
Abstract
This study examines how individuals assess administrative burdens and how these views change over time within the context of the Special Supplemental Nutrition Assistance Program for Women, Infants, and Children (WIC), which provides food to pregnant and breastfeeding women and children under age five. Using interview data from the Baby’s First Years: Mothers’ Voices study (n = 80), we demonstrate how the circumstances of family life, shifting food needs and preferences, and the receipt of other resources shape how mothers perceive the costs and benefits of program participation. We find that mothers’ perceptions of WIC’s costs and benefits vary over time and contribute to program participation trajectories, so many eligible people do not participate; need alone does not drive participation decisions.
The COVID-19 pandemic brought about a once-in-a-century public health crisis and economic precarity not seen since the Great Depression. Unemployment rose from a low of 3.6 percent in December 2019 to a high of 14.4 percent in April 2020 (BLS 2020a, 2020b). Record job loss led to acute economic hardship and food insecurity (Niles et al. 2020; Steimle et al. 2021; Wolfson and Leung 2020). The pandemic also revealed the importance of safety-net programs in supporting vulnerable populations, raising questions about how well families can access critical assistance. Although scholars emphasize the role of these programs in reducing poverty and food insecurity among vulnerable households (Bitler, Hoynes, and Iselin 2020; Bitler, Hoynes, and Schanzenbach 2020), early accounts of the pandemic highlight the difficulties of accessing programs such as unemployment insurance and nutrition assistance (Ganong et al. 2022; Gassman-Pines, Ananat, and Fitz-Henley 2020). As the editors outline in the introduction of this issue, the challenges of accessing public benefits—administrative burdens—can undermine policy goals, reinforce patterns of inequality, and weaken the polity (Herd et al. 2023, this issue). Research highlights the dimensions and consequences of administrative burden, but scholars pay less attention to how individuals assess burdens or how they perceive a change in burdens over time.
Studies that do examine responses to burdens focus on how individual-level characteristics like cognitive capacity can shape program uptake (Christensen et al. 2020). This research seldom contextualizes policy targets by providing deep insights into the social and economic factors that might shape how they view burdens and their choice to persist in burdensome welfare claims. Studies that do offer such insights examine how well-resourced individuals successfully claim benefits (Masood and Nisar 2021). We know less about how these social and economic factors inform how low-income individuals perceive the costs of program participation or the value of benefits. How do program beneficiaries weigh the costs and benefits of program participation? How do these views shape patterns of program uptake over time?
We address these questions within the context of the Special Supplemental Nutrition Assistance Program for Women, Infants, and Children (WIC), which provides vouchers to purchase basic food items (such as cereal, milk, and vegetables) to pregnant and breastfeeding people and children under age five. Drawing from eighty in-depth qualitative interviews, we examine initial and continued WIC program use in light of participants’ family contexts, social supports, and other forms of economic assistance. We demonstrate how program participants perceive the value of WIC benefits and the costs of applying for and maintaining benefits during the COVID-19 pandemic. Our interviews also show the challenges of redeeming benefits using the new, electronically distributed eWIC.
In doing so, we examine whether WIC is realizing its potential in addressing inequality in giving children access to a healthy start in life. If, for instance, a burdensome program design creates costs that underresourced or minoritized families are less likely to be able to bear, it is limited in achieving its programmatic mission. Further, this study sheds light on factors that shape individuals’ perceptions of administrative burden and how those burdens are weighed against potential benefits to determine program participation over time. These factors include eWIC and pandemic-induced changes to the program. Finally, these data are collected from mothers participating in a randomized controlled trial of an unconditional cash transfer—Baby’s First Years provides $333 or $20 monthly to mothers over the first several years of their babies’ lives. Therefore, we can observe whether and how receiving the larger versus smaller cash gift each month positions mothers to view and respond to WIC administrative burdens differently. This offers insight into how financial resources might shape perceptions of administrative burdens.
LITERATURE REVIEW
Administrative burden reflects an individual’s “onerous experiences with policy implementation” (Burden et al. 2012, 742) that occur within service-seeking bureaucratic encounters and outside conventional bureaucracies (Barnes 2021; Burden et al. 2012; Heinrich 2016; Kahn, Katz, and Gutek 1976). Scholars conceptualize administrative burden as learning, psychological, and compliance costs (Moynihan, Herd, and Harvey 2015). Applicants encounter learning costs when they are unaware of what benefit programs exist, how to apply, and how to use benefits (Barnes 2021; Moynihan, Herd, and Harvey 2015). Psychological costs, or the stigma and stress of application processes, may also discourage uptake (Baekgaard et al. 2021). Compliance costs––burdens of following program rules, providing documents for application and recertification processes, and responding to bureaucrats’ discretionary demands—can deter program participation (Moynihan, Herd, and Harvey 2015). Finally, beneficiaries may experience costs outside conventional service-seeking encounters, such as when they attempt to redeem their benefits (Barnes 2021). Redemption costs emerge in consumer choice models of service delivery where beneficiaries must understand which goods or services are eligible and find a third-party agent who will redeem the benefit. Redemption costs occur in programs such as Medicaid (which requires beneficiaries to find health-care providers), childcare subsidy programs, the Housing Choice Voucher Program, and WIC (Barnes 2021).
Economists have long considered how those eligible for assistance programs weigh the burdens of participation against the benefits of programs and conclude that nonparticipation may reflect a “utility maximizing decision” (Moffitt 1983, 1023). This is especially the case when the stigma of participating in programs outweigh the value of benefits (Moffitt 1983). In a similar vein, economists frame burdens as ordeal mechanisms—or policy tools that screen out beneficiaries who are undeserving (Heinrich et al. 2021; Schuck and Zeckhauser 2006). From this perspective, applicants rationally respond to burdens by weighing the costs and benefits of program participation. Applicants who persist signal their true preferences and need for assistance. For these deserving applicants, the costs of claiming benefits are low.
In theory, ordeal mechanisms would ensure that assistance programs target those in need, sorting out “imposters” (Nichols and Zeckhauser 1982). Administrative burden scholars, though, critique the narrow view of ordeal mechanisms as overstating the capacity of individuals to pay the costs of laying claims on the state (Christensen et al. 2020; Heinrich et al. 2021; Masood and Nisar 2021). Accordingly, eligible policy targets do not necessarily calculate the costs and benefits of navigating burdens but may lack the capacity to understand and deal with costly bureaucratic encounters. Simply stated, burdens do not sort out imposters but do disproportionately harm vulnerable and marginalized populations (Bell et al. 2021; Brodkin and Majmundar 2010; Heinrich et al. 2021; Nisar 2018). Empirical studies demonstrate how ordeal mechanisms can lead to bureaucratic disentitlement or administrative exclusion wherein individuals who are eligible for programs are deterred from claiming benefits not because they are undeserving or prefer not to receive them but because the costs of doing so are too difficult to surmount (Brodkin and Majmundar 2010; Heinrich et al. 2021).
To help explain these patterns of exclusion, more recent research reframes individuals as active agents in claiming benefits (Masood and Nisar 2021). Policy targets’ capacity to successfully claim benefits can depend on their cognitive capacity, administrative capital, or administrative literacy (Christensen et al. 2020; Döring 2021; Masood and Nisar 2021). Julian Christensen and colleagues (2020) point to the role of cognitive resources like executive functioning—or the capacity to plan and engage in goal-directed behavior—in bearing administrative burdens. Scarcity, poor mental and physical health, and age-related cognitive decline can erode executive function in ways that undermine individuals’ capacity to claim benefits (Christensen et al. 2020). To reduce administrative burden, individuals may strategically leverage social, cultural, and economic capital (Masood and Nisar 2021). Further, people may rely on social networks or organizations for information and strategies to deal with administrative burdens (Heinrich 2016; Nisar 2018).
