
Abstract
Along with the late 1980s Medicaid expansion for pregnant women and children, states implemented multiple reforms to reduce administrative burdens and facilitate access to Medicaid and prenatal care. We use National Vital Statistics birth data from 1985 to 1994 and a difference-in-discontinuities approach to compare the effectiveness of these reforms for improving infant health and access to prenatal care. Results indicate that combinations of reforms to reduce administrative burdens increased Medicaid enrollment and improved infant health nearly as much as Medicaid expansion. In most cases, these reforms yield larger benefits for racially and socioeconomically marginalized mothers, but targeted reforms could better address unequal barriers and further improve equality. Benefits of the reforms are larger in states with more physicians per capita, particularly for marginalized mothers. Overall, results suggest that combined policy responses to reduce multiple burdens at the same time are needed to address unequal barriers.
Enacted in 1965, Medicaid increased access to health care and improved infant and child health, yielding long-term educational and economic benefits (Cohodes et al. 2016; Miller and Wherry 2019; Goodman-Bacon 2018; Levine and Schanzenbach 2009; Currie and Gruber 1996, 2001). Medicaid had larger health benefits among non-White infants because they were six times more likely to be eligible than White infants (Goodman-Bacon 2018, 8). By design, mothers with low socioeconomic standing had higher eligibility rates, and Medicaid improved health more among their infants and children as well (Qureshi and Gangopadhyaya 2021; Wherry et al. 2018; Boudreaux, Golberstein, and McAlpine 2016; Baldwin et al. 1998). Medicaid increased equality of infant health by race and socioeconomic status (SES), but the equalizing effects could have been larger with lower barriers to enroll and access care.
Among pregnant women eligible for Medicaid, administrative burdens limit access to both Medicaid enrollment, because of application length or required program knowledge, and prenatal care, because of distance, transportation, or time requirements (Christensen et al. 2020; Herd and Moynihan 2018; Sommers et al. 2019). Resource-related disparities by race and education can intersect to exacerbate administrative burdens for particular groups of Medicaid-eligible women, limiting the equalizing potential Medicaid.
A challenge in addressing unequal access to care is identifying which types of reforms could most effectively reduce administrative burdens and increase equality of infant health and access to prenatal care. No single reform may suffice because administrative barriers vary by both race and education: combinations of reforms may be required to address these unequal barriers. This study uses state variation in reforms adopted to reduce burdens to Medicaid enrollment and health care for pregnant women during the late 1980s. We leverage this variation to examine how particular combinations of reforms influence infant health and prenatal care uptake.
Responding to high infant mortality rates, a series of federal changes from 1987 to 1990 increased the income threshold for Medicaid eligibility among pregnant women and infants. At the same time, states implemented various reforms to reduce barriers for eligible women to enroll in Medicaid and to access prenatal care. These reforms varied across states, but included shortened and expedited applications, asset test removal, presumptive and continuous eligibility, home visits, transportation, coordinated care services, and stationing eligibility officers at prenatal care sites. We use this unique policy context to compare how reform combinations aimed at reducing administrative burdens to Medicaid enrollment and health care influence infant health and prenatal care usage. We examine effects by maternal race and education to understand implications for inequality of infant health.
To preview our results, we find that combinations of reforms to reduce administrative burdens increase Medicaid enrollment and improve infant health and prenatal care. Our findings suggest that multiple approaches to reduce administrative burdens can improve infant health nearly as much as Medicaid expansion. In most cases, these reforms yield larger benefits for marginalized groups and increase equality of infant health, but targeted reforms could better address unequal barriers and further improve equality. Overall, results suggest combined policy responses to reduce multiple burdens at the same time can help address unequal barriers.
THEORETICAL BACKGROUND
Over the past century, the United States experienced particularly high levels of infant mortality. Even as the infant mortality rate (IMR) decreased by about ninety deaths per one thousand live births from 1916 to 2000, the rate of decline has not kept pace with other high-income countries (Singh and Yu 2019). The United States went from having the twelfth lowest IMR in 1960 to the thirty-first in 2015 (Singh and Yu 2019). Further, preterm birth—a risk factor for infant death and low birth weight—rose during the later part of the twentieth century, from 9.5 percent in 1981 to about 12 percent in 2002 (Goldenburg and Culhane 2007).
Although the overall IMR declined over the course of the twentieth century, racial disparities in infant health persist. Black and American Indian women are especially likely to experience infant death and poor birth outcomes (Singh and Yu 2019; Sparks 2009). Socioeconomic differences in birth outcomes are also substantial. Low-income mothers are more likely to give birth prematurely than their counterparts in the top income quintile (Martinson and Reichman 2016) and socioeconomic inequality of infant health has increased over the last decade in the United States (Rauscher and Rangel 2020). Given these stalled improvements in birth outcomes, it is crucial to understand the factors that affect both overall infant health and inequality in its distribution.
