
Abstract
This article examines the impact of both the Medicaid expansion and the private insurance-related components of the Affordable Care Act (ACA) on voter turnout and registration. We employ a difference-in-difference-in-differences identification strategy exploiting variation over time, state Medicaid expansion status, and within-state local area pre-ACA uninsured rates. Using data between 2006 and 2016 from the November Current Population Survey and the Census Bureau’s Small Area Health Insurance Estimates, our results suggest little effect of the ACA on voter turnout or registration.
According to the Centers for Medicare and Medicaid Services, the share of U.S. gross domestic product devoted to health-care spending rose from 13.4 to 17.3 percent between 2000 and 2009. Thus, the major changes to such an important part of the economy brought on by the passage of the Patient Protection and Affordable Care Act (ACA) in 2010 were anticipated to have broad social, political, and economic effects extending beyond the health-care sector itself. Despite this, most of the existing ACA literature has focused on effects within the health-care sector. Moreover, much of the literature interested in estimating causal effects has examined the impact of individual components of the ACA, such as the Medicaid expansion, alone (Kaestner et al. 2017; Simon, Soni, and Cawley 2017; Maclean and Saloner 2019).
Fewer causal studies examine not only the ACA Medicaid expansion, but also the other private components of the ACA implemented in 2014 at the same time. Several works document gains in health insurance coverage coming from both the Medicaid expansion and the other components of the ACA (Courtemanche et al. 2016, 2017, 2019b; Frean, Gruber, and Sommers 2017). Molly Frean, Jonathan Gruber, and Benjamin Sommers (2017) estimate that 60 percent of the coverage gains occurring in 2014 and 2015 can be attributed to the Medicaid expansion with the other 40 percent being attributed to subsidized Marketplace coverage. Others have examined the impact of the ACA on self-assessed health, access to care, and risky health behaviors (Courtemanche et al. 2018a, 2018b, 2019a). These studies tend to find that any impact of the ACA on these outcomes is driven by the non-Medicaid expansion components of the law.
Looking beyond effects within the health-care sector, the purpose of this article is to examine the impact of the ACA on civic engagement through political participation, specifically voter turnout and registration. The 2010 congressional election, where Republicans picked up sixty-three seats in the House of Representatives, may have served as a referendum on the ACA. Conversely, Democrats picked up forty seats in the 2018 congressional election where health care and the potential repeal of the ACA were major issues. During the 2018 election cycle, health care was the dominating issue in campaign ads, where pro-Democratic ads featured the issue 47 percent of the time, and the overall issue of preexisting conditions was front and center.1 Those most likely to be uninsured prior to the ACA (the young, minorities, and the low income) traditionally have low voter turnout. If the debate surrounding the ACA mobilized these new constituencies, then changes in political participation due to the ACA may have broader social impacts beyond changes in health policy.
Our primary empirical approach involves estimating difference-in-difference-in-differences (DDD) models, with differences coming from time, state Medicaid expansion status, and local area pre-ACA uninsured rates (Courtemanche et al. 2017). The third difference leverages the fact that the ACA is expected to have a stronger impact in areas with higher pre-ACA uninsured rates.2 This approach allows us to identify the effect of the private components of the ACA separately from the Medicaid expansion. Our baseline DDD model includes the full voting eligible population (U.S. citizens age eighteen or older) using the November 2006–2016 Current Population Survey (CPS). We also consider heterogeneity in the impact of the ACA within demographic groups (age, race, and income). Focusing on subgroups can help identify particular constituencies who may have responded to the ACA in different manners.
Our empirical approach and use of the CPS extends the ACA and voting literature in several ways. First, we estimate the impact of both the Medicaid expansion and the private components of the ACA on political participation. The ACA-related gains for private coverage for more affluent individuals affected approximately eleven million Americans (CMS n.d.). Second, our principal results rely on individual-level microdata, allowing us to control for a broad set of individual covariates as well as by subgroup and type of election. Finally, we include controls for economic and political environment, including voting reforms that may separately affect turnout and registration.
Across a variety of specifications, we typically find small and insignificant effects of the ACA on turnout or registration, in contrast to earlier work. But we don’t know why. The evolving literature on Medicaid’s valuation and the health effects of the ACA is mixed (Finkelstein, Hendren, and Shepard 2019; Gruber and Sommers 2019), possibly suggesting a smaller mobilization effect than one may anticipate. The political science concept of the “delegated” or “submerged” welfare state suggests that those gaining coverage may not be fully aware that they are benefiting from a public program (Mettler 2011; Morgan and Campbell 2011).
PREVIOUS LITERATURE
To date, two published studies examine the impact of the ACA’s Medicaid expansions on voter turnout and registration. Jake Haselswerdt (2017) examines voter turnout in a difference-in-difference (DD) framework (relying on variation across states and over time) with district-level turnout data from the 2012 presidential election and 2014 congressional election for the 435 congressional districts across all fifty U.S. states. He finds robust evidence that increased Medicaid enrollment is associated with higher turnout and likely due to both increased participation by new beneficiaries and backlash. The point estimates imply that for every hundred individuals who gained Medicaid coverage due to the ACA expansions, between fifty-one and 113 others turned out to vote in 2014 (Haselswerdt 2017, 683).
This enormous magnitude could potentially reflect spillovers, newly engaged Medicaid recipients spreading enthusiasm (or reflecting backlash) to others whose coverage status did not change. Alternatively, it could be driven by methodological issues. The DD research design assumes that, conditional on controls, changes in voter turnout between 2012 and 2014 would have been the same in expansion and non-expansion states in the absence of the ACA. Given only one period of pre-ACA data, it is not possible to examine pretreatment trends to evaluate the validity of this assumption. Moreover, comparing a presidential election year with a congressional election year increases the risk of confounding. If the dip in turnout in congressional relative to presidential elections differs systematically between Republican- and Democratic-majority states, the identifying assumption would be violated. In contrast, we use a DDD research design that allows for differential trends between expansion and non-expansion states as long as this difference is uncorrelated with pre-ACA uninsured rates. Moreover, we separately examine both presidential and congressional elections with multiple pretreatment years.
Joshua Clinton and Michael Sances (2018) examine Medicaid’s effect on turnout and registration using a DDD framework (relying on variation across states, over time, and by the percentage of near-poor adults in a county) and county-level elections data for thirty-two states, comparing changes in the 2010 and 2014 congressional elections and changes in the 2012 and 2016 presidential elections. In their most carefully controlled specifications, they find that the ACA Medicaid expansion increased voter registration by up to 4 percentage points in 2014 (effects persisting through 2016) and increased voter turnout in 2014 by up to 2.4 percentage points, though this estimate is not statistically significant. Further, they do not find any impact on voter turnout in 2016.
Their methodology is similar to ours in that it includes a third difference meant to capture treatment intensity and separately examines presidential and congressional elections. Accordingly, their magnitudes are much more modest than those of Haselswerdt (2017). Nonetheless, this article contributes in several ways. First, we move beyond the Medicaid expansion and estimate the effect of the ACA’s expansion of private coverage. Second, by using individual rather than aggregate data, we are able to examine how the effects differ across demographic groups. Next, we include multiple pretreatment periods to enable the evaluation of pre-trends. Finally, we use a more direct intensity measure—pretreatment uninsured rate rather than proportion low income—in an effort to obtain more precise estimates.
Several single-state studies also explore the impact of Medicaid prior to the ACA on turnout and registration. Katherine Baicker and Amy Finkelstein (2018) find that new Medicaid coverage for previously uninsured, non-elderly adults in Oregon led to an increase in voter turnout in the 2008 presidential election, but not the 2010 congressional elections. They identify the impact of Medicaid on individuals from the random assignment of coverage generated from the Oregon Health Insurance Experiment, and merge lottery assignment and Medicaid coverage status to individual voter data on registration and turnout. The causal impact of individual Medicaid coverage is to increase the individual’s likelihood of voter turnout in 2008 by up to 2.5 percentage points (from a baseline of roughly 33 percent), with larger effects for some subgroups. The impact on voter turnout in November 2010 suggests a decline in voting, but the point estimates are not significant. The impact on voter registration is roughly the same magnitude as on turnout, although the results are not significant. Haselswerdt and Jamila Michener (2019) examine major changes to TennCare that, by late 2005, led to the removal of 170,000 Medicaid adult recipients in Tennessee. They use voter turnout data across the ninety-five counties in Tennessee in the 2006 and 2002 congressional elections (which also coincided with the gubernatorial election); their point estimates imply that for every hundred individuals who lost TennCare coverage, between twenty-four and thirty-six fewer individuals voted.
