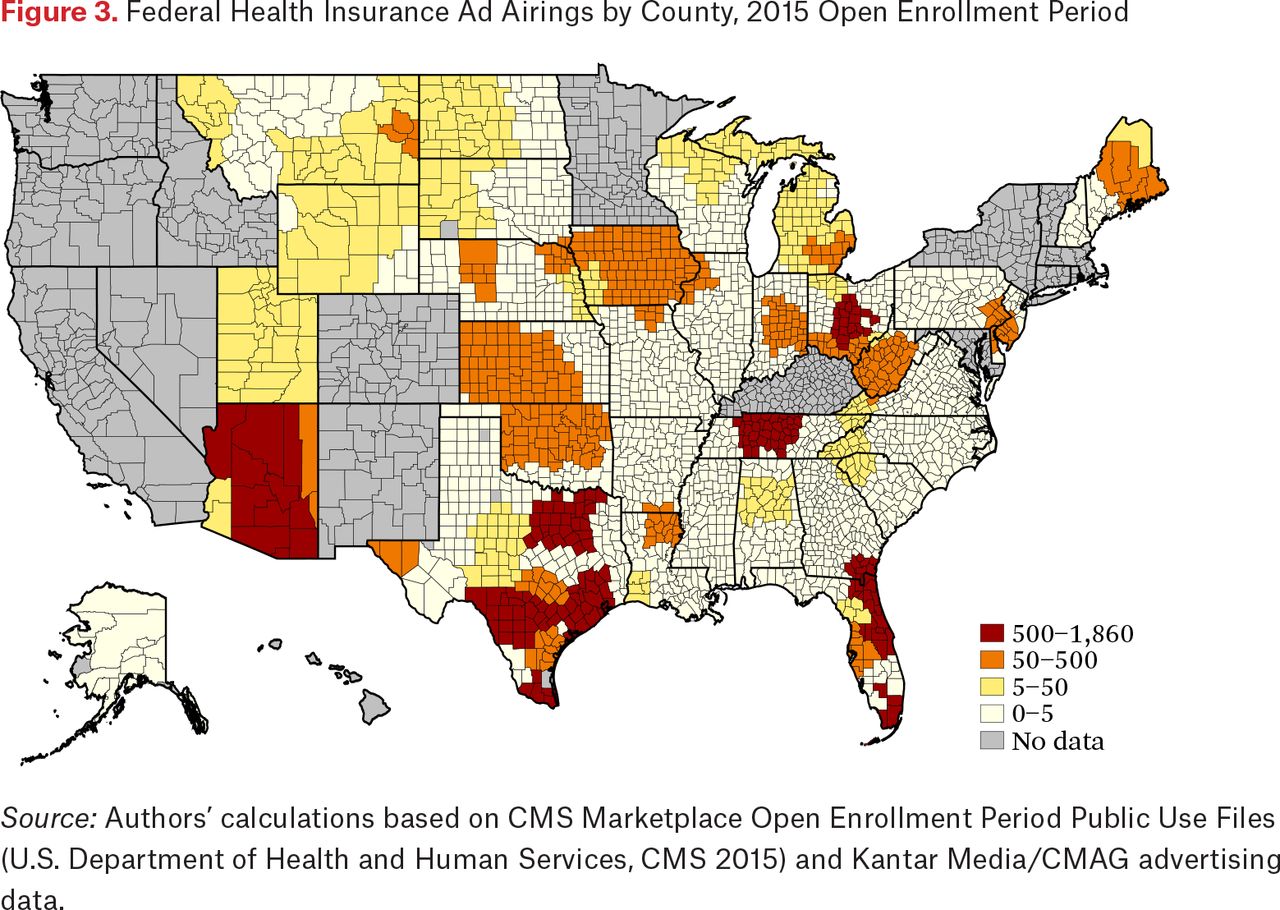
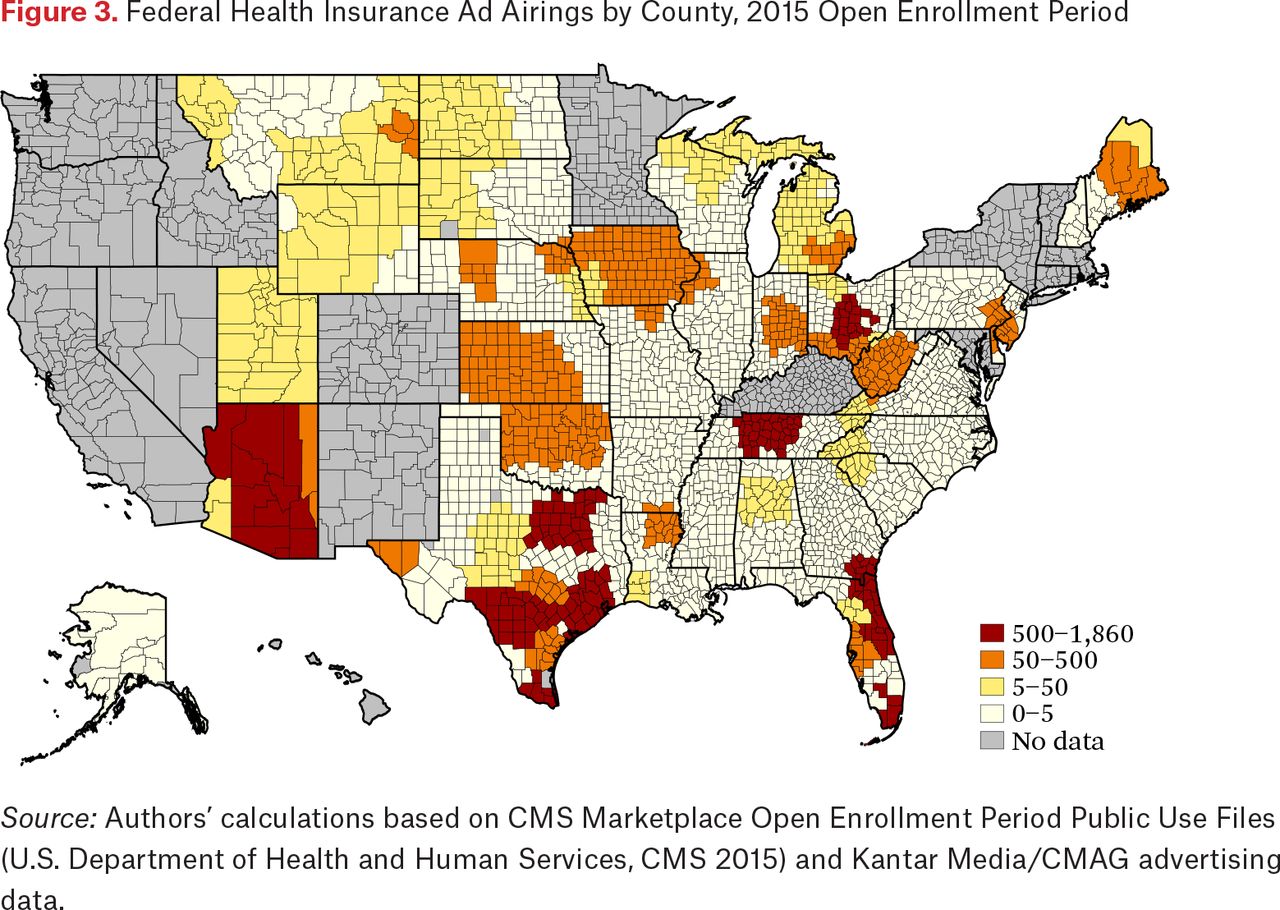
Federal Health Insurance Ad Airings by County, 2015 Open Enrollment Period
Source: Authors’ calculations based on CMS Marketplace Open Enrollment Period Public Use Files (U.S. Department of Health and Human Services, CMS 2015) and Kantar Media/CMAG advertising data.