The provision of public health insurance is one driver of infant health outcomes. With the introduction of Medicaid in 1965, infant and child health improved, yielding long-term educational and economic benefits (Miller and Wherry 2019; Goodman-Bacon 2018; Currie and Gruber 1996, 2001). Evidence suggests that higher Medicaid reimbursement rates are associated with greater prenatal care usage (Sonchak 2015) and Medicaid eligibility is associated with fewer infant deaths and greater health-care uptake (Currie and Gruber 1996; Moss and Carver 1998).
Health care during pregnancy is a second driver and has especially strong implications for birth outcomes. One study suggests that women who received no prenatal care had more than seven times higher odds of giving birth prematurely than women who received adequate prenatal care (Sparks 2009). Further, Lyudmyla Sonchak (2015) finds that an additional prenatal care visit is associated with longer gestation and a lower probability of giving birth to a low birth weight infant.
Not everyone has equal access to health care in general or prenatal care specifically. Black and Latinx Americans have lower health insurance rates than White Americans (Lillie-Blanton and Hoffman 2005) and Black Americans spend more years uninsured on average than Whites (Kirby and Kaneda 2010). Low-income and less-educated mothers are more likely to delay prenatal care or receive no prenatal care (Braveman et al. 2004). These disparities may explain some of the racial and socioeconomic inequality in birth outcomes. For example, Johnelle Sparks (2009) provides evidence that unequal prenatal care uptake is responsible for some of the racial and ethnic disparities in preterm birth.
In the U.S. context, lack of universal health insurance requires pregnant women to navigate two sets of administrative burdens: access to health insurance and access to prenatal care. Women with limited resources face barriers to Medicaid enrollment, such as long applications or required program knowledge, and to prenatal care, such as distance, transportation, or time requirements (Christensen et al. 2020; Herd and Moynihan 2018; Sommers et al. 2019). To improve equality of infant health, it remains unclear whether it is more effective to facilitate access to health insurance or to prenatal care among eligible pregnant women.
POLICY EFFECTS ON INEQUALITY AND INFANT HEALTH
Evidence indicates that Medicaid reduced inequality in infant health. Medicaid implementation had larger health benefits among non-White infants because they were six times more likely than White infants to qualify for Aid to Families with Dependent Children (AFDC) (Goodman-Bacon 2018, 8). Medicaid expansion in the late 1980s increased the use of obstetric procedures, but only among disadvantaged mothers, which had an equalizing effect (Currie and Gruber 2001). Medicaid expansion also reduced rates of low birth weight and infant mortality, with larger benefits among low-SES mothers (Levine and Schanzenbach 2009; Baldwin et al. 1998). In addition to improving infant health, Medicaid had benefits for educational achievement and attainment, income, and wealth (Brown, Kowalski, and Lurie 2020; Boudreaux, Golberstein, and McAlpine 2016; Miller and Wherry 2015; Jackson, Agbai, and Rauscher 2021).
Despite these benefits, Medicaid-eligible women faced substantial administrative burdens—particularly prior to the 1989 expansion—potentially limiting any equalizing effects of the policy. Administrative burdens include learning costs, compliance costs, and psychological costs that prevent eligible participants from enrolling in Medicaid or accessing health care (Herd and Moynihan 2018; Moynihan, Herd, and Harvey 2015). Administrative burdens to Medicaid enrollment include learning costs to find out about the program, determine eligibility status, and identify what information is required to enroll; compliance costs to assemble and provide appropriate documentation to apply and reenroll in Medicaid; and psychological costs to interact with Medicaid officials and enroll in a public program, which may have negative connotations or reduce self-esteem. Even with Medicaid, additional administrative burdens to access prenatal care include learning costs to find out what benefits are included and at which facilities; compliance costs to schedule and travel to appointments on time, and provide documentation required by health-care providers; and psychological costs to interact with health-care providers and respond to their recommendations (Herd et al. 2013).
The extent to which administrative burdens inhibit Medicaid enrollment and access to care is unequal by race and socioeconomic status. Marginalized pregnant women are at higher risk of experiencing substantial administrative burdens given unequal information, support, and stress in encounters with healthcare providers and Medicaid officials (McLemore et al. 2018; Vedam et al. 2019; Altman et al. 2019; Delaney and Singleton 2020; Rosenbaum 2003).
Unequal experiences of administrative burdens to Medicaid and prenatal care mirror research on administrative burdens in other spheres. Manasi Deshpande and Yue Li (2019) find that Social Security office closings disproportionately reduce disability insurance (DI) applications among low-SES individuals, suggesting that the economically marginalized are more burdened by barriers to program access. Further, among families eligible for unemployment insurance (UI), Black and Latinx families are less likely to receive UI benefits than White families (Parolin et al. 2023), suggesting unequal administrative burden by race-ethnicity.
Racial and socioeconomic variation in risk of administrative burdens may limit the equalizing potential of Medicaid expansion. If these burdens are not addressed, marginalized groups of women would continue to experience more barriers to care even after expansion. Thus Medicaid expansion without reforms to reduce administrative burdens could fail to increase access to Medicaid or prenatal care and yield persistent racial and SES inequality of infant health. However, expansion coupled with reforms that successfully reduce administrative burdens to enroll in Medicaid or to access prenatal care should increase equality in Medicaid enrollment, prenatal care, and infant health.