This work emphasizes individual-level factors that contribute to the capacity to successfully claim benefits and organizations that facilitate individuals’ capabilities; this overlooks individuals’ processes of choosing whether to claim and maintain benefits and the social and economic circumstances that shape these decisions. Further, this research does not probe how potential participants view the value and burdens of programs over time or how these perspectives shape eligible individuals’ claiming behavior (Moffitt 1983).
For example, a mother who is eligible for the Supplemental Nutrition Assistance Program (SNAP) may forgo claiming benefits because of the instrumental support she receives from friends and family or the economic resources of other targeted programs such as the Earned Income Tax Credit. These resources may ease the necessity of her relying on SNAP and therefore alter her willingness to deal with the burdens of applying for benefits. In the case of WIC—in which the value of benefits declines over time as children age—mothers may perceive the value as outweighing the costs at one point in time but later as exceeding the value and therefore exit the program. In this sense, it is not simply the burdens themselves that decrease claiming. How individuals perceive the intersection between the costs and benefits of program participation—views that may be shaped by an individual’s social and economic circumstances—can determine whether they claim benefits (Moffitt 1983). Low-income families are situated within social contexts that may inform their decisions to bear the burdens of welfare claiming (Domínguez and Watkins 2003; Henly, Danziger, and Offer 2005), and they often rely on multiple means-tested programs (Yang et al. 2019) that may shape how they perceive the value of benefits. To better understand how individuals decide to bear the burdens of claiming and maintaining benefits, we draw from in-depth qualitative interviews about how social and economic circumstances shape WIC benefit claims and program use over time.
CONTEXT
WIC is the third-largest food assistance program in the United States, serving 6.2 million families in 2020, a figure that includes nearly half of all infants (Toossi, Jones, and Hodges 2021). The program was established amid growing concerns about poverty-driven child malnutrition in the late 1960s, and the Department of Agriculture piloted small food distribution programs through select neighborhood clinics (Oliveira et al. 2002). This was formally authorized as a demonstration project in 1972. The WIC program then expanded to forty-five states and became permanent in 1974.
WIC offers a food package and nutritional education for individuals who have certain nutritional risks and meet income eligibility (Gray et al. 2019; Kline et al. 2020). Those who are pregnant, have given birth up to six months postpartum but are not breastfeeding, or are breastfeeding up to a year postpartum are eligible. Children are eligible from infancy to their fifth birthday. Individuals are eligible if their household income falls below 185 percent of the federal poverty line or they receive Temporary Assistance to Needy Families (TANF), Medicaid, or SNAP (Kline et al. 2020). Unlike other means-tested programs, WIC does not condition eligibility on immigrant status.1
After the initial certification, participants are eligible for a year. To maintain benefits, participants must attend quarterly appointments that assess nutritional risk, provide nutritional education, and issue benefits. WIC participants are prescribed a food package tailored to meet their household’s nutritional needs and a shopping guide that indicates WIC-participating retailers (Tiehen and Frazão 2016). Food packages specify eligible foods by brand and size. WIC participants purchase food using an electronic benefit transfer (EBT) card.
WIC enrollment and coverage rates—the percentage of the eligible population that participates in the program—have declined significantly since 2011 (Toossi, Jones, and Hodges 2021). Further, despite COVID policy waivers that made the program more accessible to beneficiaries, WIC participation in 2020 decreased by 2 percent from 6.4 million in 2019 to 6.2 million (Hall and Neuberger 2021). In addition, studies show that WIC program participation varies by the child’s age; most child participants enter the program within the first three months of life and exit after their first birthday (Gundersen 2005). Newer research suggests that mothers maintain longer-term connections with the WIC program over time through intermittent use across multiple pregnancies (Barnes, Michener, and Rains 2023). Nevertheless, some research attributes decline in program usage after infancy to changes in the food package, which eliminates formula from benefit packages after the baby turns one (Jacknowitz and Tiehen 2009), meaning that the cash value of WIC benefits can decline by nearly $130 at this point (Schanzenbach and Thorn 2020).
Other scholars point to required quarterly WIC appointments, two of which are in-person (Woelfel et al. 2004), and challenging shopping experiences (Barnes 2021) as reasons for declining enrollment. High compliance costs in the form of in-person appointments preclude long-term WIC participation. Transportation challenges and difficulties arranging appointments to accommodate work schedules can lead to program exits (Liu and Liu 2016; Panzera et al. 2017; Rosenberg, Alperen, and Chiasson 2003; Woelfel et al. 2004).
Learning how to redeem WIC benefits can also discourage participation over time. As one qualitative study of North Carolina WIC participants shows, participants struggle to identify and purchase WIC-eligible foods due to the limited portability of WIC benefits (Barnes 2021). For example, WIC participants say it is difficult to identify the WIC-approved foods—such as bread, milk, cheese, cereal, and baby food—that match their prescribed food package. Retailers add to this challenge by failing to keep WIC-approved items in stock or mislabeling foods as WIC-approved that are not. In addition, participants must learn which retailers accept WIC, stock and label WIC-eligible foods, and comply with redemption guidelines. The narrow selection of WIC-approved foods, which limits portability, and the reliance on third-party agents to redeem benefits can create redemption costs for recipients.
To modernize the program, WIC has transitioned to eWIC. The Child Nutrition and WIC Reauthorization Act of 2010 required WIC state agencies to implement EBT systems in lieu of paper vouchers by October 1, 2020. To participate in WIC, vendors must attend an annual training and are subject to audit by local WIC staff. Vendors must also keep WIC-approved foods in stock, train cashiers to process WIC purchases, and update their systems to reflect any state changes in WIC-approved foods.2
In theory, eWIC would minimize stigma, offer greater flexibility for participants, and reduce transaction times (Barnes and Riel 2022). However, research offers mixed evidence on the benefits of transitioning to an electronic benefit transfer system. On the one hand, research suggests that eWIC has improved the shopping experience (Hanks et al. 2019; Isaacs, Shriver, and Paynter 2021; Vasan et al. 2021). Yet some qualitative research points to persistent challenges WIC participants face when trying to correctly identify and purchase WIC-approved food, even with eWIC (Li et al. 2021; McElrone, Zimmer, and Anderson Steeves 2021).
BABY’S FIRST YEARS
A key contextual consideration framing our study is that we draw our data from the Baby’s First Years (BFY) intervention. BFY is the first randomized controlled trial of the effects of unconditional cash gifts on child development in the United States. Mothers participating in the study agreed to be randomly assigned to receive a large ($333) or small ($20) monthly cash gift for the first six years of their focal child’s life, distributed on a debit card; the gift is not conditional on mothers engaging in any type of behavior, including study participation, nor are they constrained in how they may spend it. The research team worked closely with state and local agencies to ensure, to the extent possible, that the cash gift does not count against eligibility for government benefits. Given the intervention context of this study, we are able to observe whether mothers in the large- versus small-cash-gift groups display distinct WIC use patterns or describe particular trends in the administrative burdens they see connected to engaging with the WIC program. It is possible that this additional monthly cash income could make mothers in the large-gift group feel less of a need for WIC or, alternatively, they could use these additional resources to help them overcome barriers to program access (for example, transportation to WIC appointments). We explore these possibilities.