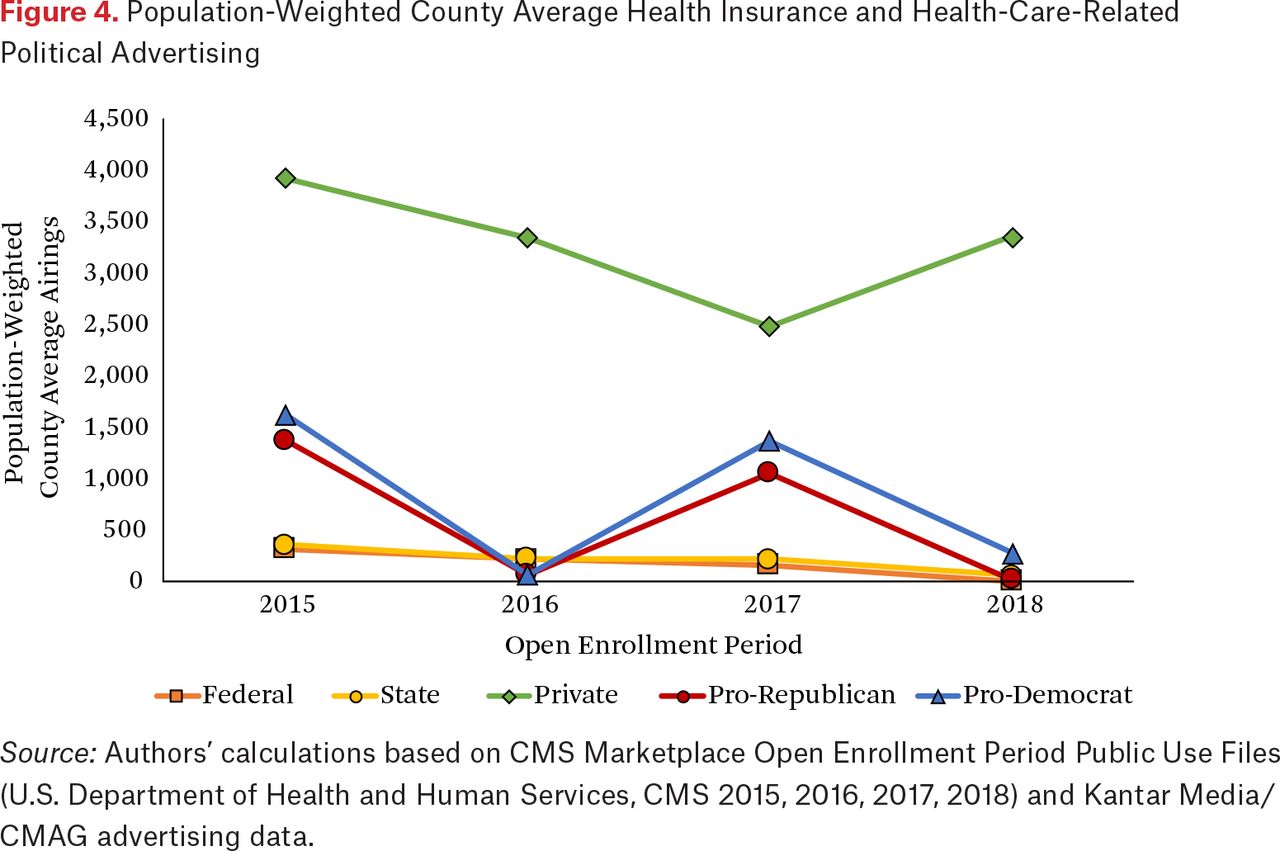
Population-Weighted County Average Health Insurance and Health-Care-Related Political Advertising
Source: Authors’ calculations based on CMS Marketplace Open Enrollment Period Public Use Files (U.S. Department of Health and Human Services, CMS 2015, 2016, 2017, 2018) and Kantar Media/CMAG advertising data.