Although the results from these two single-state studies suggest the same-signed direction (expanding Medicaid leads to short-run increases in voting, and contracting TennCare leads to short-run decreases), the estimates are different by an order of magnitude. Possible explanations include heterogeneous treatment effects across states, a lack of symmetry in the effects of expansions and contractions, or biased estimates in the latter study from differential underlying trends in voter turnout between heavily and lightly treated Tennessee counties.
In summary, most existing studies focus exclusively on Medicaid reforms and find mixed effects on turnout and registration, although the data, methods, magnitudes, and statistical significance vary substantially. Evidence from the previous ACA literature suggests short-run positive impacts that fade over time; evidence from Medicaid variation outside the ACA suggests mixed impacts.3 To date, little focus has been on the full effect of the ACA, even though substantial numbers of people gained private coverage, often highly subsidized. Given that the ACA represents a coverage expansion, we might expect our results to be more closely aligned to those from the Oregon study (Baicker and Finkelstein 2018) than the Tennessee study (Haselswerdt and Michener 2019).
LEGISLATIVE HISTORY
President Obama signed the ACA into law on March 23, 2010. Although the major provisions are well known, we highlight a number of features where the ACA could create political constituencies that affect political participation. The ACA implemented some popular, immediate reforms in 2010 related to young adults, lifetime limits, and individuals with preexisting conditions. The dependent coverage provision allowed young adults to be covered by their parent’s health insurance plan until age twenty-six. This provision affected approximately 938,000 young adults (Antwi, Moriya, and Simon 2013) and would potentially create constituencies with both young adults and their middle-aged parents.4 The ACA also eliminated lifetime dollar limits on insurance coverage for essential benefits such as hospital stays. More than 16 percent of covered workers with single coverage had a lifetime limit of $2 million or less in 2009; overall, 59 percent had some lifetime maximum (Claxton et al. 2009). The ACA also established a transitional program known as the Pre-Existing Condition Insurance Plan that launched in summer 2010 and ended in 2014 with the major rollout of the ACA. It targeted those who were uninsured for at least six months, had a preexisting condition, and were denied coverage by a private insurance company.5 At its peak, in February 2013, approximately 115,000 individuals were enrolled (CMS n.d.).
Based on the June 2012 decision in National Federation of Independent Business v. Sebelius, several major parts of the ACA were clarified.6 Most important, the Supreme Court upheld the individual mandate to buy health insurance as a constitutional exercise of Congress’s taxing power. It also ruled that expanding Medicaid was not a valid exercise of Congress’s spending power because it would coerce states to accept the expansion or risk losing existing Medicaid funding.
The ACA rollout in 2014 included both a private portion and a public portion. The private portion improved the functioning of the nongroup health insurance market for consumers who did not have access to employer-provided or public coverage (Gruber 2011). Provisions included community rating, guaranteed issue, and minimum coverage requirements. It also established a health insurance marketplace, commonly referred to as the federal exchange. Each state was given the option of establishing its own insurance exchange; fifteen did so in 2014 (KFF 2019b). It created penalties for those who did not comply with the individual mandate, which could reach as high as the annual premium for the national average price of a bronze exchange plan. It also created sliding scale subsidies in the form of premium tax credits for consumers with incomes between 100 and 400 percent of the federal poverty level (FPL) who do not qualify for other affordable coverage, such as Medicaid. It also created cost-sharing reductions for individuals who purchased a silver plan in the exchange and had incomes under 250 percent of the FPL. The public portion expanded Medicaid. In states that opted to expand Medicaid via the ACA, Medicaid is available up to 138 percent of the FPL (for private coverage, subsidies are available for those between 138 and 400 percent of the FPL). This suggests a major expansion of Medicaid eligibility via the ACA for low-income childless adults.
Both the private and public portions of the major ACA rollout strengthen the insurance market, which in turn creates new constituencies that could be mobilized to vote. Although the current uninsured are the most natural constituency from these provisions, the impact likely goes much further. Using administrative data from the Internal Revenue Service for 2015, Ithai Lurie and James Pearce (2019) classify 26.9 million non-elderly individuals as uninsured as at a “point of interview” but a much larger 72.9 million as uninsured “ever in year.” Volatility in income, insurance affordability, family structure, and job security put many currently insured people at risk of losing coverage.
CONCEPTUAL EFFECTS: HOW SHOULD THE ACA AFFECT POLITICAL PARTICIPATION?
Why would the expansion of the ACA impact political participation? We draw on insights from the civic volunteerism model (CVM), which Kay Schlozman, Henry Brady, and Sidney Verba (2018) summarize, to explore this issue. The CVM explains forms of political participation (such as voter turnout or registration, volunteering time, or contributing money) as arising from three factors. The first is resources (time, money, and civic skills). The second is political engagement (political interest, information, efficacy, and partisanship).7 The third is mobilization (recruitment requests that can come through formal political campaigns or informal social networks through which one interacts with friends, family, neighbors, and so on). These factors in turn interact with family background, schooling, and adult institutions, as well as particular political issues. All three components—as well as their interactions—lead to insights for how the ACA expansions may (or may not) increase voter turnout or registration.
When segments of the population focus on a political issue with personal benefit, there is potential for much greater political participation. Schlozman, Brady, and Verba (2018, 77–78) find that “having a stake in a particular policy . . . has a strong additional impact on the likelihood of being active on issues related to that policy.” Specifically for voter turnout, they find that political interest, political information, and partisan strength all have substantial effects.8
This would suggest that targeted beneficiaries of the ACA might increase their voter turnout or registration because the ACA increased their resources by providing health insurance coverage. Of course, this depends on several factors. First, those gaining coverage through the ACA must value this coverage to perceive their resources as increasing. Second, they must also recognize that this gain in coverage is due to the ACA. Third, it depends on how the increase in resources interacts with the other factors in the CVM. For example, if the other factors tend to push an individual away from voting, then an increase in resources would have to be large enough to convince this individual to vote.
Political engagement is particularly important in influencing turnout. One element of engagement is information. As mentioned, potential voters gaining coverage via the ACA may or may not associate this benefit with the ACA. For example, Jacqueline Chattopadhyay (2017) shows that the ACA dependent care provision does not affect political participation of young people, perhaps because the coverage is provided through employer-provided rather than public plans. Similarly, it is possible that those who purchased subsidized private coverage in the ACA marketplace did not associate the low premiums they received with the ACA.9
Why would an individual gaining coverage through the ACA not attribute this benefit to the ACA? An answer can be found in the concept of the “delegated” or “submerged” welfare state (Mettler 2011; Morgan and Campbell 2011). The concept suggests that those gaining public benefits may not be fully aware that they are receiving them from a public program. This stems from the fact that it is becoming increasingly common for public goods to be provided privately, thus obscuring whether the goods themselves are public or private. Someone gaining insurance via a subsidized Marketplace plan administered by a private insurance company, such as Anthem or United, for example, may not consider the coverage to be public. If this is the case, then we may not expect those benefiting from the ACA to respond by changing their political participation.