Alternatively, systemic racism could limit the benefits of Medicaid expansion even when coupled with reforms that reduce administrative burdens. Bias by program managers and patient-facing workers can shape how Medicaid policies are implemented (Camillo 2021), allowing unequal encounters with Medicaid and prenatal care to continue despite reforms. Pregnant women of color report disrespectful and stressful encounters with health-care providers (McLemore et al. 2018), and Black and Latina women often experience hostility, surveillance, and paternalism during prenatal care visits (Bridges 2011; Davis 2019). Racism can also result in misdiagnoses and lower-quality care for Black and Latina women, yielding lower benefits than the care received by White women on Medicaid (Rosenbaum, Markus, and Darnell 2000; Rosenbaum 2003; Sonchak 2015; Bridges 2011; Davis 2019). For example, Khiara Bridges (2011) finds that obstetricians often attributed abdominal pain in Black and Latina patients to sexually transmitted infections. Although we expect Medicaid expansion coupled with administrative burden reforms to increase equality in prenatal care and infant health, it is possible that racialized women may receive less benefit from prenatal care even after overcoming administrative burdens.
Evidence suggests that reducing administrative burdens should help counter inequality. Reducing them is generally associated with increased enrollment among Medicaid-eligible adults and children (Fox, Stazyk, and Feng 2020) and some policies may be especially effective at decreasing enrollment barriers for marginalized groups (Herd and Moynihan 2018; Remler and Glied 2003). For example, automatic Medicaid enrollment based on administrative data the state already holds increases enrollment (Dorn et al. 2009). Enrolling individuals who are presumed eligible similarly improves Medicaid enrollment (Piper, Mitchel, and Ray 1994).
Despite evidence of promising changes to reduce administrative burden, most research examines one policy change and one state at a time. Few studies systematically compare multiple attempts to increase program enrollment (Currie and Grogger 2002; Remler and Glied 2003). Rare exceptions (Herd and Moynihan 2018; Herd et al. 2013) study the case of Wisconsin from 1987 to 2011, comparing the effects of multiple procedural changes over time that altered barriers to enrollment. A key finding is that reforms interact with or depend on one another, so it is valuable to examine changes collectively rather than individually. This evidence highlights the value of examining multiple reforms, but analyses limited to any one state raise questions about generalizability to other populations or contexts.
The next step is to examine effects of multiple reforms simultaneously across all states to learn which types of policies most effectively increase access to health care and equality of health outcomes. We use a unique policy context with multiple policies aimed at reducing administrative burdens to compare effects on prenatal care and infant health. During the Medicaid expansion for pregnant women and infants in the late 1980s, states implemented various reforms to reduce burdens to Medicaid enrollment and to access prenatal care among eligible women. We take advantage of state variation in the reforms implemented with Medicaid expansion and variation in the timing of expansion to address the following research questions:
Do combinations of reforms to reduce barriers to Medicaid enrollment or to prenatal care increase enrollment, prenatal care, or infant health?
Do reform effects vary by maternal race-ethnicity or education?
Are reforms to improve access to enrollment or access to care most effective at increasing equality of prenatal care and infant health by race-ethnicity and education?
POLICY BACKGROUND
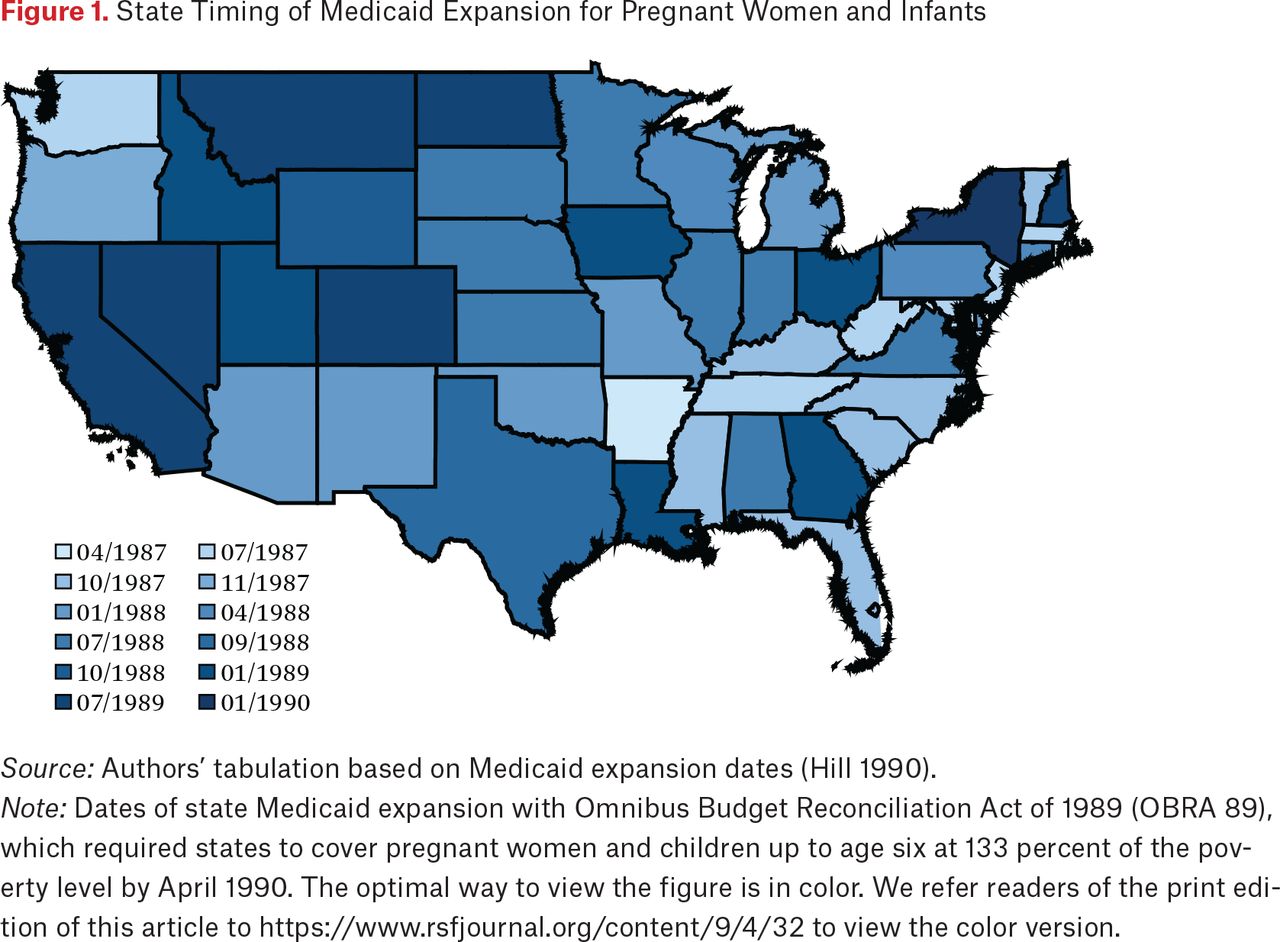