CURRENT STUDY
This study draws on the administrative burden research and empirical evidence about WIC program and retail experiences to explore how participants perceive the value and costs of program participation and how these views shape decisions to continue program receipt. Drawing from interviews with eighty low-income mothers, we observe families as they experience challenges with accessing, maintaining, and using the WIC program amid the transition to eWIC and the onset of a global pandemic. In addition, we observe how a randomly assigned large versus small monthly cash gift might alter mothers’ interactions with and views of WIC. We explore how these factors shape mothers’ perceptions of program burdens and benefits. In doing so, we address our research questions of whether and how mothers experience administrative burdens with the WIC program, how they consider both the benefits and costs of program use in deciding to access WIC services, and how these perceptions unfold over time.
METHODS
In BFY, one thousand mothers were recruited from across four metro areas—New Orleans, Omaha, New York City, and the Twin Cities—when they gave birth to the focal child, starting in 2018.3 All were over the age of eighteen and living below the federal poverty line, most were women of color, just under half of the mothers were in coresidential partnerships, and approximately one-quarter were first-time mothers. On average, they reported household incomes of about $20,000. The cities were chosen to capture variation in demographics, cost of living, and policy environment (for more details on study design, see Noble et al. 2021).
Baby’s First Years: Mother’s Voices (BFY: MV) is the qualitative component of the study, in which eighty of the mothers from BFY participated. Using stratified random sampling, we recruited fifty mothers from New Orleans and thirty from the Twin Cities, which aligns with the site distribution of mothers in the larger study. Within each city, we sampled an equal number of mothers receiving each gift amount for a total of forty each in the large- and small-gift groups.
Table 1 provides the demographic characteristics of the BFY: MV mothers at wave 1. Black mothers make up 66 percent of the sample, White mothers 10 percent, Hispanic mothers 9 percent, Asian mothers 4 percent, Native American mothers 1 percent, and the remaining mothers identify with multiple races or another race. BFY: MV mothers had between one and six children with a median of two; for 29 percent of mothers, the focal child was their first. At wave 1, the median age of mothers was twenty-seven and the focal child thirteen months. At the time of the first interview, 79 percent of the focal children had turned one year old, meaning that most were no longer eligible to receive formula through WIC. Only three mothers had another infant—younger than the focal child—at wave 1. At the time of the wave 1 interview, 64 percent of BFY: MV mothers were using WIC, 71 percent received SNAP, and 9 percent were enrolled in TANF.
Demographic Characteristics of BFY, MV Mothers at Wave 1 (N = 80)
Nationally, about two-thirds of WIC participants are at or below the federal poverty line, the cutoff used for recruitment into BFY, and about 20 percent identify as Black (Kline et al. 2020). Although the overall participation rate for all those eligible for WIC is 57 percent, among infants under one it is 98 percent, and among one-year-olds it is 61 percent (USDA 2021). The BFY: MV families, therefore, differ from the national WIC population in being more economically disadvantaged and more likely to be Black. We view the demographic makeup as a strength. Our analysis offers useful insights on most vulnerable families who have been disproportionately harmed by the COVID-19 pandemic.
DATA
For the present study, we used the first two waves of semi-structured interviews from BFY: MV. For wave 1, interviews typically lasted about one and a half hours. Most (68 percent) occurred in person between July 2019 and March 2020 and were usually completed in mothers’ homes. During the COVID-19 pandemic, we transitioned to conducting interviews by phone for the remaining wave 1 interviews completed by September 2020. All wave 2 interviews occurred by phone between July 2020 and August 2021 and typically lasted a little over an hour. For each mother, waves 1 and 2 interviews occurred nine to twelve months apart. The interviews covered an array of topics, including mothers’ childhood and educational experiences, parenthood and family life, sources of income and types of expenses, decisions about finances as well as financial services, experiences with income support programs (including WIC), mothers’ experiences of Baby’s First Years, and mothers’ vision for their futures and their children’s. Because mothers were recruited into BFY: MV at the time of the first interview, all eighty completed an interview in the first wave, and 90 percent of mothers completed the wave 2 interview.4 Interviews were audiorecorded and transcribed. We use pseudonyms for all mothers and children.
EXTERNAL FACTORS: LOCATION, EWIC, AND COVID-19
Although WIC is a federal program, it varies somewhat between states. For example, although most recipients use their benefits at regular grocery stores and markets, some states, such as California, have many specialized WIC stores (McLaughlin and Martinez 2021). The two states in our study, Louisiana and Minnesota, do not have such stores.
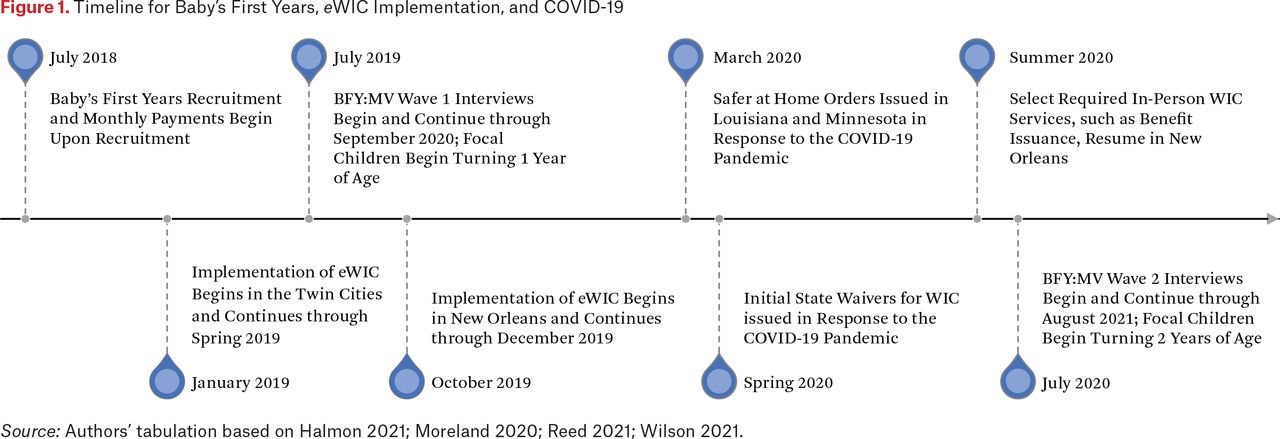
The timeframe of our wave 1 interviews that occurred in 2019 and 2020 coincided with substantial changes in the WIC program (see figure 1). First, benefits switched from being distributed via paper vouchers to being loaded on a debit-like card through the transition to eWIC. In New Orleans, eWIC was rolled out simultaneously across the sixteen WIC offices; mothers began receiving their EBT cards in the fall of 2019 as they had their WIC visits, and vouchers were phased out by the end of that year.5 In the Twin Cities, vouchers were phased in during the spring of 2019, and eWIC cards were gradually disseminated as WIC visits occurred.6 This was accompanied by a change in how recipients could use their allocated benefits. Among the redemption costs stemming from limited portability, WIC users had needed to separate their groceries into WIC and non-WIC items, have the cashier verify the WIC-eligibility of each item, and then turn over the paper voucher for that item. If a parent had a voucher for three gallons of milk, for example, but there were only two gallons in the store, the parent could either buy no milk, saving the voucher for another day, or give up the value of the third gallon of milk, receiving two for the price of three. This was no longer the case with eWIC.

The second major program change during the study occurred with the onset of the COVID-19 pandemic in 2020. Their daily life considerably altered, BFY: MV mothers dealt with shifting work and family responsibilities. Although not all mothers were in the workforce before the pandemic, many who were saw their jobs affected by it, temporarily or permanently losing jobs, or seeing their hours cut. In addition, they managed changes to their children’s routines, which for some mothers meant less availability of family and friends to help care for children, early care and education program closures, and transitions to virtual learning for their older children. These changes have the potential to influence mothers’ perceptions of WIC’s benefits and costs, because those experiencing job or income loss could see WIC benefits as having more value whereas those managing the new routines of their children might find the administratively requirements more difficult to satisfy.