We weighted our models by county population younger than sixty-five in 2017 (for the 2018 open enrollment period) to allow for more populous areas to be represented proportionally in our estimates as is often done in analyses of policy effects over many counties and/or states (Gertner, Rotter, and Shafer 2019; Shafer 2019, 2017). Standard errors were clustered at the state level to allow for correlation of errors across counties in the same state. We estimated average marginal effects and marginal effects by open enrollment period to describe the association between an additional one hundred airings for each type of advertising with Marketplace enrollment, independent of other factors. We also stratified our models by crossover market status (see figure 2) to explore differential effects by potential exposure to advertising from neighboring states that were state-based marketplaces at any point during the study period. Our analyses were conducted in Stata 14.2 and the maps (see figures 1, 2, A1, and A2) were generated using maptile, a user-written package for Stata (StataCorp 2015; Stepner 2017).
RESULTS
Our set of included counties in thirty-four states captures a near totality of those using the HealthCare.gov enrollment platform for the 2015 to 2018 open enrollment periods; only a handful of counties were lost on the basis of suppressed enrollment data (ten enrollees or fewer) (see figure 1). The volume of health insurance and health-care-related political advertising varies widely by geography and type over time. For example, geographic variability in the number of ads the federal government chose to air indicates that the federal contribution to marketing was by no means uniform. Figure 3 shows the geographic variation in the volume of federal advertising during the 2015 open enrollment period, the first captured in our data, ranging from essentially none to nearly 1,900 ad airings over the three months. In figure 4, we see that population-weighted average health insurance advertising by county was overwhelmingly dominated by private sponsors, increasing from 85 percent of all health insurance ads during the 2015 open enrollment period to nearly 98 percent of all ads in an average county by the 2018 open enrollment period as ads by all other sponsor types declined. In particular, private advertising increased substantially between the 2017 and 2018 open enrollment periods, from 2,480 (range: 0–11,163) to 3,354 (range: 1–11,451) population-weighted average ads per county (range of 2017 to 2018 change: –3,317–4,783), reversing a declining trend in absolute terms and rising as a share of all health insurance advertising. Federal and state advertising volumes were similar by open enrollment period with state being consistently higher, particularly during the 2018 open enrollment period when federal Marketplace advertising had been eliminated (an average of 1 ad airing per county for federal [range: 0–32], 54 for state (own and other combined) [range: 0–1,386]) (see figure 4 and table A1). There were no federal Marketplace ads during the 2018 open enrollment period; however, total federal advertising does not go completely to zero because of ads for Medicare and CHIP (Gollust, Baum, et al. 2018).
The decline in government-sponsored advertising is consistent with evidence on public exposure to ads. The Kaiser Family Foundation Health Tracking Poll reported that the proportion of the public who had heard or seen ads “that provided information about how to get health insurance under the health care law” fell from 41 percent in November 2014 to 32 percent in November 2017 and 28 percent by November 2018 (Kaiser Family Foundation 2014, 2017, 2018). This decline in reported exposure, despite the high volumes of private advertising (as noted in figure 4), may indicate that consumers did not perceive the increased presence of private advertising as a share of all health insurance ads as providing ACA-specific information as much as government-sponsored ads do. Indeed, references to the ACA in all insurance ads aired declined between 2013 and 2016 (Barry et al. 2018) and in insurance-company sponsored ads in particular (Gollust, Baum, et al. 2018).
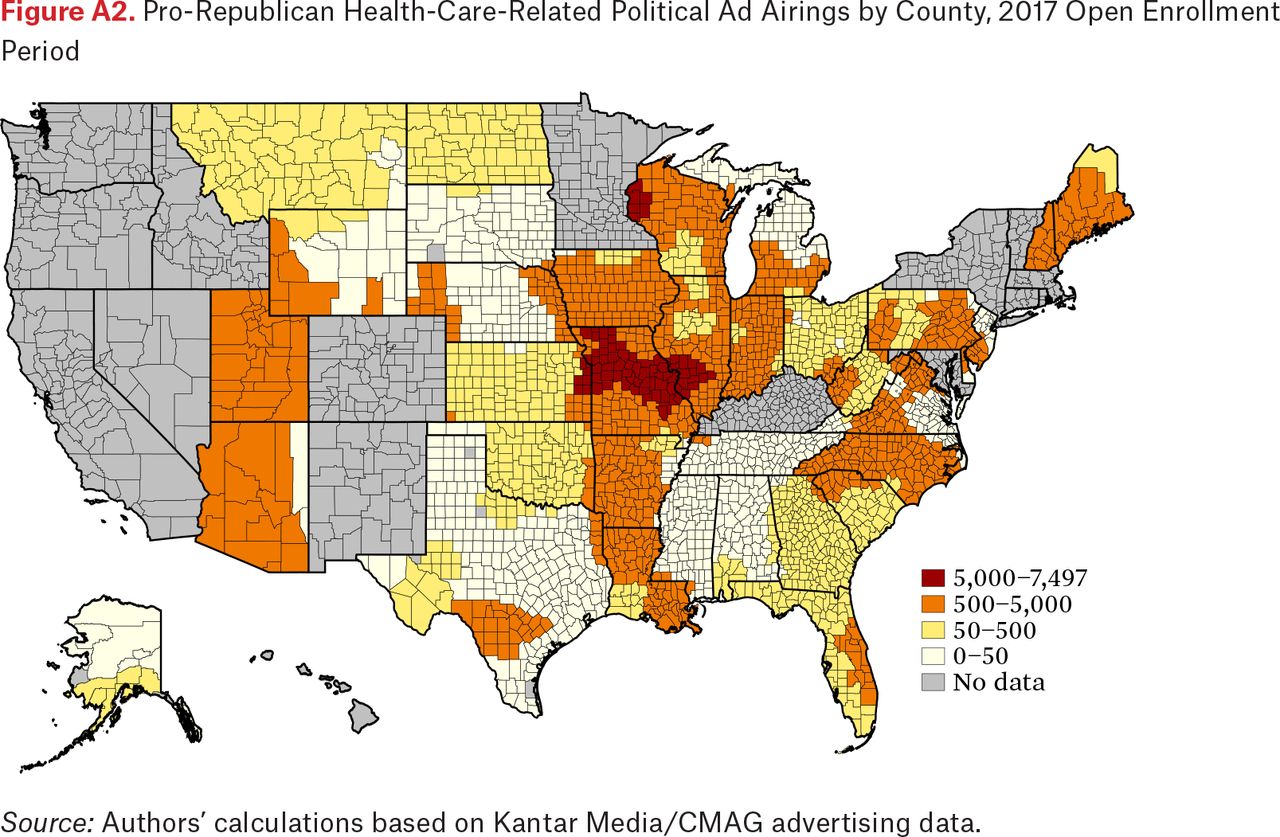
Health-care-related political advertising was much heavier during the 2015 and 2017 open enrollment periods (fall 2014 and fall 2016, respectively) than the other two years (fall 2015 and fall 2017), which coincided with primary election campaigns for federal office and some off-year gubernatorial elections. Although the pro-Republican and pro-Democrat ad volumes appear to be moderately correlated within each open enrollment period (r=0.55), the similarity of the population-weighted county average trends (see figure 4), which combine federal and gubernatorial contests, masks substantial variation in the underlying data. Areas that saw high volumes of pro-Republican health-care-related political advertising were not the same areas that saw high volumes of pro-Democrat advertising, as shown in county-level heat maps of these advertising volumes during the 2017 open enrollment period (see figures A1 and A2).