Another component of political engagement is efficacy. It is also possible that the programs lack efficacy, signaling that the government does not listen to or care about people like the beneficiary. The individual mandate may be seen as negative, as an infringement on personal liberty, even though the intent is to help consumers by stabilizing insurance markets from adverse selection. Although millions of poor individuals signed up for Medicaid in expansion states, the program itself may be viewed as stigmatizing or poorly run, in turn sending a message to beneficiaries that they do not deserve a voice in politics. Michener (2017) argues that the Medicaid program conveys disempowering messages.10
The third factor in the CVM is mobilization (see Rosenstone and Hansen 2002). Mobilization efforts on both sides of the political debate surrounding the ACA have been ongoing since before 2010. Those who earn a living in the health-care sector may experience greater mobilization given that changes to health policy may affect them both personally and professionally. Organizations such as the American Medical Association and the American Association of Retired Persons, as well as lobbyists associated with the pharmaceutical industry and the insurance industry, are also involved in mobilization efforts. Presumably, these sorts of efforts will differentially affect different types of individuals.
As suggested, it is important to consider the interaction of these three factors rather than each in isolation. For example, even if Medicaid is viewed as efficacious and the information about the ACA’s role in providing the benefit is understood, some constituencies lack resources to translate increased information into higher political participation. Schlozman, Brady, and Verba (2018) find evidence that recipients of means-tested benefits, who tend to have less education and lower income, are relatively uninterested in and uninformed about politics. The bump given to their political participation by their interest in issues is not enough to overcome their other resource deficits, such as lack of time or money. Similarly, even if the ACA improved financial security or health status for Medicaid beneficiaries (thus, increasing resources to new beneficiaries), the gain in resources may not have been enough to increase political participation, given the initial resource deficits. For private coverage, the effects on resources is less clear. Gaining private coverage would also improve financial security, although some beneficiaries choose plans that entail substantial out-of-pocket costs (Pauly 2017). Thus, private coverage reduces the risk an individual faces (and affects the variance of expenses), but the mean effect on expenditure may not change substantially. In sum, the CVM suggests important interrelated factors that influence the effect of the ACA on voter turnout.
DATA
Our principal dataset is the 2006 to 2016 Voting and Registration Supplement to the CPS, produced in November of even-numbered years. Aram Hur and Christopher Achen (2013) argue that this supplement is widely respected and often used for studying voting behavior given to its data quality, sample sizes, and response rates. We restrict our empirical analysis to the vote-eligible population (VEP).11 The CPS asks a number of questions about voter behavior; we focus primarily on voter turnout, worded as “In any election some people are not able to vote because they are sick or busy or have some other reason, and others do not want to vote. Did (you/name) vote in the election held on Tuesday, November ——?” In some specifications, we examine whether the ACA affected voter registration, derived from the CPS question “(Were you/Was name) registered to vote in the November —— election?”
In our primary analysis, we follow conventional academic coding rules by restricting the VEP sample who answer the turnout question with yes or no, excluding individuals who respond with don’t know, refused, and no response. Official Census Bureau reports categorize these answers into no, in part to due to well-known overreporting of voting driven by social desirability bias (Ansolabehere and Hersh 2012). Following the recommendation of Hur and Achen (2013), we drop all categories of missing turnout response, and adjust the CPS survey weights for overreporting using files from the United States Elections Project.12
The CPS is well suited to studying the full impact of the ACA on voter turnout using an approach similar to that of Courtemanche and his colleagues (2017, 2018a, 2018b, 2019a, 2019b) because it provides geographical information at the state level for all respondents, and at the county level for approximately 40 percent of respondents. Over the entire 2006 to 2016 period, the CPS identifies 368 counties within the United States; however, only 193 are consistently identified across all six surveys. These 193 tend to be relatively large and represent around 38 percent of the total U.S. population, the average county population being around 615,000 (approximately nine times larger than the counties or county-equivalents that are not identified). Following earlier work, we create a “rest of state” category for respondents who are either in an unidentified county or in one of the 175 counties identified only intermittently from 2006 to 2016. Ultimately, we have 242 geographic areas in our analysis. Among the vote-eligible population, we extract questions on voter participation and registration along with demographic and socioeconomic characteristics. The covariates include respondent’s age, marital status, sex, educational attainment, race, employment status, and family income. We also control for whether the respondent self-reported voting status.13
We append a number of health policy variables that vary at the state or substate level to the CPS microdata. One key variable is pretreatment uninsured rate. For each of the local areas, we use the 2013 Small Area Health Insurance Estimates (SAHIE) to compute the uninsured rate for adults age eighteen through sixty-four, as well as smaller subgroups age eighteen through thirty-nine, forty through forty-nine, and fifty through sixty-four, when appropriate (U.S. Census Bureau 2017). Variation in the rate of uninsured adults age eighteen through sixty-four across areas is substantial, varying from 5.3 percent to 51.1 percent, rates for younger adults being somewhat higher and those for older adults somewhat lower. Another important variable, commonly used in ACA studies, indicates the state-optional Medicaid expansions. Following Courtemanche and his colleagues (2018a), we code twenty-one states as non-expansion if they had not expanded by early 2015. According to the Kaiser Family Foundation (2019c), twenty-eight states (including the District of Columbia) participated in the Medicaid expansion in 2014, two others implemented in early 2015.
We also include several economic and political variables. One is the unemployment rate (which varies by local area and year) from the Bureau of Labor Statistics (2018). The local unemployment rate ranges from 2.0 percent to 17.2 percent. We also parameterize three political variables related to the voting process, each of which varies by state and year. The first relates to voter identification laws. We follow the National Conference for State Legislatures (NCSL) in classifying states in each election year as having strict laws requiring photo IDs, nonstrict laws requiring photo IDs, strict laws requiring nonphoto IDs, nonstrict laws requiring nonphoto IDs, or no ID requirement (Underhill 2020). For the 2018 election, thirty-five states had laws requesting or requiring voters to show some form of identification at the polls. The remaining fifteen states use other methods to verify voters, such as checking a signature against information on file. In our primary specification, we control for states not having any ID requirement. Between 2006 and 2016, the number of states that adopted an ID requirement steadily grew from twenty-three to thirty-three. We also use the NCSL (2019b) to classify states with early voting. We explored definitions of early voting, which in Paul Gronke, Eva Galanes-Rosenbaum, and Peter Miller (2007) mean no-excuse in-person early voting, no-excuse absentee, vote-by-mail, or in-person absentee voting. The number of states with early voting has remained nearly constant, thirty-six in 2006 and thirty-eight in 2016. Finally, a recent innovation to voting is automatic registration; some states automatically register a person to vote, unless the person actively decides to opt-out of voter registration (NCSL 2019b). Although seventeen states and the District of Columbia authorized automatic registration by December 2018, only Georgia and Oregon implemented such laws in time for the 2016 election (Brennan Center for Justice 2019).
Virtually all studies recognize that competitiveness of elections and coattail effects from presidential, senatorial, or gubernatorial elections are likely to affect voter turnout (see, for example, Clinton and Sances 2018; Haselswerdt and Michener 2019). We control at the state-year level for a number of variables related to competitiveness, coattails, and partisanship. First, following Clinton and Sances (2018), we separately estimate the impact of the ACA for congressional elections (2006, 2010, and 2014) and presidential elections (2008, 2012, and 2016). Second, for every state and year in our sample, we control for (when available) the difference in aggregate vote percentage for the candidates finishing in first and second place for presidential, senatorial, and gubernatorial elections.14 Third, we control for a state’s partisanship by computing the difference in a state’s Republican vote percentage and Democrat vote percentage using the 2000 and 2004 presidential elections, prior to our CPS sample. We interact this state-level characteristic with year dummies in all specifications.
Table 1 characterizes voter participation in the CPS over time for the full population age eighteen and older, as well as by age group, Medicaid expansion status, and pretreatment uninsured rate. To preserve comparability with published Census Bureau reports (File 2015, 2018), we recode invalid voting responses as nonparticipation. Over the period examined, participation was approximately 17 percentage points higher in presidential elections than congressional elections; on average, approximately 45.1 percent participate in congressional elections and 62.3 percent in presidential elections. The highest participation was in the 2008 election, when 63.6 percent of the vote-eligible population participated. Participation increases markedly with age, especially in congressional elections. On average, the youngest group (age eighteen through thirty-nine) had a 52.4 percent turnout in presidential elections, compared with 71.1 percent for those age sixty-five and older. The youngest group also had substantially lower comparative participation in congressional elections; the gap in voter participation for those age eighteen through thirty-nine was 23.1 percentage points (29.3 percent versus 52.4 percent), relative to just 10.2 percentage points (60.9 percent versus 71.1 percent) for those age sixty-five and older. States that expanded Medicaid by 2015 (expansion states) had somewhat higher participation rates in congressional elections than non-expansion states, but virtually no difference in presidential elections. States with below-median uninsured rates had higher participation in all elections.