Initially, WIC offices in both BFY: MV locations suspended in-person visits in response to COVID-19. In New Orleans, some of the required in-person services resumed in July 2020, but in the Twin Cities, services remained remote as of October 2021 unless in-person services were requested and could be accommodated.7 Research has found that program modifications in response to the pandemic eased some, but not all, of the program access barriers families faced (Barnes and Petry 2021; Barnes and Riel 2022). Marianne Bitler, Hilary Hoynes, and John Iselin (2020) find that WIC is a countercyclical program, meaning that it may have helped to counteract the pandemic-induced economic downturn. In this study, we observe whether and how these experiences around eWIC and the service changes due to the pandemic shaped mothers’ program perceptions and the burdens they cited in accessing or using benefits.
ANALYSIS
Because of its qualitative approach, BFY: MV allows for the possibility of discovering unanticipated themes or factors that are not included in the larger study’s surveys (DeLuca et al. 2012), including our analysis of mothers’ experiences with WIC. We entered all wave 1 and wave 2 transcripts into Dedoose 9.0.17 and used this qualitative software for our analysis. Because the semi-structured interviews covered many topics, we began by identifying all excerpts in which mothers discuss topics related to food security and then narrowed to those specific to WIC. Because we did not ask specifically about administrative burdens with WIC, we draw on the narratives mothers spontaneously offered during the interviews.
We used both inductive and deductive approaches to our coding. We structured our coding hierarchy to capture mothers’ perceptions of WIC as high cost, low cost, high benefit, or low benefit. Within each of these codes, we developed subcodes. We drew on the literature regarding administrative burden to organize the category of WIC’s high costs, creating subcodes for learning costs, psychological costs, and compliance costs (Herd and Moynihan 2018). Within learning costs, we also specified when mothers cited redemption costs (Barnes 2021). We developed the subcodes for the categories of high benefit, low benefit, and low cost based on the perspectives shared by mothers in the interviews. Under low cost, we included subcodes regarding convenience, including those created by eWIC and remote services. We also included a subcode indicating an absence of noted costs related to WIC participation. The subcodes for WIC being high benefit included valuing the baby formula it covered, seeing value in WIC-provided food and drinks, saving money by using WIC, lack of other supports or resources (making WIC resources relatively more important), WIC staff, education provided by WIC, and eligibility for other programs and services that comes with WIC receipt. We also included a subcode indicating whether there was an absence of benefit critique in a mother’s narrative about WIC. Last, subcodes related to the low-benefit perspective included the loss of highly valued formula, the limited value of WIC-provided food and drink, and the limited value of WIC’s child health and nutrition education.
We applied our coding scheme to identify all costs and benefits described by each mother at both waves. That is, it was mothers’ perspectives of what was costly and what was beneficial that drove our determinations, as opposed to our sense of what would be burdensome versus useful. For each mother at each wave, we were then able to determine the combination of mothers’ views as high benefit–high cost, high benefit–low cost, low benefit–high cost, or low benefit–low cost based on their descriptions of WIC’s benefits and costs. Although many mothers viewed the program uniformly (for example, all the views they expressed could be described as high cost), some described both high- and low-cost or both high- and low-benefit perspectives. For example, a mother may describe the ease of using eWIC (low cost) and the difficulty of getting WIC staff on the phone to ask a question about eligibility (high cost), or a mother may highly value the formula WIC provides (high benefit) but report that her children will not eat the other foods it offers (low benefit).8 We consider these nuances throughout our coding process. We also noted parents’ WIC receipt status at each wave and categorized their participation as continuing from wave 1 to wave 2, ceasing between wave 1 and wave 2, starting between wave 1 and wave 2, or having not participated at both waves 1 and 2.
Two researchers independently coded the excerpts for twenty-two of the eighty mothers and then worked together with a third study team member to resolve any differences in coding. This allowed for the development of coding reliability and for analytic discussion of the meaning of the codes and themes. Among the remaining cases, any questions of coding or categorization that arose were resolved through consensus by a pair from the research team. After completing our coding and categorization, we examined the patterns and themes that emerged by cost and benefit pairings and among the participation types. We investigated differences between the mothers receiving the large BFY gift amount and small-gift amount to account for the role of the unconditional cash transfer in our sample; we also examined differences between groups by site, given that the experience with the WIC program could vary by state.
RESULTS
We categorized mothers’ accounts of their experiences with WIC as high- versus low-cost and high- versus low-benefit to understand how the intersection of these cost and benefit experiences relate to mothers’ decisions to participate in WIC. Here, we first present the types of experiences that characterized reports. Table 2 presents the distribution of benefit and cost categories, which we discuss in depth. At least 91 percent of mothers indicated current or previous WIC receipt, meaning that nearly all had some familiarity with it.9 They followed four trajectories of WIC participation from the wave 1 to the wave 2 interviews (see table 3): continued participation (twenty-six, or 33 percent); did not participate at either wave (nineteen, or 24 percent); stopped participating (did at wave 1 but not at wave 2; fifteen, or 19 percent); or started participating (did not at wave 1 but began by wave 2; two, or 3 percent). We then explore how these views of costs and benefits varied by mothers’ patterns of participation over time, which sheds light on how the relative balance of perceived costs and benefits shapes program participation.
Distribution of Benefit and Cost Categories
WIC Participation over Time
HIGH BENEFIT
Among the eighty mothers, fifty-six (70 percent) described WIC in ways we characterized as high benefit at wave 1, when their children were about a year old; by wave 2, only thirty-two (45 percent) did.10 The most common reasons mothers saw benefit in the WIC program, especially before the children turned one (the age at which WIC stops covering formula), were the food and drinks it provided. Further, mothers appreciated saving money when they were able to stretch scarce resources to cover other costs, given that WIC was taking care of certain basic food costs for their children; some valued WIC because they lacked other resources, such as their SNAP benefits, making WIC a key part of their budgets. Although less common, some mothers highlighted the nutrition education WIC provided, that participation made them eligible for other programs or discounts (such as free zoo entry), or the helpfulness and friendliness of the WIC staff. Here we illustrate those themes most common among mothers who described seeing high benefit to WIC participation.
The first time we spoke to her, Trinity, a White mother of four, including baby Sebastian, from the Twin Cities, told us, “I do have WIC. So, that also is a huge life saver for, like, the formula. Now he’s on regular milk, but we’ll get three gallons for Sebastian, three gallons for [my other young son], and my older boys go through the gallons pretty quick.” Trinity actively manages her children’s food consumption and relies on WIC to ensure that, even when they run short on fruits and vegetables each month, she’s still able to provide the basics. “So, you know, I try to space it out or tell [the boys], you know, no cereal at night. . . . I always make sure that there’s milk, eggs, bread, butter, all the basics, and noodles.” For Trinity, WIC is essential to making sure her kids—not just those under five—are fed throughout the month.