The counties included in our analysis vary significantly in terms of demographic and socioeconomic characteristics by whether they were in a crossover market (see figure 2 and table 1), a media market that was shared with part of any state that ever operated its own exchange (sixteen states and the District of Columbia). Counties within a crossover market had significantly lower population younger than sixty-five, lower unemployment, higher median household income, lower percentage of families in poverty, and lower uninsured rate among those younger than sixty-five than counties not in a crossover market. Despite the lower average population younger than sixty-five, they were more likely to be a metropolitan area based on the rural-urban commuting area codes. The divide in voting behavior was substantial; counties within a crossover market were significantly more likely to have had a majority vote for Obama in 2012 and less likely to have had one for Trump in 2016. Differences in advertising were also significant by crossover market status during these years. Crossover market counties, for example, saw fewer federal ads aired, more private non-Medicare, non-Medicaid ads aired (for 2015 to 2017) and more state ads aired for neighboring states as expected (see table A1).
Population-Weighted County Characteristics
Turning to descriptive information on enrollment (see table 2), we see that across all included counties, population-weighted average plan selections rose from 38,437 for 2015 to 40,370 for 2016 before falling to 36,236 by the 2018 open enrollment period. Counties within crossover markets had just under half (47 percent) as many plan selections on average as counties that do not share a media market with a state-based marketplace, which is similar to the difference in average population younger than sixty-five between the two groups (counties within crossover markets had only 56 percent of the average population of counties not in crossover markets). Crossover market counties also had lower pre-ACA uninsurance rates, and therefore fewer people who would have been looking for coverage (see table 1).
Population-Weighted Average County Enrollment
In table 3, we show average marginal effects from simple to progressively more complex models, moving from total health insurance advertising volume without regard for sponsor type (model 1) to our full model with federal, own and other state, and product-specific private advertising (model 3). These models demonstrate that both sponsor and the specific product marketed are consequential for whether advertising volumes are associated with Marketplace enrollment rate (plan selections per hundred thousand population younger than sixty-five). Specifically, model 1 finds no relationship between health insurance ad volume overall and the Marketplace enrollment rate. Model 2 disaggregates by sponsor type and we see large positive estimates of the marginal effect of federal and both types of state ads (own and other state) on the Marketplace enrollment rate; however, only the volume of ads from other states reaches statistical significance. Finally, model 3 disaggregates the private ads further by product, showing that private non-Medicare, non-Medicaid, and private Medicaid airings are positively associated with enrollment, offering evidence of a spillover effect across products.
Average Marginal Effects of Health-Insurance-Related Advertising on Marketplace Enrollment Rate, 2015 to 2018 Open Enrollment Periods
To further examine the idea of a spillover effect across state lines, rather than products, we estimate the full model (model 3 from table 3) with the crossover market stratification. Specifically, the fixed-effect regression estimates for our full model (see table A2) were used to estimate the average marginal effects (see table 4) and marginal effects by open enrollment period (see table 5) of each type of advertising separately during the 2015 through 2018 open enrollment periods. The federal marginal effect estimates, for all counties and by crossover market status, are the largest of all by far though they do not reach statistical significance. This seems to be driven largely by the small volume of Medicaid, CHIP, and Medicare ads that remain on air during the 2018 open enrollment period (see table 5). For own state ads, the average marginal effect across all counties was not significant, though it was when stratified by crossover market status, in both cases corresponding to approximately seventy-four additional plan selections per hundred thousand population younger than sixty-five for each additional one hundred ad airings (average marginal effect [AME] for counties not in a crossover market: 74.7, 95% confidence interval [CI]: 14.9, 134.5; AME for counties in a crossover market: 74.0, 95% CI: 20.3, 127.7) (see table 4). Each additional hundred airings of state-sponsored ads from other states were associated with twenty-six additional plan selections per hundred thousand population younger than sixty-five (AME: 25.7, 95% CI: 9.0, 42.3) (see table 4), driven by counties within a crossover market (AME: 30.1, 95% CI: 1.0, 59.3) in which other state advertising would be from a neighboring state-based marketplace. We find associations between private non-Medicare, non-Medicaid and private Medicaid (Medicaid managed care) advertising and Marketplace enrollment rate, contributing approximately seven (AME: 7.2, 95% CI: 0.3, 14.1) and 53 (AME: 52.6, 95% CI: 18.4, 86.8) additional plan selections per hundred thousand population younger than sixty-five for each additional hundred airings, respectively. The private Medicaid ad results are driven by the 2018 open enrollment period, in which federal Marketplace advertising had gone to zero (see table 5).