Before 1987, Medicaid coverage was tied to receipt of AFDC, for which the average state eligibility threshold was 48 percent of the federal poverty level (National Governors Association 1990). Responding to high infant mortality rates, a series of federal changes from 1987 to 1990 decoupled Medicaid eligibility from AFDC receipt and expanded access. After allowing states to expand Medicaid coverage to pregnant women and infants up to the federal poverty level regardless of assets effective April 1987 (OBRA 86), the Omnibus Budget Reconciliation Act of 1989 (OBRA 89) required states to cover pregnant women and children up to age six at 133 percent of the poverty level by April 1990 (National Governors Association 1990). Together, these bills expanded Medicaid eligibility during gestation and the first year of life by more than 20 percentage points (Levine and Schanzenbach 2009, 17). The timing of Medicaid expansion varied by state from April 1987 in Arizona to January 1990 in New York. Figure 1 illustrates the month and year each state implemented the expansion.

State Timing of Medicaid Expansion for Pregnant Women and Infants
Source: Authors’ tabulation based on Medicaid expansion dates (Hill 1990).
Note: Dates of state Medicaid expansion with Omnibus Budget Reconciliation Act of 1989 (OBRA 89), which required states to cover pregnant women and children up to age six at 133 percent of the poverty level by April 1990. The optimal way to view the figure is in color. We refer readers of the print edition of this article to https://www.rsfjournal.org/content/9/4/32 to view the color version.
At the same time that states expanded eligibility, they also took multiple steps to simplify Medicaid enrollment and to facilitate access to health care among pregnant women. Table 1 provides an overview of these reforms, which vary across states and include those that primarily reduced burdens either to Medicaid enrollment or to access care.
State Reforms to Increase Medicaid Enrollment and Health-Care Access
Prior to these changes, enrolling in Medicaid and accessing care was more burdensome. Medicaid applications were extremely long, sometimes up to forty-five pages (Hill 1990), and required asset tests in addition to income verification (GAO 1989). Women could generally not apply for Medicaid at prenatal care sites, had to make a separate trip to the county welfare office for an appointment with an eligibility official, and had to provide multiple types of documentation including identification, pay stubs, and bank statements (Hill 1990). Even after applying, waiting for Medicaid applications to be processed could delay prenatal care, and pregnant women could lose coverage during pregnancy because of changes in income or assets or problems recertifying their eligibility (GAO 1989). After enrolling, challenges including transportation, identifying appropriate care providers, and coordinating referrals among them could limit access to prenatal care.
MEDICAID REFORMS TO REDUCE BURDENS TO ENROLLMENT
Several policies aimed to improve Medicaid access, increasing the likelihood that women have insurance throughout their pregnancy. To examine the potential benefits of this group of reforms, we examine the joint effects of removing asset tests, shortened applications, expedited applications, officials at prenatal care sites, and continuous eligibility.
Removing the asset test was made possible when OBRA 86 delinked Medicaid eligibility from AFDC receipt, so that asset restrictions were no longer required (National Governors Association 1990, 3). Asset tests were a primary barrier to Medicaid enrollment and required complex application processes, including detailed documentation and qualified officials to review applications (Hill 1990). Removing the asset test lowered compliance and learning costs by reducing the documentation and information required to apply for Medicaid.