During our wave 2 interview, when we asked about WIC, Eve, a Hmong mother of one who lives in the Twin Cities and at the time was pregnant with her second child, shared a similar perspective on the important role WIC played as a key household resource that shored up her food budget. She quickly pulled out her phone and opened the WIC app (a feature of eWIC) to show us how she uses WIC-approved foods to feed her child. “So currently for Eli and I, we get cheese, we get tofu, we get eggs, we get breakfast cereal, peanut butter, peas or beans, and whole grain items, fresh fruits, fresh or frozen fruits and vegetables, yogurt. And, of course, Eli, he is lacto [lactose intolerant], so we get soymilk for [him] and then we get regular milk for me. And juice as well.” Eve noted that using all of this food requires some creativity on her part, because her two-year-old is “really picky.” “So it is kind of hard to give him all these items at once. But he really does love his bread. He likes to eat cheese, but it has to be incorporated like in the bread. Like, for example, like a grilled cheese. . . . So it just really depends on his mood some days, and then everything else he just intakes it other days, but he loves to switch his vegetables.” Even with her son’s food tastes changing from day to day, she says of WIC, “It’s working great.”
Mothers who lacked alternative resources and whose children’s food preferences matched the items WIC provided valued these benefits as well as the money they saved and the holes in their budgets WIC filled. WIC was a core element of their food budgets, fulfilling the program’s stated mission of “providing nutritious foods” to “safeguard the health” of participating families.
LOW BENEFIT
The proportion of mothers who reported limited benefits to WIC participation remained stable from wave 1 to wave 2, seventeen (21 percent) and eighteen (25 percent), respectively.11 Here, the temporal nature of how mothers weighed the costs and benefits of the WIC program emerged. Mothers saw WIC as offering low benefits for one of two reasons: they no longer received the one thing from WIC that they highly valued (formula) or they saw limited value in the foods and drinks WIC provided.
At a baby’s first birthday, WIC stops covering the costs of formula, which some mothers referred to as milk or baby milk. This marked a turning point in many mothers’ relationships with WIC. As Cassandra, a Black mother of one in New Orleans, explained at our wave 2 interview: “The food that they gave me, my baby really wasn’t eating. . . . The main reason why I were getting WIC was because I needed the milk. Milk assistance. So, you know, once she stopped using the milk, I really didn’t need the WIC [any] more.” The many mothers like Cassandra are correct in a financial sense, in that the value of what mothers typically described being prescribed in formula (seven cans per month x $20 per can = $140, according to several mothers’ estimates) far outstripped the value of what they were prescribed in cows’ milk (three gallons per month x $3.70 per gallon = $11.10).12 The financial gains to WIC participation therefore objectively change with the transition from formula to milk (see also Schanzenbach and Thorn 2020).
When mothers cited issues with specific foods, it was often not being prescribed the kind of milk they preferred (such as 1 percent rather than whole or cows’ milk rather than soy) or being limited to kinds of baby food or cereal no one in their family wanted to eat (such as cereal with low or no sugar). More simply, the foods prescribed by the program did not match participants’ preferences. When we spoke with Patrice, a Black mother of five, including toddler Demyah, in New Orleans, at wave 2, she told us that the WIC food package did not match what her family wanted to eat. “I stopped getting WIC. I mean, they don’t give us what the kids eat, and it just like pile up and pile up. And I feel like other people could get that. They give us, like, one percent milk, and they give us, like, for the cereal. But the kids don’t really eat cereal. The only cereal they probably will eat is the Cheerios, and they don’t really eat that. . . . Demyah don’t drink cow-base milk. I let her drink SILK soy milk.” Some mothers described being able to get other kinds of milk alternatives (soy, almond) through WIC. The state WIC programs in Louisiana and Minnesota allow for the purchase of soy milk, for example. However, some mothers were under the impression that they would only be offered cow milk through WIC and so chose to forgo WIC and purchase their chosen milk alternative themselves. Others saw limited value in the products to which WIC gave them access, leading them to see limited benefits to program participation.
HIGH COST
The proportion of mothers who saw WIC participation as costly was fairly consistent between waves 1 and 2, twenty-three (29 percent) and twenty-seven (38 percent), respectively. By far, the most common reason mothers described participation as costly was compliance costs, such as having to manage appointments—remembering to keep them, finding time in a busy schedule for them, difficulty scheduling them around work or other obligations, arranging transportation to them, and bringing children to the appointments—and dealing with any necessary forms and documents. Issues around appointments were the primary cost cited. In addition, some mothers described learning costs, either learning about the program (pre-enrollment) or learning how to navigate the program (after enrollment), or psychological costs of the program, the stress or stigma of interacting with unhelpful staff.
Among these potential burdens, as discussed, compliance costs emerged most frequently. For example, Jaclyn, a Black mother with six children in the Twin Cities, said that her husband was opposed to getting help from any assistance programs, so Jaclyn juggled a lot on limited resources. They did receive WIC for some of their now-older children. For their youngest, however, making it to the appointments proved to be too much: “I never got it with Hassan though. I don’t know, I missed appointment. And then, I don’t know, something came up. [The WIC staff member] always called me, ‘You come into the WIC appointment? You coming?’ Something always keep coming up. I never got the WIC with Hassan.” For Jaclyn, complying with the required frequency of WIC appointments was too difficult to continue participation; that is, the compliance costs were too high. Similarly, the first time we met Simone, a Black mother of one in New Orleans, she told us that finding time in her schedule to get to the WIC office has stood in the way of her ongoing participation. “I was getting WIC. I can always go and still get it or whatever. I had just been so busy with work. Like with me working Monday through Friday, I haven’t had a chance to get up there and get it.” As it was for Jaclyn, the requirements to go to the WIC office while juggling work and childcare raised the compliance costs above what Simone was willing to pay. The ease of being able to “always go and still get it,” which Simone described, changed with the onset of the COVID-19 pandemic, however.
Multiple mothers cited a concern over in-person appointments during the pandemic as a reason they had stopped using WIC. Especially because they had to bring their children with them as part of the WIC appointments, they saw the health risks of going to a WIC appointment as outweighing the benefits.13 When we met her at wave 1, Tori, a White mother of three in New Orleans, told us she had stopped receiving WIC because she could not make her appointments.
I have issues missing my WIC appointments, apparently, since this pandemic started, especially. I’ve missed two appointments, and because we don’t have a car and just the way, like, one time it was raining. I don’t even remember what happened the second time. We weren’t able to make it. So, it just kind of sucks, but otherwise, other than having to go there physically and have the appointment, it would be good if it was other than that . . . if we could do applications online and/or video phone call like we can for SNAP.
“That sucks,” she concluded about in-person appointments. “That sucks without a car.” The combination of transportation issues and the risks of in-person meetings during a pandemic made Tori feel that the costs to WIC participation were high.
For many, redemption costs remained a significant hurdle even with the switch to eWIC. For some mothers, eWIC compounded the burdens of redeeming benefits given that they found navigating the program more difficult than before. At wave 1, when we asked about her experiences with WIC, Alisha, a Black mother of three in New Orleans, said, “Well, it was okay, but now that they upgraded to a credit card, and you can only go to like grocery stores like Walmart and [grocery store], it’s just too much. You have to walk around the store. You have to see what’s for WIC and what’s not for WIC. It’s a lot. It’s a lot.” Other mothers confirmed that fewer stores accepted their benefits after the transition to eWIC. When we met her at wave 2, Serena, a Black mother of three in New Orleans, told us she had received WIC in the past but was not currently because of the problems she faced trying to redeem those benefits with the eWIC card: “I think with this card thing they have made it complicated. Less places take it now, so it just really made it bad.”