Average Marginal Effects of Health-Insurance-Related Advertising by Crossover Market Status on Marketplace Enrollment Rate, 2015 to 2018 Open Enrollment Periods
Marginal Effects by Open Enrollment Period of Health-Insurance-Related Advertising by Crossover Market Status on Marketplace Enrollment Rate
The relationship between political advertising and Marketplace enrollment rate is somewhat surprising and counterintuitive. We do not find a significant relationship between volume of pro-Democrat health-care-related political advertising and Marketplace enrollment rate (see tables 3 and 4). However, we do find a positive and significant association between pro-Republican ad airings and enrollment. For each additional hundred airings of pro-Republican health-care-related political ads, we see increases of Marketplace enrollment of approximately twenty-six additional plan selections per hundred thousand population younger than sixty-five (AME: 26.2, 95% CI: 11.1, 41.3). The relationship between pro-Republican health-care-related political ads and enrollment is driven by counties not in a crossover market (see table 4). Specifically, these results seem to be driven by the 2016 (ME: 68.7, 95% CI: 36.5, 100.9) and 2018 (ME: 38.4, 95% CI: 1.2, 75.5) open enrollment periods (see table 5). As a reminder, the 2016 and 2018 open enrollment periods correspond to the end of calendar years 2015 and 2017, which were not major election years. Political advertising during these periods was much lower overall than in the other two years (see figure 4), and to the extent it existed was concentrated in just a few places where federal primaries were off to an early start or there were off-year gubernatorial contests. For instance, the population-weighted average county-level volume of pro-Republican airings is less than twenty during the 2018 open enrollment period (see table A1). Because political advertising is also highly targeted (and therefore endogenous) and these volumes are so low, we are hesitant to make too much out of these counterintuitive findings because they may be picking up additional politically relevant characteristics not included in our model.
Finally, examining the insurance market-related control variables, our results indicate that changes in plan availability and pricing within a county over time are generally not associated with changes in enrollment (see table A2). A dollar increase in the benchmark premium was associated with approximately one additional plan selection per hundred thousand population younger than sixty-five (AME: 1.3; 95% CI: 0.2, 2.4). The number of plans, number of participating insurers, and silver spread in a county were not associated with changes in the Marketplace enrollment rate. However, we do not put too much emphasis on interpreting these control variables because of how small the year-to-year changes in these values are, and that marginal effects assume the other factors are held constant, which is generally not the case given that these are all likely correlated. They are also being driven by enrollment and claims performance in prior years, surrounding counties in which the insurer offers plans, and underlying characteristics of the county that may make it more vulnerable to insurer disruption (Abraham 2020), which may make these controls also endogenous. The codependent relationship between premiums and enrollment is complex, and a growing literature is exploring partisanship, differences between subsidized and unsubsidized premiums, and zero premium availability as among the factors related to enrollment behavior and plan choices (Anderson, Abraham, and Drake 2019; Branham and DeLeire 2019; Drake and Abraham 2019; Frean, Gruber, and Sommers 2017; Hinde 2017; Trachtman 2019).
DISCUSSION
This study combines data on television advertising, insurer competition, and plan pricing to measure the dose-response relationship of various types of health insurance and health-care-related political advertising on Marketplace enrollment, disentangling potentially countervailing policy effects (such as elimination of cost-sharing reductions and federal advertising). It is the first to our knowledge to extend both the time and geographic dimensions, stretching beyond a single state or open enrollment period, to examine whether federal investments in Marketplace advertising—and all other sponsors of insurance-related advertising—affect enrollment. Our findings imply that all health insurance advertising is not created equal and the source of the information matters. Specifically, we find state-sponsored advertising has the most robust evidence for being a positive driver of Marketplace enrollment. We find large estimates for the effect of federal advertising on Marketplace enrollment but they do not reach the threshold of statistical significance, being limited by the inherent difficulties in modeling causal effects in a complex information environment such as this. The seeming lack of an effect of federal advertising must be considered in the context of our inability to account for the endogeneity of advertising decisions across media markets and potential federal coordination with other sponsor types (such as states and insurers). We attempt to identify dose-response effects for federal advertising in an environment where we cannot identify the allocation mechanism across counties, relying only on within-county changes over time (which are always negative, given declining volumes of federal ads over the study period). Finally, we observe positive relationships between private (insurance company) advertising and Marketplace enrollment, particularly advertising for Medicaid products (though these are very low volume) and particularly in 2018 (when there was no federal investment in televised advertising). Our analysis includes only Marketplace enrollment and not applications for Medicaid through HealthCare.gov, for which there is ample evidence of positive spillover effects of government-sponsored advertising (Karaca-Mandic et al. 2017; Shafer et al. 2018). This is similar to other products, such as pharmaceutical advertising, that show evidence of spillover effects from one product to others in its same class (Shapiro 2018; Sinkinson and Starc 2019).
These findings have important practical implications for how policymakers and officials operate and support the Marketplace moving forward as well as political implications for the broader theoretical debates over privatized delivery of services resulting from public policy actions. The elimination of the federal role in advertising is consistent with broad trends in social policy toward privatization of services, or, more precisely, delegating the governance of services to private actors (Morgan and Campbell 2011b). As Kimberly Morgan and Andrea Campbell (2011b, 21) note, “Governance, and governing, is ultimately about power: the ability to make people do what they otherwise might not be able or inclined to do. Delegating governance is about moving this power from public to private actors.” Relying on the private sector to communicate about the availability of insurance plans through the Marketplace exemplifies the “submerged state” and obscures the governmental role in regulating and facilitating it (Mettler 2011). Indeed, failing to communicate about policy benefits (in this case, the federal Marketplace) exemplifies Suzanne Mettler’s typology of a case of perpetuating the submerged state after policy enactment (114).