Shortened application forms were also made possible when OBRA 86 delinked Medicaid eligibility from AFDC receipt (National Governors Association 1990, 3). The shorter applications ranged from one page in Vermont and Florida to nine pages in Alabama. Vermont’s single-page application also assessed eligibility for the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC). Individuals who find the Medicaid application long and complicated are more likely to be eligible but not enrolled (Stuber et al. 2000). Shorter forms should reduce learning and compliance costs by reducing the time and difficulty of applying for Medicaid.
Expedited applications for pregnant women gave priority to Medicaid applications for prenatal care (National Governors Association 1990). Some states required applications for prenatal care to be processed within a specific time, such as five to ten days, but such requirements were difficult to enforce (4). Expedited applications are expected to reduce learning and psychological costs by allowing more rapid determination of Medicaid eligibility and more rapid access to care. Expedited and shortened applications should reduce Medicaid application time and difficulty, allowing higher Medicaid enrollment rates and earlier insurance coverage during pregnancy.
Stationing eligibility officials at prenatal care sites allowed states to enroll women without transportation to a social services office and improved experiences of women and eligibility workers (National Governors Association 1990, 3). Eligibility workers were stationed at hospitals, health departments, clinics, and community and migrant health centers. Some states shared the cost of these workers with hospitals or health-care centers; others rotated workers out of social services offices into the field (3–4). Having officials at care sites should reduce learning, compliance, and psychological costs by reducing the time and difficulty of applying for Medicaid and by improving the application experience. This reform should be especially beneficial in conjunction with expedited and shortened applications, which also reduce burdens related to applying for Medicaid.
Continuous eligibility guaranteed continuous coverage during pregnancy to eliminate the risk women could lose Medicaid coverage if family income increased above the eligibility threshold (Hill 1990, 79). State policies generally required Medicaid enrollees to confirm eligibility regularly, such as every month, three months, or six months. Removing these requirements should reduce compliance and psychological costs by allowing continuous enrollment and access to care without having to reenroll or maintain a maximum family income. Studies find that continuous eligibility is associated with more health-care usage and longer insurance coverage among children (Brantley and Ku 2021; DeSisto et al. 2020; Ku, Steinmetz, and Bruen 2013; Swartz et al. 2015). We expect the policy to have similar effects for pregnant women.
Janet Currie and Jeffrey Grogger (2002) do not find that officials at care sites, expedited applications, or shortened applications were significant independent predictors of prenatal care usage. However, the combination of these policies with continuous eligibility and asset test removal may have a stronger effect. Together, asset test removal, shortened applications, expedited applications, officials at care sites, and continuous eligibility should interact to facilitate higher Medicaid enrollment and more continuity in health insurance during the prenatal period. Given that Medicaid is associated with better infant health, reforms that jointly improve access to Medicaid may also improve infant health. Thus, we expect that the combined effects of these reforms will be associated with better infant health outcomes and greater prenatal care use.
Nearly all states removed the asset test and only three states (Delaware, Virginia, and West Virginia) implemented all five of these access reforms. Therefore, we also examine two alternative combinations. First is elimination of the asset test, shortened application forms, continuous eligibility, and officials at care sites with twelve states. Second is elimination of the asset test, continuous eligibility, and officials at care sites with sixteen states (see table 1). Results are generally consistent using these alternative combinations (see online tables A.7 and A.8).1
MEDICAID REFORMS TO REDUCE BURDENS TO CARE
These reforms may enable more women to enroll in Medicaid and for longer periods, but using that coverage to access care requires overcoming another set of administrative burdens. Reforms including presumptive eligibility, coordinated care services, and home care visits may be especially beneficial in improving access to prenatal care. Although transportation cost assistance may also improve access to care, we do not include it in our analyses because only four states adopted this reform and coordinated care services included transportation in most states.
Presumptive eligibility improved access to prenatal care by “allowing primary care providers to approve a simple, short-term, income-related eligibility status” (Hill 1990, 79). Presumed eligibility is expected to reduce learning and compliance costs of prenatal care and therefore increase access to prenatal care. By enabling immediate coverage for prenatal care, presumptive eligibility is associated with increased health-care uptake, including increased prenatal care usage during the first trimester (Piper, Mitchel, and Ray 1994). However, it created administrative complications (such as designation of which providers could determine presumptive eligibility, new forms and cards for women with presumed eligibility) and still required application for full Medicaid eligibility (Hill 1990, 79).