Voter Participation Across Elections
As to the impact of the ACA, table 1 reveals that the overall effect may be small and sensitive to the type of election. Voter participation in presidential elections is remarkably stable, though somewhat higher in the historic 2008 election. Voter participation has steadily declined in congressional elections for many demographic groups; in addition, disparities in participation across demographic groups are significant (File 2015). Voter participation drops off more pronouncedly for Medicaid expansion states relative to non-expansion states after ACA implementation in 2014. However, in the group of states with low uninsured rates (where the impact of the ACA should be smaller), we continue to see much larger voter participation changes in Medicaid expansion states compared with non-expansion states. This potentially suggests that the expansions are not responsible for the decline in voter participation.
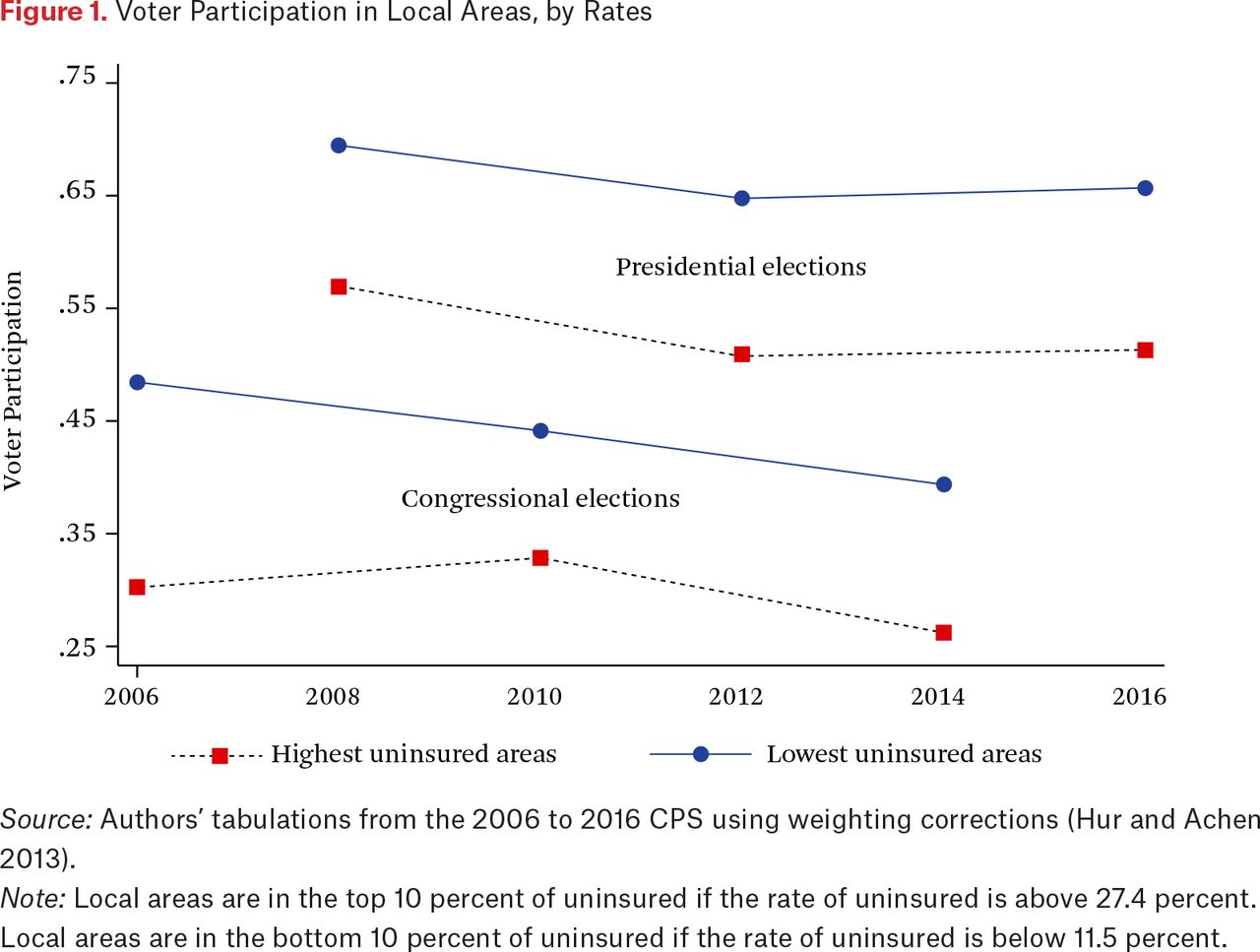
Figure 1 draws on the CPS sample used in the empirical analysis (described further). Localities with low uninsured rates clearly have higher voter turnout than those with high rates.15 However, difference is minimal in the trends from the pre to post period for either presidential or congressional elections.
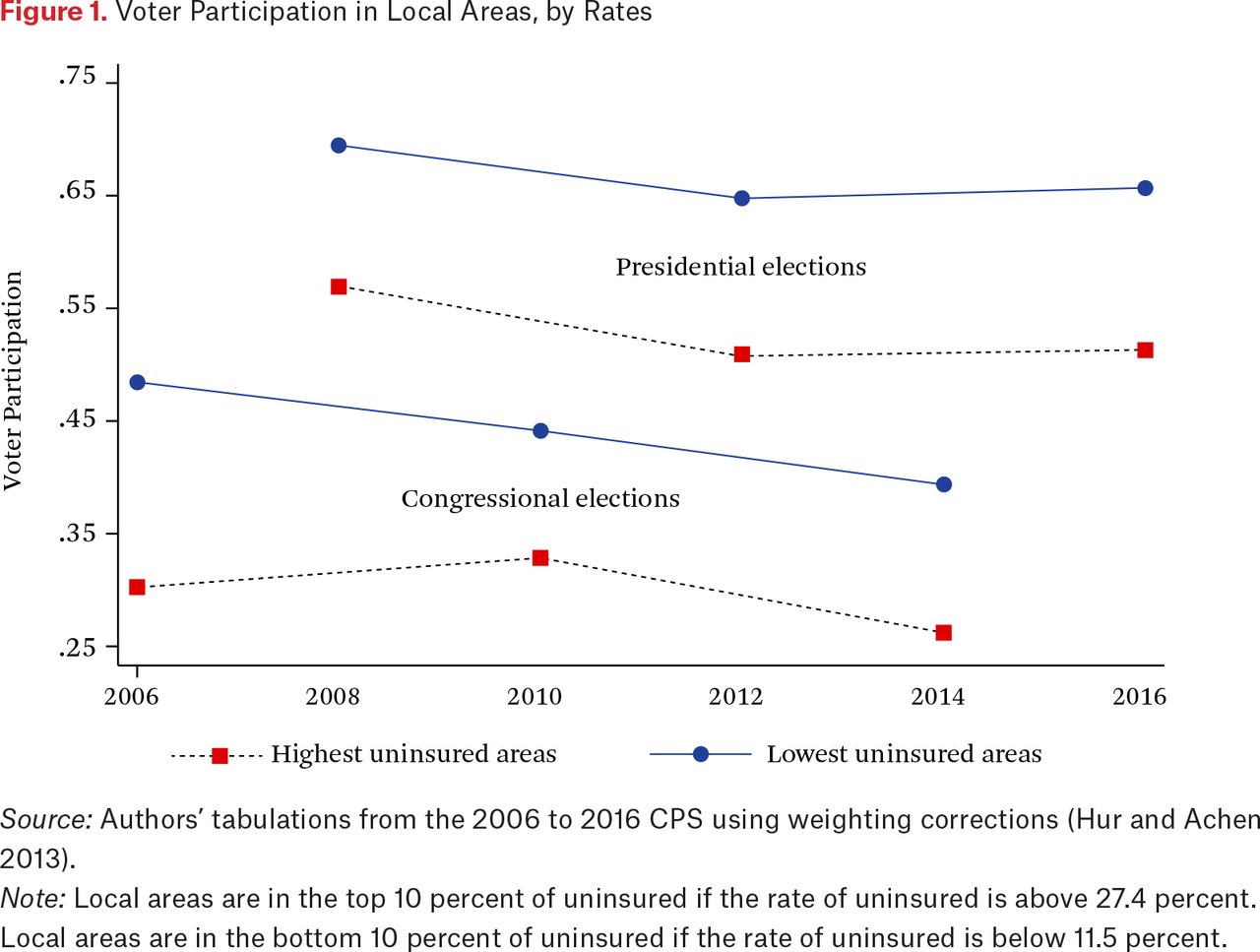
Voter Participation in Local Areas, by Rates
Source: Authors’ tabulations from the 2006 to 2016 CPS using weighting corrections (Hur and Achen 2013).