Some argue that the ACA and the Marketplace are now a known quantity and investments in advertising are unnecessary, ignoring that advertising is a multibillion dollar industry with established brands still providing new messaging and product information to consumers on a daily basis. Young adults aging out of dependent coverage and other adults uninsured for the first time in many years (such as through job loss or change) may not have engaged with the Marketplace before and would benefit from awareness of the open enrollment period and availability of financial help (Dahlen 2015). Also, advertising may remain important for the Marketplace in the presence of ongoing political upheaval, legal challenges, and the like, which could leave consumers unsure of whether the ACA is still intact. In addition, even if the private sector can competently advertise the availability of enrollment opportunities—and indeed, promote enrollment (a proposition with mixed evidence based on this article and others, such as Lerman, Sadin, and Trachtman 2017; Shafer et al. 2018)—enrollment in plans is only one of many outcomes that might result from a communications campaign. Specifically, strategic political and media communication about governmental policies is needed not only to encourage uptake of that policy, but also to help the general public and beneficiaries alike understand what government provides. As Mettler (2011) argues, awareness of governmental programs is critical for democratic engagement, trust in government, and subsequent support for future reforms. Indeed, research has found that the privatized delivery of public programs can decrease awareness of that program. Specifically, Ashley Tallevi (2018) shows that greater state-level Medicaid managed-care penetration was associated with lower reporting of Medicaid receipt, indicating that privatized policy design can lead to less recognition of governmental benefit, the ultimate consequences of which bear on the level of and quality of civic engagement and public assignment of government accountability (Gingrich and Watson 2016). Thus, even if the private sector can promote short-term enrollment in programs, private advertisers are unlikely to promote awareness of the public nature of that program, which in turn can have broad and potentially long-term political consequences.
Our results also offer new evidence of the importance of considering multiple types of media information, and not solely focusing on insurance marketing, when considering how communication affects health insurance enrollment. Specifically, our findings offer suggestive, albeit uncertain evidence, that ad airings referencing health care for Republican candidates are associated with increases in Marketplace enrollment, but only in years when no major elections were held (fall 2015 and fall 2017, when the airings were low in volume and mainly for primaries and sporadic gubernatorial contests). During the general election contests when political ads are aired in higher volume, results are less consistent and suggest limited to no association of political ads on enrollment.
It is challenging to interpret the positive relationship between pro-Republican political ad airings and enrollment given both the low volumes of these airings and the counterintuitive direction of the association, given that the tone of Republican reference to the ACA is negative during this time period. However, it is important to consider a few caveats within which to interpret these findings. First, airings of political ads are likely to be endogenous with other types of media messaging or characteristics of the community, such as the interest in policy and politics in that community or engagement in health policy as communicated through third parties and social networks. Unlike in previous work by this study team (Karaca-Mandic et al. 2017; Gollust, Wilcock, et al. 2018), we did not have data on the volume of attention to health insurance policy on local broadcast news. Commentators have suggested that the better-than-expected enrollment in the 2018 open enrollment period in particular may be due to more news media attention across multiple channels, including television news during which many political ads are aired, during the failed legislative attempts to repeal and replace the law (Abelson and Sanger-Katz 2018). If local-level political advertising of health-care topics (and, particularly, predominantly negative ads from Republicans) correlates with more or better local news information about health-care options, this omitted variable—news attention to health insurance—may explain these results. Second, we are unable to distinguish the partisanship of the enrollees given that our findings are at the county level. Thus, we cannot distinguish among enrollees who identify as Republican who are exposed to anti-ACA political messaging and who enroll despite the counter message, those of any political orientation who are simply reminded of health insurance options regardless of its political rhetoric, or enrollees who identify as Democrats who enroll in a sort of backlash to the political messaging (or for anyone, regardless of partisanship, who enroll out of concern of the potential for later repeal). We know from other research that Republicans’ uptake of Marketplace plans may have been lower than Democrats’, which is challenging to square with our findings without knowledge of individual partisanship in our study (Lerman, Sadin, and Trachtman 2017; Trachtman 2019). Future work is needed to replicate these findings and continue to examine how the polarized information environment competes in shaping consumers’ health insurance behavior.
Finally, when interpreting any of these advertising associations, it is important to consider that there is likely to be interaction between and among the media types within and across communities. For instance, private advertising strategies may change in response to anti-ACA rhetoric. As Republicans fight the ACA, we might expect other sponsors to submerge the role (that is, hide mentions) of the ACA in their advertisements. We see indications of this submerging in data from the first three open enrollment periods, where 49 percent of ads mentioned the ACA in the first open enrollment period but only 31 percent in the second and third (Barry et al. 2018). There is likely an interaction between different types of communication, with the political communication strategies shaping insurer strategies, and vice versa. For instance, areas with more pro-Republican (anti-ACA) advertising may have contributed to even more “submerging” of the government role in insurer communication (Mettler 2011), suggesting that those who enrolled in Marketplace plans in those areas could be even less aware of the public nature of programs than in other geographic areas.
Limitations
This study has several limitations. Without specific knowledge about the strategy behind the overlapping advertising buys, we cannot identify causal effects of each type of advertising, nor can we account for potential dependence or simultaneity in advertising decisions. Advertising decisions may not be independent across sponsor types, through actual strategic coordination (federal and private sponsors) or correlated marketing decisions because of timing (pro-Republican and pro-Democrat health-care-related political advertising). For example, figure 4 shows that political ads went up for the 2017 open enrollment period and insurance ads went down—likely because of the declining “hole” (available space) for advertising because of the election. Pro-Republican and pro-Democrat ads are certainly not independent; they are in conversation with one another purposefully and strategically. Strategic behavior by insurers with respect to Marketplace entry and exit, and the resulting advertising decisions, are not well understood, an area we plan to examine in the future. Similarly, advertisement airings may be correlated with other outreach and enrollment activities. For instance, areas that saw more Medicaid content in ad airings may also have had more navigators or other enrollment outreach on the ground.