Coordinated care services (CCS) provide case management for pregnant women on Medicaid across care settings, integrating health services from multiple providers into a single care plan. These services included four aspects: needs assessment by identifying risk factors, a plan of care to address those needs, coordinating referrals to appropriate service providers identified by the plan of care, and following up and monitoring whether services are received. Care coordinators also assist with establishing Medicaid eligibility, perform outreach and community education, and assist with arranging transportation (Hill 1990, 84). CCS was enabled by COBRA 1985, the Consolidated Omnibus Budget Reconciliation Act, which allowed states to adopt specialized services for pregnant women without requiring those services for all Medicaid recipients and allowed targeted case management programs for populations requiring extra assistance in accessing services (Hill 1990, 83). Medicaid officials viewed CCS as the “most essential to program success” and described it as “the ‘glue’ holding the perinatal system together” (Hill 1990, 84). Implementation of CCS is associated with increased uptake of prenatal care early in pregnancy (Muoto et al. 2016; Oakley et al. 2017). We expect CCS to increase prenatal care by facilitating access to a range of services to address individual needs.
Home care visits allowed health-care providers to deliver prenatal care in the mother’s home. The rationale was that providers could assess needs and teach healthy behaviors more easily than during office visits (Hill 1990, 86). Home visits could therefore reduce compliance costs by reducing barriers to parental care and by allowing more individualized care. However, home visits could also increase psychological costs if mothers feel that health-care providers judge or look down on their home or neighborhood. Current evidence suggests that home care visits are associated with higher rates of prenatal care use and higher likelihood of receiving adequate prenatal care, based on the Adequacy of Prenatal Care Utilization Index (Meghea et al. 2013). Further, home visits have been found to increase well-child screening and improve clinical outcomes for children with asthma (Campbell et al. 2015; Marshall et al. 2020; Selby-Harrington et al. 1995). These findings suggest that home visits have positive implications for the delivery of health care and for health outcomes.
Transportation costs provided pregnant women with direct financial assistance to cover costs of buses, taxis, and gasoline to travel to prenatal care locations (Hill 1990, 86). This financial assistance only applied if state CCS did not include transportation assistance. Evidence from Georgia and Kentucky suggests that transportation services can improve access to care among Medicaid recipients (Kim, Norton, and Stearns 2009). Covering transportation costs is expected to reduce compliance costs by reducing barriers to access prenatal care.
Given evidence that presumptive eligibility, CCS, and home care visits enable easier access to health care and in some cases improve health, we expect that the combined effects of these three policies will increase prenatal care and improve infant health. Ten states implemented this combination of reforms: Alabama, Arizona, Idaho, Maryland, New Jersey, New York, North Carolina, Pennsylvania, Tennessee, and Utah. Continuous eligibility improved access to both Medicaid and prenatal care and may be particularly valuable for pregnant women by enabling more consistent access to care. Therefore, we examine an alternative reform combination to increase access to care including that reform: continuous eligibility, presumptive eligibility, CCS, and home care visits with nine states (see table 1). Results are generally consistent using this alternative combination (see online tables A.7 and A.8).
States implemented an average of 4.6 in a range of 0 to 7 of these nine policy changes, and only one state (North Dakota) implemented no reforms. Table 1 provides summary information about these reforms, including whether they primarily sought to increase Medicaid enrollment or access to health care, mechanisms (that is, how the policy change should improve enrollment or access), and which types of administrative burden those changes are expected to reduce. Table A.1 specifies policy changes adopted separately by each state. State variation in reforms and their timing allows identification of the effects of these reform combinations for infant health and inequality of infant health.
Based on this review, we examine the following hypotheses:
The combination of reforms to facilitate access to Medicaid increased Medicaid enrollment and infant health.
The combination of reforms to facilitate access to prenatal care increased prenatal care and infant health.
Both reform combinations improved infant health and prenatal care more among mothers with higher risk of administrative burdens (Black, Latina, no college education) than mothers with lower risk of administrative burdens (White, college education).
METHODS
We use state variation in Medicaid reforms and implementation timing from 1987 to 1990 to test whether reforms to reduce administrative barriers to Medicaid or health care influenced Medicaid enrollment, prenatal care, or infant health. We examine effects by maternal race and education to understand implications for inequality of infant health.
DATA
National Vital Statistics System (NVSS) birth data for 1985 through 1994 provide administrative data on infant health and prenatal care by maternal race, ethnicity, education, and state of residence for infants born in the United States from 1985 through 1994. Data from these years include births in all states before and after the 1987–1990 Medicaid expansion for pregnant women and infants. NVSS data provide the most complete and accurate information about births in the United States and include multiple measures of infant health and prenatal care. NVSS birth data have low rates of missing information. For example, in the time period we examine, 0.03 percent of births are missing birth weight measures and 0.11 percent are missing gestational length measures.
We take a 10 percent random sample of births in each year from records for singleton births with information on infant health, prenatal care, and maternal age, race, and education. We use a random sample because statistical inference is not generally applicable to population data (Gibbs, Shafer, and Miles 2017; Berk, Western, and Weiss 1995). We limit the sample to singleton births because infant health measures are often lower for multiple births, the rate of multiple births has increased over time, and the likelihood of multiple births is not randomly distributed (Saavedra 2020; Matthews, MacDorman, and Thoma 2015; Kulkarni et al. 2013; Luke and Martin 2004; Russell et al. 2003). Including births up to sixty months (five years) before and after Medicaid expansion in each state, this results in nearly 2.8 million births in our sample (see descriptive statistics in table A.2).