At wave 2, Yasmin, a Black mother of three in New Orleans, carefully walked us through what the process of using WIC was like before and after the switch to eWIC:
When you get to the register, you tell them that you have a WIC. Alright? They got to call somebody over, see that if they don’t come or if they don’t answer the radio, it’s hard, you got to stand there, and the people behind you are like ‘What’s going on?’ I keep apologizing, ‘I’m so sorry, but I have a WIC, you know. I am really sorry,’ and someone finally comes over, they check the card, and then what you should have in your basket pops up on their screen, so if you don’t have what’s in their basket you pay the difference if that’s what you really want. . . . Nothing is labeled in the aisle for WIC. It’s just a whole—you got to ask somebody. . . . “Is this available on WIC?” They don’t know. “Let me call somebody.” I’m just like, “Oh god, please. Let it be over.” So, I mean it’s a good thing to have. But the process you have to go through to get it, it’s horrible.
Yasmin compared this experience with what it was like before the switch to eWIC, when her paper vouchers were accompanied by a sheet of paper listing what she was eligible to receive. “Well, before the process changed, all you had to do was sign the back of it. Look at a sheet of paper. . . . I love being a visual person. I can’t do things, you know, offhand. I can’t read it once, and then get it. I need to look at this. . . . That way I know exactly what I go get, I know exactly what I need. . . . They made it way more complicated, and a lot longer.”
As Yasmin explained, eWIC increased redemption costs for her—the time and effort of redeeming the benefits, learning what she could and could not purchase, and dealing with the stigma she felt attached to WIC use. Even though the eWIC card may be less distinct from the payment methods non-WIC customers are using, the process of involving store staff and holding up the line made Yasmin feel even more singled out than she did when using paper vouchers. The challenges of finding a store that accepted WIC or finding the WIC-approved items led some mothers to leave the program. Others, who continued to receive WIC, stopped redeeming all of their benefits because figuring out what they could select was too much effort.
As Nakeisha, a Black mother of two in New Orleans, told us at wave 2: “That WIC is something else. I can’t deal with them. I only get the main stuff that I know because half of the stuff on there they be giving you, you bring it to the counter, [and you’re told] that’s not the right one. So, I just want to get the main stuff that I know that I can get.” Nakeisha avoided some of the redemption and learning costs of using WIC, but at the price of forgone food assistance for her family. Like Nakeisha, other mothers described paying out of pocket for foods WIC would have covered in order to avoid the costs of WIC participation.
LOW COST
Mothers were quite likely to describe WIC participation as low cost at wave 1, fifty (63 percent) doing so; by wave 2, only twenty-eight (39 percent) did.14 In expressing this low-cost perspective, mothers often had little to say about their experiences. Some, however, used words such as easy to describe the process of enrolling in and using WIC. Some noted the convenience of new features, including eWIC and the pandemic-induced switch to phone appointments from in-person ones.
For example, Jayla, a Black mother of one in New Orleans, is fairly typical of this group; for her, participation was not particularly notable at our wave 1 interview, either in what they received or the challenges in navigating the program. She said, “I get WIC for Mila . . . We just get like milk, juice, stuff like that, yogurt, things like that. . . . It’s just good, no issues.” At wave 2, her story was the same: “I like WIC, too. I don’t have no problems with them either.”
Some mothers viewed the switch to eWIC as increasing redemption costs, as described. Others felt differently. At wave 1, Alexandra, a Black mother of one in the Twin Cities, described the eWIC card as “pretty easy to use.” Her husband, in contrast, did not feel comfortable so instead used their BFY card when he was at the store buying baby food. The plus side of the card, for some mothers, came in the flexibility eWIC offered in redeeming their benefits. Whereas before they needed to redeem their voucher for all of a prescribed food item at once, such as getting all three prescribed gallons of milk or getting fewer and forgoing the remainder for the month, eWIC allowed them to purchase items as needed. As Imani, a Black mother of four in New Orleans, told us at wave 1, “With the vouchers, you have to get everything at one time. With the card, you can stretch it out throughout the month. . . . I think the card is much better.” At wave 2, Chantel shared a similar sentiment—“I don’t have to get everything at one time”—and pointed out how much easier it was for her to manage the food benefits for all three of her children on WIC with everything loaded on one card rather than spread across three separate sets of vouchers.
Because the switch to eWIC for some mothers came shortly before the pandemic led to widespread shutdowns, some mothers saw eWIC as easing the burdens of having to go into the WIC office. As Soledad, a Latina mother of three, living in the Twin Cities, told us at wave 2, “[WIC is] much better because now they handed [you] a card, and you no longer have to go to their office. You schedule appointments through the phone . . . much better.” As we see here, the response to the eWIC transition among mothers was far from uniform, with some feeling it eased the costs of program use while others saw it as increasing them substantially.
We use these perspectives, of WIC as high- versus low-benefit and high- versus low-cost, to understand the participation patterns we see over time, from wave 1 to wave 2.
CONTINUED PARTICIPATION
Of the eighty mothers, only a minority—twenty-six (33 percent)—continued their WIC participation from wave 1 through wave 2.15 At wave 1, most of these mothers (sixteen, 62 percent of those who continued participation) described WIC as high benefit and low cost; in this group, four described WIC as high benefit–high cost and four described it as low benefit–low cost. Mothers in this group tended to describe the benefit application process as easy, and they valued the food WIC provided, particularly before their child was one, when WIC was helping cover the costs of formula. Even among the mothers who continued participating in WIC across interview waves, several noted that their families did not eat some of what WIC covered, and so they did not redeem all of their benefits; they ended up with those foods piling up at home, or they shared them with other family members. The difference in moms’ enthusiasm for WIC based on whether they had an infant for whom it was covering formula was notable.
NO PARTICIPATION
Of the eighty mothers, nineteen (24 percent) did not receive WIC at either wave. Many in this group had participated in WIC in the past but were just not receiving it at the times of the interviews. At wave 1, these mothers (seven, 37 percent) most commonly described WIC as high benefit–high cost; the rest were evenly spread across the other perspectives. Mothers in this group had often received WIC but stopped doing so by the time of our wave 1 interview, sometimes because of compliance challenges or the lower value they saw WIC having after their babies were one. Other mothers, however, had not received WIC for the focal child, even if they had done so with older children; making it to appointments was often a key difficulty. Some mothers had stopped using WIC when they no longer received formula—some even described their WIC benefits as stopping at that point, as opposed to saying they chose to stop receiving WIC. As Michelle, a Black mother of three in New Orleans, reported, “They said he aged out.” Tori, introduced earlier, told us that it began to matter less if they were receiving WIC once her son aged out of formula because “those are the most important days to have it.” In recounting when they had last received WIC, mothers often pegged it to the time when their youngest child was still drinking formula, emphasizing what a key turning point in their relationship with the WIC program the end of formula coverage represents.
CEASED PARTICIPATION
Of the eighty mothers, fifteen (19 percent) were using WIC at wave 1 but stopped by wave 2. We saw their views of the program evolve over time. At wave 1, a majority (ten, or 67 percent) described WIC as high benefit–low cost. By wave 2, however, none did so: about a third described it as high benefit–high cost and a third as low benefit–low cost. It would seem that for some of these mothers, the costs or benefits of participation changed, leading them to decide that taking part in WIC was no longer worthwhile. Two factors stood out. First, some mothers found that the milk WIC prescribed did not match their children’s or their preferences and thus WIC no longer met their needs; alternatively, they had needed help affording formula—one mother described WIC as “milk assistance”—but once their children switched to milk, they could more easily cover these costs with their earned income and SNAP benefits. Second, with the beginning of the pandemic, as WIC—and so many other offices—struggled to transition to a virtual world, mothers’ relationships with the program were disrupted; many simply never went back. As Jade, a Black mother of two in New Orleans, told us, “I have not received WIC since, in months . . . because the pandemic started and they wasn’t accepting anymore, anymore appointments. So, when I did actually make the appointment, it was basically for . . . [my toddler] to go to the appointment, but they never gave me a date or a time. They was just like come in whenever you could, but then, you know, my baby couldn’t go in . . . so I just never went.” Other mothers similarly recounted finding the WIC offices closed or requiring their child’s in-person attendance during the pandemic, which they did not feel comfortable with, and so their participation in WIC ended because they could not or did not comply with program requirements.