Note: Local areas are in the top 10 percent of uninsured if the rate of uninsured is above 27.4 percent. Local areas are in the bottom 10 percent of uninsured if the rate of uninsured is below 11.5 percent.
Table 2 shows health insurance coverage, derived from the SAHIE for 2011 through 2016. Overall, insurance coverage increased in 2014 on implementation of the full ACA provisions and continued to increase through 2016. Coverage gains were larger among younger, nonwhite, or less affluent adults. States that elected to expand Medicaid in 2014 (or early 2015) had higher baseline insurance levels, and exhibited larger overall gains in coverage after implementation. The impact of the ACA was most dramatic in states that expanded Medicaid and had a high baseline uninsured rate. The bottom part of table shows the growth in coverage for the newly eligible adults (near-poor adults, those living under 138 percent of the FPL) and all other adults in both expansion and non-expansion states. Without question, near-poor individuals in expansion states saw the greatest increase in coverage—14.9 percentage points on average, translating into insurance gains of nearly 2.4 million non-elderly adults. However, other groups—near-poor adults in non-expansion states, and higher-income adults in both expansion and non-expansion states—also experienced significant growth. Insurance gains for near-poor adults in non-expansion states were approximately 1.2 million (10.1 percentage points). Gains for higher-income adults from private coverage were approximately 7.2 million or 5.4 percentage points in expansion states, and 4.8 million or 4.3 percentage points in non-expansion states. Overall, the insurance gains for near-poor, non-elderly adults in Medicaid expansion states made up approximately 15 percent of all gains.
Health Insurance Coverage of Non-Elderly Adults, SAHIE (Various Years)
For our empirical work, starting from an initial 2006 through 2016 CPS sample of 914,152 respondents, we restrict attention to the 567,706 respondents in the vote-eligible population, that is, respondents age eighteen or older who are citizens of the United States. The sample is further restricted to the 490,053 respondents who provide yes or no answers to the voting question (Hur and Achen 2013). We remove a few respondents when we could not derive a local unemployment rate, as well as individuals who had missing values for family income, leaving a sample of 465,517 respondents. Finally, we exclude individuals older than sixty-four because the ACA was not intended to affect the health-care coverage of seniors (Courtemanche et al. 2017), leaving 371,015 respondents.
Table 3 shows selected summary statistics for the remaining CPS sample, as well as by year (full results in table A1).16 There are large swings in voter turnout across congressional and presidential elections, but more muted swings in registration. Approximately 60 percent of respondents lived in a state that expanded Medicaid. The local unemployment rate rises until 2010, and then decreases after. Approximately 56 percent of respondents self-report their voting and registration status; 44 percent had another respondent report voting and registration for them.
Selected Summary Statistics from the 2006 to 2016 CPS Voter Registration Supplement
EMPIRICAL FRAMEWORK
We estimate both DD models examining the impact of the Medicaid expansions alone and DDD models that isolate both the public and private portions of the ACA. The DD specification takes the form

where Vist is an indicator for whether individual i living in state s voted in election year t, MEDICAIDsindicates whether state s participated in the ACA’s Medicaid expansion, POSTt indicates whether time t is in the posttreatment period (2014 or later), Xist is the set of individual-level controls discussed, Pst is the set of state-level political variables, αs and τt are the state and election year fixed effects, and εist is the error term. Expansions states are those that adopted in 2014 or early 2015, and the posttreatment period does not count for the specific timing of the expansion (see Courtemanche et al. 2019a). We do not include the MEDICAIDs and POSTt dummies separately because they are subsumed by the state and year fixed effects. The coefficient of interest is β1, which represents the average effect of the Medicaid expansion on residents of expansion states. Standard errors are robust to heteroscedasticity and clustering by state.
The DDD model adds a third layer of variation: pre-ACA uninsured rates across counties. This approach is based on the idea that areas where a greater percentage of residents are uninsured experience larger treatments from large-scale health insurance expansions (see Courtemanche et al. 2017, 2018a, 2018b, 2019a, 2019b). The model is
where UNINSUREDc is the time-invariant pre-ACA uninsured rate in county c, θc and σt are county and year fixed effects, and µicst is the error term. In non-Medicaid expansion states, the effect of the ACA is given by γ2 * UNINSUREDc, We are especially interested in γ2 * UNINSUREDc, which is the effect at the mean county pretreatment uninsured rate in our sample. Similarly, the effect of the Medicaid expansion is γ3 * UNINSUREDc, and its effect at the average pretreatment uninsured rate is γ3 * UNINSUREDc. The impact of the “full ACA”—that is, both the Medicaid expansion and the so-called private portion of the law that was implemented in all states—is therefore the sum of these terms, which is (γ2 + γ3) * UNINSUREDc with (γ2 + γ3) * UNINSUREDc being the total effect at the mean pre-ACA uninsured rate.
The key identifying assumption behind the impact of the Medicaid expansion in our DD model is that, conditional on the other control variables, any changes in voter turnout would have been the same in Medicaid expansion and non-expansion states had the expansion not occurred. Our DDD model, on the other hand, has separate key identifying assumptions for the impact of the Medicaid expansion and for the impact of the private components of the ACA. The identifying assumption behind the impact of the Medicaid expansion in our DDD model is that, in the absence of the ACA, the differentials in voter turnout between high and low baseline uninsured rate areas in Medicaid expansion states would have evolved similarly to these differentials in non-expansion states. The identifying assumption behind the impact of the private (national) components of the ACA in our DDD model is that, in the absence of the ACA, any changes in our outcomes of interest would not have varied differentially by local area uninsured rates, conditional on the controls. The DDD approach also requires potentially restrictive functional form assumptions: the intensity of treatment is assumed to vary linearly with the pretreatment uninsured rate, and the ACA is assumed to have no causal impact in a (hypothetical) county with no uninsured people. Accordingly, we consider γ1—the effect of expanding Medicaid at a 0 percent uninsured rate—to represent unobserved state-level confounders rather than part of Medicaid’s causal effect.
In both the DD and DDD models, our identification strategy assumes that areas gaining more insurance coverage would potentially have more mobilization (and the conceptual model suggests that the mobilization would come mostly from those who gained coverage), but nothing in our identification strategy constrains that to be the case. For example, areas with higher uninsured rates are also likely to have a larger portion of the insured population at risk for losing coverage, and they too could be mobilized to vote. To the extent that individuals are mobilized by the ACA but not geographically concentrated (as could be the case for sicker individuals with preexisting conditions or young adults covered by the dependent coverage mandate), our approach will not capture such mobilization.