We link these data to annual state-level information from the Medicaid Statistical Information System (MSIS) to examine Medicaid enrollment and payments. We also link annual state-level data from the Census Bureau, the University of Kentucky Poverty Center’s State Welfare database, and the Current Population Survey to control for population and economic characteristics that may be related to state Medicaid expansion reforms or efforts.
MEASURES
Infant health is measured using birth weight (grams), gestational length (weeks), and indicators for low birth weight (less than 2,500 grams), and preterm birth (before thirty-seven weeks). The thresholds for low birth weight and preterm birth identify infants at high risk for poor health in childhood and later life (Conley, Strully, and Bennett 2003; Johnson and Schoeni 2011; Smedley, Stith, and Nelson 2003). We examine intrauterine growth restriction (less than the 10th percentile of birth weight for gestational age) in sensitivity analyses to allow for downward trends in birth weight over time (Oken et al. 2003).
Prenatal care is measured using indicators for receipt of any prenatal care, receipt of care in the first trimester, length of prenatal care (in months), and number of prenatal visits. We examine multiple measures to allow for potential variation in health-care needs. Reliability and validity are high for infant health measures in the NVSS data but lower for prenatal care measures (Northam and Knapp 2006). This higher measurement error would cause attenuation bias for estimates predicting prenatal care measures.
We examine variation in infant health and prenatal care by maternal education, race, and ethnicity. NVSS data do not include a measure of family income. Maternal education provides a measure of SES that strongly predicts health (Harding, Morris, and Hughes 2015; Montez et al. 2019). We compare infants born to mothers with no college education to those with at least some college education. Given large racial disparities in infant health, we also compare infants born to mothers who identify as White, Black, and Latina. Racial-ethnic categories are mutually exclusive and we refer to White and Black mothers throughout without specifying non-Latina.
Medicaid enrollment and spending are measured for each state and year using annual Medicaid Statistical Information System (MSIS) documents for years 1985–1994 gathered by David Brown, Amanda Kowalski, and Ithai Lurie (2020). From these documents, we extracted state-year data on the number of people enrolled in Medicaid and total payments, adjusted for inflation to 1995 dollars using the Consumer Price Index. We divide these values by the annual number of state residents in poverty. These data are not disaggregated by month, race, or education. We use them to estimate how annual Medicaid enrollment and spending changed with Medicaid expansion and reforms.
State Medicaid enrollment efforts or resources could vary with the state economy (Rodgers and Tedin 2006; Brown and Best 2017), state governance (Soss, Fording, and Schram 2011; Scruggs and Hayes 2017; Brown and Best 2017), state generosity for other programs (Holahan and Liska 1997), and by demographic composition and population size (Holahan and Liska 1997; Alesina, Glaeser, and Sacerdote 2000; Rodgers and Tedin 2006; Preuhs 2007; Soss, Fording, and Schram 2011). Therefore, we control for time-varying measures of state unemployment rate, poverty rate, AFDC benefit for a family of four, an indicator for whether the governor (mayor in the case of Washington, D.C.) is a Democrat, proportion of the population that is Black, proportion Latinx, and population size (logged to reduce skewness). Analyses are conducted with and without these time-varying state controls.
ANALYSIS
We use a difference-in-discontinuities design to compare births before and after Medicaid expansion in states with and without each reform combination (Qureshi and Gangopadhyaya 2021; Lalive 2008; Campa 2011; Leonardi and Pica 2013; Casas-Arce and Saiz 2015). This approach assumes that infants born shortly before or after the expansion are similar except for whether their mothers had expanded access to Medicaid, and other factors related to infant health vary continuously over birth cohort, which is controlled (Lee and Lemieux 2010; Imbens and Lemieux 2008). Comparing effects by state reforms assumes common trends in infant health before expansion and that the local average treatment effect of Medicaid expansion is stable (Qureshi and Gangopadhyaya 2021). In other words, we assume that the effect of Medicaid expansion without each reform combination is stable across states, so that taking the difference isolates the effect of the reforms.
Equation 1 predicts health or prenatal care for each infant (i), in each state of maternal residence (s), and birth month from Medicaid expansion date (t), with an indicator for births after expansion (Postits), indicators for each reform combination to reduce burdens (Medits, Careits) interactions between the combination indicators and birth after expansion (Postits*Medits), indicators for each individual reform (Reforms), month of birth from expansion (Cohortt), fixed effects for each state (μs) and birth year (πt), and controls for male infant, maternal age, and time-varying state economic and demographic measures (Xits). Controlling for a continuous measure of month of birth from Medicaid expansion date addresses potential secular trends in the outcome over time that are unrelated to Medicaid reforms. Models are fit with and without time-varying state-level controls and interactions between post-expansion and each individual reform. Standard errors are adjusted for state-level clustering in all models.