BEGAN PARTICIPATION
Of the eighty mothers, two (3 percent) were not using WIC at wave 1 but had begun doing so by wave 2. Because so few people had this experience, we cannot identify patterns in their program perspectives. Like some in the no participation group, the mothers who appear to have begun participation at wave 2 had actually received WIC previously but were not at the time of the wave 1 interviews. This underlines the sometimes unstable nature of parents’ experiences with WIC, cycling on and off benefits, particularly when their receipt is interrupted by a missed appointment.
VARIATION BY SITE AND OTHER RESOURCES
At wave 1, just under two-thirds of mothers in both sites reported WIC participation. Likewise, their perspectives on costs and benefits of participation were similarly distributed within each site, with the exception of a higher likelihood in New Orleans of seeing WIC as low benefit–low cost (18 percent of mothers, relative to 10 percent in the Twin Cities).16
Because this study was conducted in the context of an intervention, attending to whether and how the additional income received through BFY by the large-gift group ($333 per month) relative to the small-gift group ($20 per month) is related to use and views of WIC’s administrative burdens is important. At wave 1, we see no differences in WIC receipt between groups: just under two-thirds of mothers in both gift groups reported that they received WIC for the focal child. At wave 2, despite a substantial decline in WIC receipt overall, differences by BFY gift group remain small, 38 percent of large-gift group mothers and 41 percent of small-gift group mothers reporting receipt. Additionally, the perspectives mothers shared on the benefits and costs of WIC participation were distributed similarly within each group. This would suggest that the additional dollars from BFY do not alleviate the need for WIC or change the perception of the costs and benefits associated with WIC participation. Given that all BFY mothers were below the federal poverty line at the start of the study, and that the WIC program reaches up to 185 percent of the federal poverty line, this finding may not be surprising.
In addition, we can examine how mothers’ participation in another common nutrition assistance program, SNAP, is related to their WIC participation. At wave 1, three-quarters of those not receiving WIC were on SNAP, as were two-thirds of those on WIC. This pattern continued at wave 2: mothers were more likely than not to be on SNAP regardless of WIC participation. Mothers therefore do not appear to be uniformly substituting SNAP for WIC. Despite their receipt of these other resources, mothers who received SNAP were likely to describe WIC as a high-benefit or a low-cost program at wave 1. These trends continued at wave 2, suggesting that, for many mothers, WIC and SNAP are more complements than substitutes.
DISCUSSION
We demonstrate how the circumstances of family life, shifting food preferences, and the receipt of other resources shape WIC-eligible mothers’ perceptions of the costs and benefits of program participation. We find evidence that mothers’ perceptions vary over time and, in some ways, shape program participation trajectories; need alone does not drive participation decisions. The additional income from BFY does not appear to shift the costs and benefits of WIC that mothers randomly assigned to the larger versus smaller gift groups perceive. Many emphasized the high compliance and redemption costs, showing some ways in which structural factors drive perceived costs. However, the high value of WIC benefits for infants made program participation worth the burdens of accessing and redeeming benefits. We find that perceptions of the value of the WIC program shifted as children aged out of formula and WIC-approved foods no longer matched families’ preferences. As the value of benefits declined, the high compliance and redemption costs discouraged many mothers from staying on the program. Child age and the resources that mothers had to navigate program participation costs, therefore, worked to sort who gained and who withdrew from WIC benefits. The burdens appear to be disproportionately affecting women who cannot afford the costs of participation. These findings have suggestive implications not only for WIC but also for other programs with high redemption costs, such as Medicaid, childcare subsidies, and Housing Choice Vouchers (Barnes 2021).
This points to two key takeaways from this study. First, for WIC participation, formula is a singularly important benefit among the set of foods currently offered. Second, costs matter as much, if not more than, benefits in shaping prospective mothers’ willingness to participate, especially after they lose formula benefits. Because we follow families over a year, we see how perceptions of the relative mix of costs and benefits evolve over time. Further, we see that when participation was disrupted, families may not return, suggesting some degree of path dependency in program participation patterns. Some WIC offices struggled to maintain connections with or serve families at the onset of the pandemic; even though they were able to adapt their service models to provide services virtually, the initial disruptions had longer-term implications for some families, who did not return to seek benefits.
As studies demonstrate, the evidence that eWIC reduced administrative burden is mixed (Leone et al. 2021; McElrone, Zimmer, and Anderson Steeves 2021). For some mothers, eWIC increased the burden as stores and mothers alike struggled with the adjustment. This experience, though, was not universal: some mothers saw the new program delivery system as cutting their redemption costs. Even so, eWIC was insufficient in addressing the main burdens parents cited as shaping their program experiences—compliance costs. Many of the parents interviewed lacked the time and transportation resources to make it to in-person appointments. It therefore follows that eWIC does not appear to address a primary administrative burden facing potential and current program participants.
This study, of course, is not without limitations. First, we capture perceptions of administrative burdens that may arise from implementation failures rather than burdensome structural program features. We lack qualitative data from the staff’s perspective to understand whether some of WIC participants’ burdensome experiences stem from policy implementation failures. Further, as is true of most qualitative studies, the results are not generalizable; the intention of this study is to examine the variety of perspectives and experiences mothers describe with WIC. Our sample size limits our ability to make comparisons among our respondents. Whether the frequency of these perceptions varies substantially within other populations or locations is an open question. Because families are WIC-eligible up to 185 percent of the poverty line, but our sample was recruited from mothers who were below 100 percent of the poverty line, we are missing the perspective of those who have relatively higher incomes. Second, we only follow mothers over a limited time around the birth of one of their children; we see that experiences change over time and may be different with each child, depending on a mother’s circumstances, and so the points of view mothers express about the WIC program should be expected to vary over time. Third, the COVID-19 pandemic disrupted many aspects of life, including those germane to families’ participation in WIC, such as their willingness to ride public transportation to get to appointments and whether WIC offices were open and parents willing to take their children in for appointments. Although some mothers were dissuaded by these obstacles, others may have continued their participation longer than they otherwise would, as the costs associated with attending in-person appointments were eased for a period of time during the pandemic with the option for phone appointments. Looking to the future, the facility with which social service providers pivot their service delivery will be key to maintaining access to program participation as climate change and associated extreme weather events grow in their disruptive impact.
We see three take-away public policy messages from this study. First, those eligible for a program may become more or less willing to tackle the burdens of participation depending on the benefits of doing so; neither these costs nor these benefits are static for participants. For example, with the loss of formula benefits once children turned one, many mothers were no longer willing to tackle the same set of costs. That is, the administrative burdens of program participation must be assessed in a relative way. Second, eWIC created and eased costs of program usage for different mothers, depending on how easy both they and the stores around them found the new system to use. More scaffolding to ease transitions for both individuals and the stores through which they redeem benefits could be useful. Third, policymakers ought to reflect on which administrative burdens families feel the weight of the most and which eWIC actually resolves. We see a mismatch between these, which suggests room for further program refinements to address the burdens families perceive as most costly. For example, WIC offices now have experience administering the program without quarterly in-person visits, which suggests an opportunity to reflect on whether and how often in-person visits should be required in the future, since these are a barrier mothers see to their ongoing participation. Given how many mothers participate in both SNAP and WIC, for example, programs could work around administrative silos to allow families to complete their requirements for both programs simultaneously in one visit.17 This could raise the benefits of going to a WIC appointment, given that SNAP benefits are substantial for many families, an average of $392 per month for households with children (Center on Budget and Policy Priorities 2019), and lower the costs, because it would limit the number of appointments parents need to juggle. However, this ease of access must be weighed against the potential loss of relationships with WIC staff that some parents build and value through their WIC appointments (Barnes, Michener, and Rains 2023).