MAIN RESULTS
Table 4 presents the regression results for our DD model. Columns (1) and (2) report results for the years of congressional elections (2006, 2010, and 2014), while columns (3) and (4) report the results for the presidential election years (2008, 2012, and 2016). The reason for this stratification is that the enormous differences in voter turnout between presidential and midterm elections documented in table 3 raise the possibility that the causal effect of the ACA could differ in the two types of elections. Because we only have one posttreatment year for both types (2014 for congressional, 2016 for presidential), it will not be possible to distinguish between differential effects by election type and effects that dissipate over time. Columns (2) and (4) include time-varying political variables that control for voter identification laws, early voting laws, and automatic registration; columns (1) and (3) do not.
Voter Turnout (DD Specifications)
We report results both for the full sample of non-elderly adults and subsamples for race-ethnicity (non-Hispanic white versus other), age (eighteen through thirty-nine, forty through forty-nine, and fifty through sixty-four), and income (less than and more than $50,000). We use the SAHIE pretreatment uninsured rates that correspond to each subsample. This is why, for instance, we do not stratify further within the age eighteen through thirty-nine category, because that is the narrowest age range for which SAHIE insurance information is available. Table 4 presents only the coefficient estimate representing the impact of the ACA Medicaid expansion (for all other covariates, excluding geographic controls, see tables A2 and A3).
In the full sample regression results presented in the top panel of table 4, the coefficient estimate in column (1) indicates that the Medicaid expansion reduced voter turnout in congressional elections by 4.0 percentage points (p-value = 0.121) relative to a base of around 38 percent, though the p-value associated with this coefficient suggests that it is not statistically significant at conventional levels. When we include political controls in column (2), this estimate falls to a 3.5 percentage point reduction (p-value = 0.160) in voter turnout in congressional elections. For presidential elections, column (3) suggests that the Medicaid expansion led to a 1.1 percentage point increase (p-value = 0.179) in turnout from a base of around 60 percent. When we include political controls in column (4), this estimate falls to a 0.9 percentage point increase (p-value = 0.289). Thus none of our full sample DD estimates suggest a statistically significant impact of the Medicaid expansion on turnout in either congressional or presidential elections.
Turning to our subsample DD results, we for the most part observe modest and statistically insignificant effects with a few notable exceptions. The Medicaid expansion led to a statistically significant 4.3 to 4.4 percentage point reduction in voter turnout among nonwhites in congressional elections, but a statistically significant 3.5 to 3.8 percentage point increase in presidential elections. Although we see no statistically significant difference in the impact of the Medicaid expansion on turnout in presidential elections by age, we do observe a statistically significant 4.4 to 5.2 percentage point decrease in congressional elections for those age forty to forty-nine. We also observe a statistically significant 4.0 to 4.2 percentage point decrease in turnout among lower-income individuals in our sample in congressional elections, but no statistically significant difference by income in presidential elections.
Table 5 presents the regression results for our DDD model in a similar format to the DD results in table 4. One difference is that the rows in table 5 report the implied effects of the private portion of the ACA, the Medicaid expansion, and the full ACA (private + Medicaid) at the mean pretreatment uninsured rate. Table 5 presents only the coefficient estimates representing the impact of the different components of the ACA (for all other covariates, excluding geographic controls, see tables A4 and A5).
Voter Turnout, Implied Effects for DDD Specification
In congressional elections for the full sample, the DDD coefficient estimates on the Medicaid expansions suggest reductions of 3.1 and 3.6 percentage points in turnout, but the standard errors are large, so the estimates are not statistically significant (the p-values are 0.489 and 0.416 respectively). The estimated effect of the private portion of the ACA is similar in magnitude but positive rather than negative and also statistically insignificant. Together, the estimated impacts of the private and Medicaid expansions approximately cancel each other out so that the full effect of the ACA is approximately zero.
The full sample DDD results for presidential elections, shown in columns (3) and (4), are somewhat different but lead to the same general conclusion of little overall effect. The Medicaid expansion now increases voter turnout by 2.7 to 2.8 percentage points—relative to a base of around 60 percent—yet the coefficient is statistically insignificant. The estimated effect of the private portion of the ACA is negative, but smaller in magnitude: 1.9 to 2.3 percentage points, with the latter being statistically significant at the 10 percent level. Combining the impacts of the private and Medicaid expansions again yields full effects that are small and insignificant. Thus, as in congressional elections, the fully implemented ACA had no statistically significant impact on voter turnout in presidential elections.
Turning to our subsample DDD results, much in the DD models, the congressional election results are often modest and statistically insignificant, a few notable exceptions aside. One notable finding is that for nonwhites, the Medicaid expansion led to a statistically significant 8.8 to 9.2 percentage point reduction in voter turnout in congressional elections and the private portion of the ACA led to a statistically significant increase of 5.3 to 5.4 percentage points. Overall, the fully implemented ACA led to a 3.4 to 4.0 percentage point reduction in congressional turnout among nonwhites, the 4.0 percentage point estimate being statistically significant at the 10 percent level and the 3.4 percentage point estimate statistically insignificant (p-value = 0.145). In the higher-income subsample (more than $50,000), the private portion of the ACA increases congressional voter turnout by a sizable 5.1 to 5.8 percentage points, with the 5.8 percentage point effect without political controls being statistically significant at the 10 percent level and the 5.1 percentage point effect with political controls being statistically insignificant (p-value = 0.157).
Similarly, we see that most of the subsample results for presidential elections continue to reveal modest, insignificant effects with a couple exceptions. For nonwhites, the Medicaid expansion increases turnout by 4.7 to 6.4 percentage points, but the estimates are not statistically significant. A more puzzling result is that among the higher-income subsample, the Medicaid expansion leads to a large (5.2 to 5.3 percentage point) and statistically significant increase in turnout. Conceivably, this result could reflect a spillover effect, following which individuals whose coverage is not directly affected are nonetheless more motivated to vote by broader considerations. For instance, Jake Haselwerdt (2017) finds a backlash effect among conservative voters opposed to ACA implementation. Additionally, the ACA provided greater insurance protection to those who currently have coverage but may be at risk of losing it in the future.
MULTIPLE HYPOTHESIS TESTING
Tables 4 and 5 report evidence of scattered, and sometimes surprising, statistically significant effects across the various subsamples. However, given the large number of subsamples and specifications, some statistically significant estimates would be expected to emerge simply by chance. We therefore next ask whether any of these effects survive adjustments for multiple hypothesis testing. In other words, after accounting for multiple comparisons, can we reject the null hypothesis of no effects across any subsamples?
The simplest multiple hypothesis test adjustment is the Bonferroni correction, which simply divides the p-value necessary to obtain a given level of significance by the number of hypotheses being tested. In our case, given eight subsamples (including the full sample), we divide 0.1, 0.05, and 0.01 by eight to obtain new p-value thresholds of 0.0125, and 0.00625, and 0.00125. Such a procedure controls the overall type 1 error rate, making the probability of obtaining any spurious results from the eight subsamples 0.1, 0.05, and 0.01, respectively (Dunn 1961). Table 6 reports the p-values from the statistically significant subsample estimates from tables 4 and 5. We see that the smallest (most highly significant) p-value is 0.013, which does not meet any of the Bonferroni-adjusted p-value thresholds. In other words, we cannot conclude that any of the effects are “real” after using the Bonferroni correction.
Holm-Bonferroni-Adjusted Significance Levels for Statistically Significant Subsample Results
A criticism of the simple Bonferroni method is that it can be too conservative if the number of tests is high or the test statistics are positively correlated (Moran 2003). One alternative is the Holm-Bonferroni method, which controls the type 1 error rate in a way that retains greater statistical power. The lowest (most strongly significant) p-value is still subjected to same test as the Bonferroni method—thresholds divided by the number of tests. However, the next lowest p-value’s threshold is divided by the number of tests minus one, the next lowest the number of tests minus two, and so on (Holm 1979). In our case, this means the second-lowest p-value from a given group faces thresholds of 0.1, 0.05, and 0.01 divided by seven, or 0.014, 0.00714, and 0.00143. The third-lowest p-value uses thresholds divided by six, or 0.01666, 0.0083, and 0.00167. Table 6 shows the p-value thresholds for each specific statistically significant estimate, defining groups as the eight subsample estimates for a particular treatment (Medicaid or private), election type (congressional versus presidential), and specification (for example, DD without political controls). We see that using the Holm-Bonferroni method instead of Bonferroni does not help any effects to survive. We still conclude that no evidence indicates that any subsamples are affected.