To further explore sources of variation in advertising, we exploit mismatches in state and media market boundaries to segment our sample of counties into those potentially subject to advertising spillovers from neighboring state-based marketplaces, providing insight into how the effects of federal and state ads may change in different settings. This approach has also been used in political science to observe individuals in non-battleground states, who would not otherwise be targeted by presidential campaigns, who live in a media market crossing over into a neighboring competitive state that receive the same barrage of messaging as residents from battleground states. This unintentional treatment of citizens in non-battleground states allows for comparison within the uncontested states of those who may have seen the advertising and those who could not have. This literature has demonstrated that this spillover treatment can affect political persuasion and campaign donations, but not necessarily voter turnout (Huber and Arceneaux 2007; Franz and Ridout 2010; Franz 2013; Urban and Niebler 2014; Krasno and Green 2008; Ashworth 2007). Also, with outcome data at the open enrollment period level rather than daily or weekly, we are unable to closely attribute the timing and magnitude of advertising by specific sponsors or sponsor types with the relevant behavior, which would certainly attenuate our effect estimates. Thus far, only one study using weekly data has been published (Shafer et al. 2018), likely due to the difficulty of getting more granular outcome data than what is made public. In addition, our exposure measures (ad airings) are at the ecological level and thus a crude measure of volume (gross ratings points would be preferable). We cannot ascertain whether individual enrollees were truly exposed to the insurance or political advertising (Niederdeppe 2014) and thus cannot speak to individual mechanisms through which information in the advertising environment leads to enrollment. In addition, as mentioned, our measures of advertising were restricted to those aired on television. We did not include advertising through other channels, such as digital advertising. Finally, the key dependent variable we examined—insurance enrollment—is only one of many consequential outcomes of marketing. Public attitudes, knowledge, and opinion about policy are also shaped by advertising from public and private sponsors (Fowler, Baum, Barry, et al. 2017), but not examined here.
Theoretical and Policy Implications
A growing body of research in political science and related disciplines examines the policy feedback effects of the Affordable Care Act. Policy feedback effect research is a broad category of inquiry that assesses how policies, once implemented, affect subsequent political outcomes because of changes to the beneficiaries affected directly by the policy and changes in widespread interpretation or understanding of the policy context (Campbell 2012; Chattopadhyay 2019; Mettler and Soss 2004; Oberlander and Weaver 2015). The emerging evidence examining the feedback effects of the ACA suggest that it has had differential effects on enrollment and opinion based not only on where someone lives (for example, living in a state that did or did not expand Medicaid) (Hopkins and Parish 2019), but also based on their partisanship (Hopkins and Parish 2019; Lerman, Sadin, and Trachtman 2017; Sances and Clinton 2019). Gains in coverage attributable to the ACA were more likely in areas that tended to vote Democratic and in states that did not expand Medicaid, and Democrats and independents gained insurance at higher rates than Republicans (Sances and Clinton 2019). Republicans were also less likely to gain private insurance through the Marketplace than through private channels (off-exchange plans, brokers), likely because they prefer market-based insurance models that make the role of government less obvious (Lerman, Sadin, and Trachtman 2017). A previous study examining only the first open enrollment period found that negative political advertising (all anti-ACA) was associated with lower uptake of Marketplace plans (Gollust, Wilcock, et al. 2018), suggesting that partisan uptake of insurance may be mediated by the information environment. Our findings, in contrast, suggest that pro-Republican health-care-related political advertising is positively associated with county-level Marketplace enrollment in the 2016 and 2018 open enrollment periods. Another recent study suggests a health insurance-partisanship relationship in the other direction, with county-level health insurance gains being associated with increases in voting for the Democratic presidential candidate (Hollingsworth et al. 2019). Local preferences and experiences with the ACA can also directly feed into the policies proposed by leaders attempting to shift federal policy in the direction of their constituencies, such as Medicaid buy-in versus work requirements (Fording and Patton 2020).
Overall, the findings of this study—when considered in light of the growing body of evidence on the political and policy effects of the ACA—suggest a few key implications. The ACA has been such a controversial issue for the past decade that interactions between prior knowledge, partisan attitudes, and repeated exposures to information about health insurance and the ACA makes marketing (or educational strategies, more generally) difficult because what is considered a “credible source” may vary widely among individuals (Kumkale, Albarracín, and Seignourel 2010). Tailoring communications around the characteristics of the target population becomes extremely important in this type of environment. Existing evidence, including this study, support the potential for significant spillover effects in both directions at the state level, such as increasing Marketplace enrollment through Medicaid advertising (as we show) and possibly Medicaid enrollment through Marketplace advertising as well (Karaca-Mandic et al. 2017). States may be seen as a more credible source of information in this hyperpolarized environment and in a better position to effectively market to their populations (Pacheco, Haselswerdt, and Michener 2020). Overall, addressing the information environment related to the ACA is complicated and requires policymaker attention to both intended and unintended consequences. For instance, one implication of this study is that the funds collected by the 3.5 percent user fee levied on insurers in federally facilitated marketplace states could be redirected to states to undertake their own marketing efforts and support Marketplace stability. However, given the existing heterogeneity in how states are implementing the ACA, such as Medicaid expansion, 1115 waivers, and 1332 waivers (Fording and Patton 2020) and this emerging evidence of intrastate variation in marketing effectiveness, policies should be designed to attend to the potential for disparities in effort and execution across states.