Using the WIC program as a case, this study advances our understanding of how lower-income families in the United States assess and make decisions in light of the administrative burdens of participating in means-tested assistance programs. These decisions are based on their implicit assessment of the relative balance of the costs and benefits of program participation; notably, however, the compliance and redemption costs that weighed most heavily varied across mothers. Inequities across mothers, such as their facility in navigating the eWIC app, their access to personal transportation, employment schedules, and the other resources on which they had to draw (such as SNAP), changed their perceptions of the costs and benefits attached to program participation. Further, mothers whose children’s food preferences aligned with WIC’s food packages receive greater benefits from the program: WIC food is only valuable insofar as children are willing to eat it.
The intention of the WIC program is to boost mothers’ and children’s adequate nutritional intake. Although the weight of the evidence suggests that WIC is effective at achieving this goal and in promoting positive child development (Currie and Rossin-Slater 2020), opportunities to reach more children for a longer span in the early childhood period by addressing the administrative burdens mothers must navigate to access these supports are clear. Because WIC participation rates are well below eligibility rates, room for WIC’s impact to grow on the healthy development of economically disadvantaged children is substantial. WIC shows potential as a tool for giving children access to a more equal start in life, but currently administrative burdens are impeding its ability to fully deliver on this promise.
FOOTNOTES
↵1. WIC does not condition eligibility on immigrant status, but Carolyn Heinrich and her colleagues (2021) offer an example of discrimination when a WIC worker imposed additional compliance on a Latino man seeking benefits for his infant.
↵2. Some states require stores to connect their systems to the state’s WIC EBT system daily to reconcile their WIC authorized products with any state-level changes to food packages (for more information, see Louisiana WIC 2022; Minnesota WIC n.d.).
↵3. Because mothers were recruited over the course of approximately a year, they are interviewed in different months, spread across that year, so that their children are a similar age at the time of the interview. For example, one mother may have been recruited in December 2018 and then completed a wave 1 interview in December 2019, whereas another may have given birth and been recruited in March 2019 and completed a wave 1 interview in April 2020.
↵4. In light of issues with Child Protective Services, we did not attempt to recontact one of the mothers at wave 2, therefore our total possible sample size at that wave is seventy-nine.
↵5. Chantell Reed, New Orleans eWIC and COVID-19 related changes, telephone conversation, 2021.
↵6. Valeesha Halmon, Ramsey County eWIC and COVID-19 related changes, telephone conversation, 2021; Jill Wilson, Hennepin County eWIC and COVID-19 related changes, telephone conversation, 2021.
↵7. Halmon, telephone conversation, 2021; Reed, telephone conversation, 2021; Wilson, telephone conversation, 2021.
↵8. When we categorize mothers’ perspectives as high benefit–low cost, and so on, we do so primarily based on whether they reported any high benefits or costs; if they reported both high- and low-cost or benefit perspectives, we considered what category best captured their general sentiment about the program and categorized their views accordingly.
↵9. Of the eighty mothers, seventy-three reported current or previous WIC receipt and four that they had no experience with WIC. We were unable to discern whether the remaining three had any experience. To avoid overestimating, we calculate the overall rate of previous or current participation using the full sample of eighty mothers; the rate may therefore be an underestimate.
↵10. Because of missing data and the inability to categorize some responses, benefit and cost totals at each wave do not add to 100 percent. We report percentages based on the full sample at each interview wave to avoid potential overestimates (for more detail, see table 2).
↵11. The reason the proportion of mothers describing WIC as high benefit declines from waves 1 to 2 without a comparable increase over time in those describing it as low benefit is that we have less information about mothers’ views at wave 2 due to attrition; interviewers inadvertently skipped this question; or mothers did not say enough for us to characterize their views, such as indicating that they did not receive WIC but not elaborating.
↵12. These are the estimated value to mothers of the WIC-prescribed formula versus milk. The cost to the government is distinct, however, since WIC pays a far lower rate for formula as negotiated by states, often paying only 15 percent of the market cost (Oliveira 2011).
↵13. In response to the pandemic, WIC offices in both New Orleans and the Twin Cities transitioned to remote services after their state’s receipt of a federal waiver. In July 2020, New Orleans WIC offices returned to some in-person services, including brief education and benefit issuance (Reed 2021). In the Twin Cities, Hennepin County continued remote services into the fall of 2021 (Wilson, telephone conversation, 2021), whereas over the course of the pandemic, Ramsey County began offering some in-person services at the client’s request and curbside pickup of eWIC cards (Halmon 2021).
↵14. See previous footnote for some reasons this declined without a comparable increase in the proportion viewing it as high cost.
↵15. Due to missing data and an inability to categorize some mothers’ responses, participation categories do not add to 100 percent. We report percentages based on the full sample of eighty mothers to avoid potential overestimates (for detail, see table 3).
↵16. Because the interviewers in Minnesota were disproportionately likely not to gather information on WIC status at wave 2, we do not offer site comparisons focused on wave 2.
↵17. In some places, like New Orleans, initial eligibility determinations are already coordinated across assistance programs, but the recertification process is not. Further, as mothers described, SNAP program appointments were fully remote, making demands for in-person appointments in WIC more exceptional.
- © 2023 Russell Sage Foundation. Barnes, Carolyn, Sarah Halpern-Meekin, and Jill Hoiting. 2023. “‘I Used to Get WIC . . . But Then I Stopped’: How WIC Participants Perceive the Value and Burdens of Maintaining Benefits.” RSF: The Russell Sage Foundation Journal of the Social Sciences 9(5): 32–55. DOI: 10.7758/RSF.2023.9.5.02. The authors thank the students and interviewers who have worked on the Baby’s First Years: Mothers’ Voices study and, particularly, the mothers who shared their time and stories with us. The Baby’s First Years: Mothers’ Voices study receives financial support from the Heising Simons Foundation, the Office of Planning, Research, and Evaluation in the Administration for Children and Families, and the Russell Sage Foundation. For more study information, see https://www.babysfirstyears.com. Please direct correspondence to: Carolyn Barnes, at cb120{at}duke.edu, 201 Science Dr., Durham, NC 27705, United States.
Open Access Policy: RSF: The Russell Sage Foundation Journal of the Social Sciences is an open access journal. This article is published under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.
REFERENCES
In this issue





{kind=link}
Jump to section
- Article
- Abstract
- LITERATURE REVIEW
- CONTEXT
- BABY’S FIRST YEARS
- CURRENT STUDY
- METHODS
- DATA
- EXTERNAL FACTORS: LOCATION, EWIC, AND COVID-19
- ANALYSIS
- RESULTS
- HIGH BENEFIT
- LOW BENEFIT
- HIGH COST
- LOW COST
- CONTINUED PARTICIPATION
- NO PARTICIPATION
- CEASED PARTICIPATION
- BEGAN PARTICIPATION
- VARIATION BY SITE AND OTHER RESOURCES
- DISCUSSION
- FOOTNOTES
- REFERENCES
- Figures & Data
- Info & Metrics
- References
Related Articles
Cited By...
- No citing articles found.