Note that, if anything, this analysis errs on the side of being too generous. It could be argued to define the groups more broadly, in which case the adjustments would use even lower p-value thresholds that divide by an even larger number of hypothesis tests. In the most extreme case, all estimates could be grouped together, in which case the p-value thresholds would be divided by sixty-four rather than eight. In any case, the analysis from table 6 is enough to make the case that not too much should be made of the occasional stars from tables 4 and 5. On balance, evidence is minimal that the ACA meaningfully influenced voter turnout, either for the full sample or for demographic subsamples.
ROBUSTNESS CHECKS
We next conduct a number of robustness checks to address potential concerns with our baseline specifications. The main finding is that the general pattern of no statistically significant effect on voter turnout or registration is robust to a variety of specification checks and consideration of additional relevant policies.
In our baseline DDD model in equation (2), we do not include a full set of state-year effects; rather we include MEDICAIDs * POSTt to control for time-varying differences across expansion and non-expansion states. As a consequence, the DDD model does not capture time-varying, unobserved state-level confounders, but instead time-varying confounders common to all states. To the extent of heterogeneity in voting trends within the group of expansion or non-expansion states, the MEDICAIDs * POSTt interaction will not control for it. As a specification check, we explore the sensitivity of the results to including a full set of state-year interactions (table A6). By including state-year fixed effects, our identification comes from within-state variation in uninsured rates at the local level. Our primary conclusion—that the fully implemented ACA has virtually no effect on mobilization in the full sample—persists, although in some cases the standard errors increase dramatically. In no instance is the full effect of the ACA statistically significant for any subgroup. In some instances, effects of the private portion of the law and the Medicaid expansions are statistically significant and offsetting, but these results are, as discussed earlier, susceptible to the multiple hypothesis test critique.
Our voter turnout models in tables 4 and 5 have stratified the sample by congressional and presidential elections, and especially for the full sample, have found little impact in terms of mobilization. We have estimated models that pool all election years, since such an approach would allow more precise estimation of the treatment effects of the ACA. Even with the larger sample (and two “post” years), we find very little effect of the Medicaid expansion or full ACA across our models (table A7). The Medicaid expansions insignificantly reduce turnout (by up to 1.7 percentage points) for the full sample. The full effect of the ACA in the DDD models is not statistically significant for any demographic group (the largest point estimate of the full effect of the ACA is a 1.9 percentage point increase for white voters).
We also have estimated voter registration models (tables A8 through A13). Broadly, the results continue to suggest small and statistically insignificant effects in most cases. Given the findings from our previous analysis of multiple hypothesis testing, we are reluctant to attach much importance to the handful of statistically significant results in some of the subsamples. A noteworthy result—across both the voter turnout and registration models—is that including the state-level political controls makes virtually no difference in the estimated effects of the ACA. In the few cases when including political controls affects statistical significance, they do because both estimates are near a particular threshold. These findings suggest that adoption of voting laws was essentially uncorrelated with Medicaid expansion decisions and uninsured rates.
We next examine several additional institutional details that may affect the relationship between the ACA and voter outcomes. These include the ACA’s interaction with motor voter legislation, the impact of turmoil from technology glitches during the first open enrollment period, and the impact of changing the parameterization on the percent uninsured variable in our DDD analysis.
One important discussion point is how the 1993 motor voter legislation (National Voter Registration Act or NVRA) might interact with the ACA rollout (in turn potentially increasing voter participation and especially registration). The NVRA legislation mandates public assistance agencies to provide voter registration services to every person applying for or renewing government benefits, including Medicaid (Michener 2016). Some groups take a more expansive view of what government benefits means (above and beyond the Medicaid expansions and state-run exchanges), and argue that the NVRA applied to both federal and state-run exchanges, even though many states on the federal exchange did not expand Medicaid (Rho and Barksdale 2013). The Obama administration, in contrast, acknowledged that NVRA applied to state-run exchanges but did not include voter registration service in the ACA federal exchanges (Onek 2015).
Given widespread agreement that NVRA applied to public Medicaid coverage on state-run exchanges, we focus on fourteen state-run exchanges only. It is far less clear, especially given that the Obama administration ignored the NVRA on federal exchanges, whether any predictions for expanding private coverage are especially useful. All states that ran their own exchange in 2014 also expanded Medicaid that year. Of the state-run exchanges, six states acknowledged their obligation to provide voter registration services under NVRA, and eight states had no announced plans to comply with NVRA (Rho and Barksdale 2013). We therefore classify states as NVRA-compliant and estimate DD models for congressional or presidential elections, substituting this variable for the Medicaid expansions. Similar to our original DD model, the model now becomes

where the coefficient estimate θ1 represents the DD estimate of NVRA compliance on the outcomes of interest. Our prediction is that, if the motor voter act were enforced during the Medicaid expansion, states that affirmatively signed on to NVRA would have higher registration rates and perhaps voter turnout.
We estimate models for voter turnout and registration, in congressional and presidential elections, for these states (table A14). The findings suggest the ACA’s interaction with the motor voter act did not increase registration or turnout. In all instances, the DD estimate is negative for voter registration, the most directly affected outcome. In most cases, the effect on turnout is also negative. We might expect that young adults, given their low registration and high mobility, to be particularly sensitive to the motor voter act, yet in NVRA-complaint expansion states, registration is falling, not rising. Thus we find no evidence that the motor voter act increased political participation after ACA implementation.
In earlier work (Courtemanche et al. 2017), we examined the impact of exchanges that experienced glitches. Amanda Kowalski (2014) notes that six state-run exchanges had severe technology glitches and that “the federal exchange had its own difficulties.” All six also had a Medicaid expansion. Such glitches were prominent during the open enrollment period for the initial ACA rollout in 2014, but were corrected in subsequent open enrollments.
We focus on state-run exchanges, and examine whether turmoil through technology glitches affected voter outcomes. We focus on the fifteen jurisdictions Kowalski (2014) classifies as state exchanges, six of which had glitches. Because all of these states also had Medicaid expansions, we modify our DD framework by replacing Medicaid expansion with exchange glitch:

where the coefficient estimate ϑ represents the DD estimate of exchange glitches on the outcomes of interest. Our prediction is that, if a state experienced technology glitches, enthusiasm about the ACA would be diminished, thereby affecting voter turnout or registration. Such glitches were corrected by open enrollment window for 2015; therefore, we only examine the impact of glitches for congressional elections, which includes 2014.
We estimate models for voter turnout and registration in congressional elections for these fifteen jurisdictions (table A15). The findings suggest that exchanges glitches did not increase registration or turnout. In all but one case, the DD estimate is insignificant and relatively small. For the full sample, voter turnout—an expression of frustration with glitches—insignificantly increased by 0.5 percentage points in the 2014 election (standard error of 1.8 percentage points). Voter turnout does not increase for any group due to glitches, and only one group experienced a registration increase (although the same critiques about multiple hypothesis testing apply here).
Finally, we modify our primary DDD specification by examining different parameterizations of the local, pretreatment uninsured rate. First, we compute the DDD estimates using the uninsured rate from 2010 rather than 2013 (table A16). When the ACA was enacted in 2010, the earliest provisions to reduce the uninsured were implemented soon after (such as the dependent coverage mandate); thus, the uninsured rate in 2013 may not accurately measure the pre-period. Second, we compute the 2013 pretreatment uninsured rate for individuals under 250 percent of the FPL (table A17). For both parameterizations, the DDD findings are remarkably stable to the main findings.
DISCUSSION
In this study, we explored the broader ramifications of the ACA by examining the impact on political participation. Using large samples of respondents from the publicly available CPS Voter and Registration Supplements from 2006 to 2016 and a DDD methodology to estimate the impact of both the private and public portion of the law, we find little impact on mobilizing newly eligible insured individuals to vote or register. Our study thus contributes to the literature by disentangling the causal impact of the different components of the ACA on our outcomes of interest, rather than focusing on a single component in isolation.