Appendices
Population-Weighted County Average Health Insurance and Health-Care-Related Political Advertising by Crossover Market Status, 2015 to 2018 Open Enrollment Periods
County-Level Fixed-Effect Estimates of Advertising on Marketplace Enrollment Rate, 2015 to 2018 Open Enrollment Periods
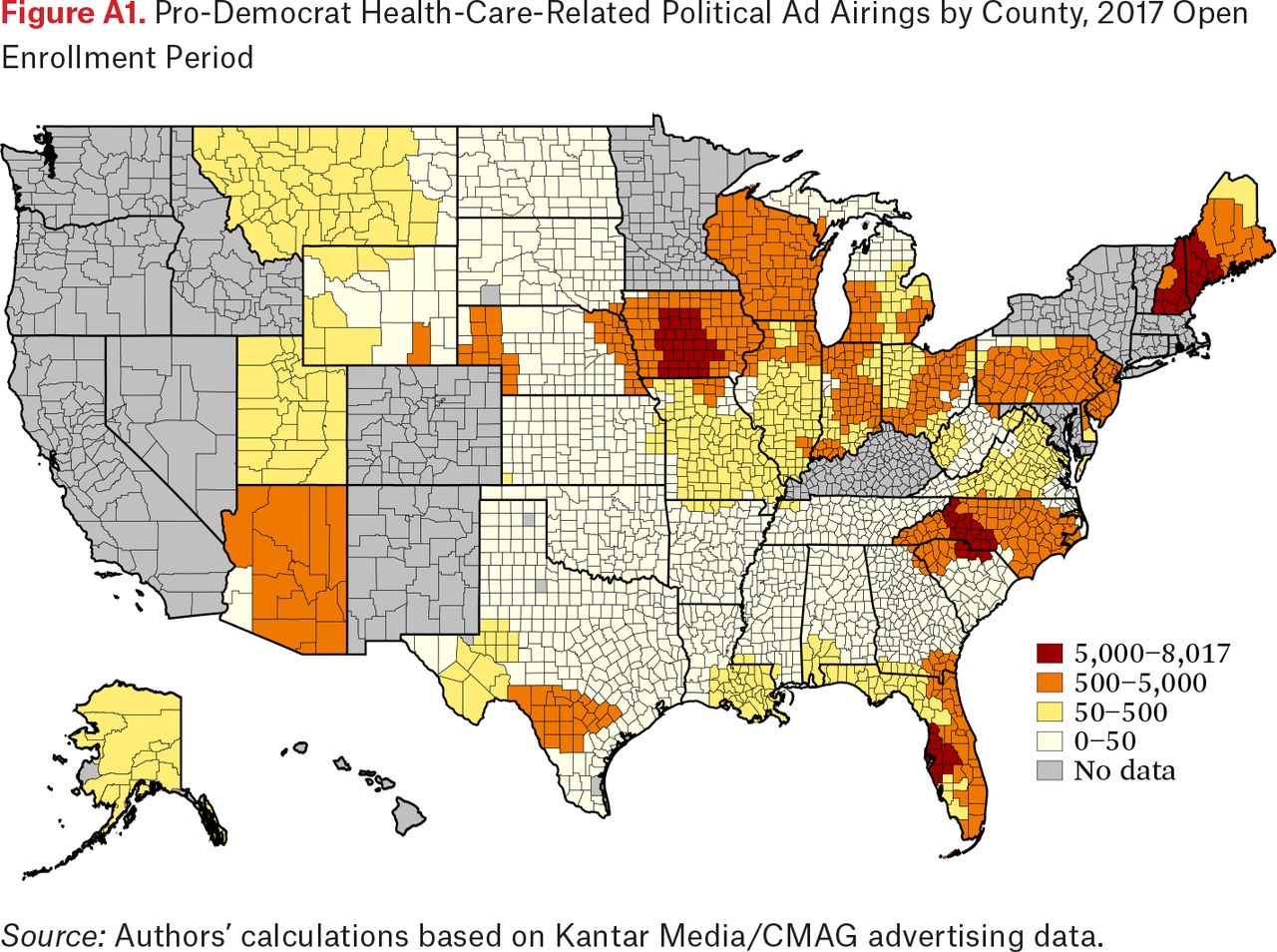
Pro-Democrat Health-Care-Related Political Ad Airings by County, 2017 Open Enrollment Period
Source: Authors’ calculations based on Kantar Media/CMAG advertising data.

Pro-Republican Health-Care-Related Political Ad Airings by County, 2017 Open Enrollment Period
Source: Authors’ calculations based on Kantar Media/CMAG advertising data.
FOOTNOTES
↵1. National Federation of Independent Business v. Sebelius 567 U.S 519 (2012).
- © 2020 Russell Sage Foundation. Shafer, Paul R., David M. Anderson, Seciah M. Aquino, Laura M. Baum, Erika Franklin Fowler, and Sarah E. Gollust. 2020. “Competing Public and Private Television Advertising Campaigns and Marketplace Enrollment for 2015 to 2018.” RSF: The Russell Sage Foundation Journal of the Social Sciences 6(2): 85–112. DOI: 10.7758/RSF.2020.6.2.04. The authors acknowledge Wesleyan University and the Robert Wood Johnson Foundation for support to establish the advertising data infrastructure used in this study (State Health Access Reform Evaluation, 72179). This work has also been supported in part by the Russell Sage Foundation (1808-08181). Any opinions expressed are those of the authors alone and should not be construed as representing the opinions of the Robert Wood Johnson Foundation or Russell Sage Foundation. Direct correspondence to: Paul R. Shafer at pshafer{at}bu.edu, 715 Albany St., Boston, MA 02118; David M. Anderson at dma34{at}duke.edu, 100 Fuqua Dr., Box 90120, Durham, NC 27708; Seciah M. Aquino at saquino{at}lchl.org, 1225 8th St., #375, Sacramento, CA 95814; Laura M. Baum at lbaum{at}wesleyan.edu, 45 Wyllys Ave., Middletown, CT 06459; Erika Franklin Fowler at efowler{at}wesleyan.edu, 45 Wyllys Ave., Middletown, CT 06459; and Sarah E. Gollust at sgollust{at}umn.edu, 420 Delaware St. SE, MMC 729 Mayo, Minneapolis, MN 55455.
Open Access Policy: RSF: The Russell Sage Foundation Journal of the Social Sciences is an open access journal. This article is published under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.