More generally, this article contributes to an emerging empirical examination on how the ACA, or Medicaid in particular, affects public opinion and policy, polarization, and other non-health outcomes. Richard Fording and Dana Patton (2020) examine the policy backlash (in the form of work requirements) from the ACA’s Medicaid expansions, which is difficult to reconcile with the notion that Medicaid produced positive policy feedback, supportive constituencies, and policy entrenchment. They argue that the full range of policy feedback effects can mixed or negative, which can lead to self-undermining consequences such as policy regression. Their hypotheses are empirically supported in an original dataset on gubernatorial support for Medicaid work requirements. Julianna Pacheco, Jacob Haselwerdt, and Jamila Michener (2020) examine how polarization in ACA support varies by both policy choices and party in power. They find that attitudes are especially polarized in states with aligned partisan environments where Democratic governors support setting up state health exchanges. Carrie Fry, Thomas McGuire, and Richard Frank (2020) isolate the impact of Medicaid on criminal recidivism, and find the expansion has a small negative relationship with recidivism.
Our findings stand in contrast to some other recent work on the ACA (Haselswerdt 2017; Clinton and Sances 2018). Overall, our analysis does not find significant voter mobilization in response to the ACA during the 2014 and 2016 elections. It is interesting to contrast our empirical findings based on the 2014 and 2016 elections with the conventional wisdom that the 2018 congressional election was a referendum on the ACA that generated increased voter turnout. Several points about such a comparison are significant. First, some of our political variables (such as automatic registration) were only starting to be implemented toward the end of our 2006 to 2016 period and very well could have enhanced turnout in the 2018 election (and beyond). Second, Gallup polls suggest that voters always rank health-care policy as a top priority. According to these polls, in 2012, 2014, 2016, and 2018 the share of voters ranking health care as “extremely / very important” was 80 percent, 64 percent, 77 percent, and 80 percent respectively (Newport 2012, 2014, 2018; Jones 2015). Third, even though health care is consistently ranked as a high priority, it may have been more salient in 2018. In 2014, when President Barack Obama was in office, it was clear that ACA repeal efforts would not survive a veto. In 2016, the election of President Donald J. Trump was a shock, and voters would not have anticipated serious repeal efforts under a Clinton presidency. In contrast, by 2018, President Trump had the opportunity to work with a Republican House and Senate, and almost succeeded in a skinny repeal in July 2017. In addition, three fairly conservative states had Medicaid expansions on the ballot in 2018. As a consequence, both the gains and losses from the ACA were far more salient, which might suggest a heterogeneous treatment effect.
Nonetheless, it is not clear that the skinny repeal or state-level Medicaid expansions (or Medicaid work requirements) mobilized voters, versus the 2018 turnout (and outcome) being a more general referendum on Trump’s presidency. Issues such as polarization, immigration, gun violence, and sexual harassment on the one hand, and the booming economy and Supreme Court appointments on the other, are likely to have affected turnout as well. Thus, even with the heightened salience in 2018, we would be reluctant to ascribe the turnout as primarily an ACA mobilization effect. This suggests the need for more research incorporating 2018 data from the CPS and other data sources. One limitation of the CPS is that its measures of political participation do not allow us to examine attitudes or ideology, and thus we are not able to observe whether changes in turnout across various subgroups was concentrated among Democrats or Republicans (which would suggest a backlash to repeal efforts).
FOOTNOTES
↵1. Wesleyan Media Project, “2018: The Health Care Election,” October 18, 2018, http://mediaproject.wesleyan.edu/releases/101818-tv (accessed January 9, 2020).
↵2. This approach mimics the earlier work of Amy Finkelstein (2007), who studied the initial introduction of Medicare, and Sarah Miller (2012), who studied Massachusetts’s health reform.
↵3. Michener (2017) examines voter turnout (and other forms of civic participation) for almost all counties in the United States in the 2000, 2004, and 2008 presidential elections, where the key independent variable is percentage of children enrolled in Medicaid. The estimate is unlikely to be causal because it is not based on quasi-experimental policy variation.
↵4. However, Jacqueline Chattopadhyay (2017) finds that young adults show virtually no signs of political feedbacks from the dependent coverage provision.
↵5. HealthCare.gov, “Pre-existing Condition Insurance Plan (PCIP), https://www.healthcare.gov/glossary/pre-existing-condition-insurance-plan-pcip (accessed January 9, 2020).
↵6. National Federation of Independent Business v. Sebelius, 567 U.S. 519 (2012).
↵7. Here efficacy represents the extent to which an individual believes the government listens to people like them.
↵8. They also find that citizenship has a substantial effect on turnout; in our empirics, we focus on the vote-eligible population (citizens, age eighteen and older).
↵9. Of those enrolled in Marketplace coverage in 2018, fully 87 percent received a premium tax credit and 53 percent received cost-sharing reductions (for more, see Kaiser Family Foundation 2019a).
↵10. The question of whether Medicaid sends a stigmatizing message is debatable. Recent surveys have found that 74 percent of the public, including a majority of Democrats (84 percent), Independents (76 percent), and Republicans (61 percent) look favorably on Medicaid (Zirzinger, Wu, and Brodie 2017).
↵11. Individuals are vote eligible if they report themselves as citizens and age eighteen or older. In practice, we restrict our sample in several other ways, most importantly by confining our analysis to non-elderly adults.
↵12. United States Elections Project, “CPS Vote Over-Report and Non-Response Bias Correction,” 1994–2016, http://www.electproject.org/home/voter-turnout/cps-methodology (accessed January 9, 2020). Other examples of reweighting to account for underreporting include Bradley Hardy, Timothy Smeeding, and James Ziliak (2018), who examine SNAP participation, and Robert Hartley, Carlos Lamarche, and Ziliak (2017), who examine AFDC/TANF participation.
↵13. These covariates, including family income, are commonly in individual-level analyses of voter turnout with the CPS VRS (see, for example, Holbein and Hillygus 2016). We have rerun our specifications excluding family income and employment status, and none of the conclusions change.
↵14. The difference is usually computed from the vote percentages for the Democrat and Republican candidates. When no relevant race took place within a given state-year cell, we code the difference as 0, and also include a dummy variable for that race occurred.
↵15. The threshold for being in the lowest 10 percent of uninsured rates for an area was 11.4 percent. The threshold for the highest 10 percent was 27.5 percent.
↵16. All supplemental appendix tables, designated in text with a leading A, are available via the online appendix at https://www.rsfjournal.org/content/6/2/179/tab-supplemental.
- © 2020 Russell Sage Foundation. Courtemanche, Charles, James Marton, and Aaron Yelowitz. 2020. “The Full Impact of the Affordable Care Act on Political Participation.” RSF: The Russell Sage Foundation Journal of the Social Sciences 6(2): 179–204. DOI: 10.7758/RSF.2020.6.2.08. We thank Emily Dunlap for expert research assistance. We also thank the editors, Andrea Campbell and Lara Shore-Sheppard, three anonymous referees, and participants at University of Kentucky’s brownbag economics lunch and the Russell Sage Foundation Social, Political, and Economic Effects of the Affordable Care Act conference for helpful comments. Direct correspondence to: Charles Courtemanche at courtemanche{at}uky.edu, Department of Economics, 244 Gatton Business & Economics Building, University of Kentucky, Lexington, KY 40506; James Marton at marton{at}gsu.edu, Department of Economics, Andrew Young School of Policy Studies, Georgia State University, P.O. Box 3992, Atlanta, GA 30302; and Aaron Yelowitz at aaron{at}uky.edu, Department of Economics, 225H Gatton Business & Economics Building, University of Kentucky, Lexington, KY 40506.
Open Access Policy: RSF: The Russell Sage Foundation Journal of the Social Sciences is an open access journal. This article is published under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.
REFERENCES
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.