In equation (1), β1 estimates the effect of expanding Medicaid eligibility for pregnant women and infants on birth weight. This coefficient tests whether outcomes differ for infants born in the same state before and after Medicaid expansion and reforms. βm and βk are the coefficients of interest and estimate the additional effect of the combination of reforms to increase access to Medicaid and care. They test whether infant outcomes after expansion differ significantly in states that implemented the package of reforms compared to states that did not implement them. These intent-to-treat estimates compare infants born in the same state shortly before and after Medicaid reforms, adjusting for secular trends. Identification is based on within-state variation across birth cohorts and within-cohort variation across states. Positive βm coefficients when predicting infant health would support hypothesis 1 and positive and βk coefficients when predicting infant health and prenatal care would support hypothesis 2.
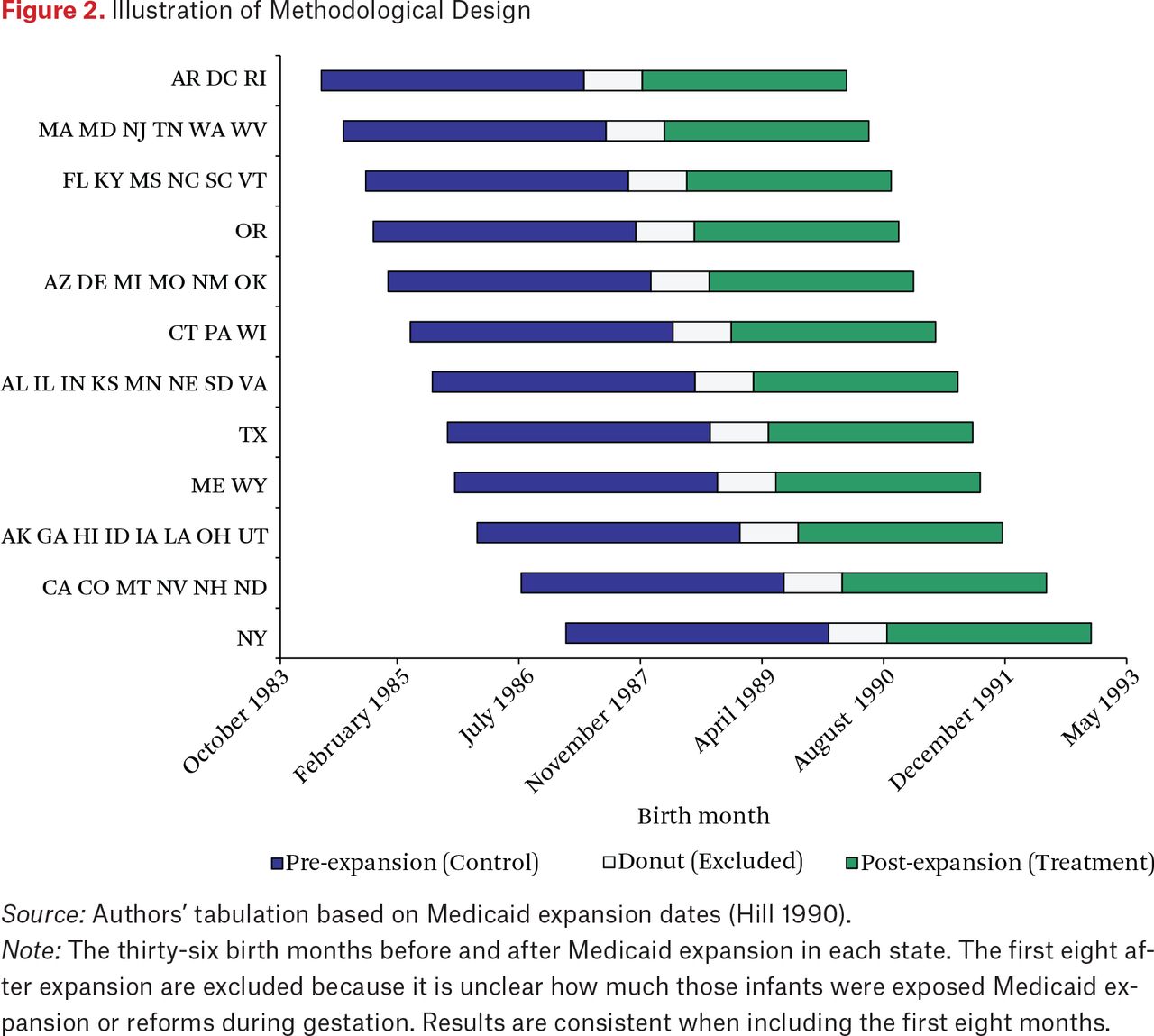
We limit analyses to a consistent window of birth months before and after expansion in each state. Main analyses include a window of forty-eight months (four years) before and after expansion and we vary the width of the window in sensitivity analyses. In main analyses, we exclude the first eight birth months immediately after expansion because it is unclear whether or how much those infants were exposed to the treatment during pregnancy. Figure 2 illustrates this approach. Results are consistent when we include the first eight birth months after expansion.

Illustration of Methodological Design
Source: Authors’ tabulation based on Medicaid expansion dates (Hill 1990).
Note: The thirty-six birth months before and after Medicaid expansion in each state. The first eight after expansion are excluded because it is unclear how much those infants were exposed Medicaid expansion or reforms during gestation. Results are consistent when including the first eight months.
The same model is used to compare effects of Medicaid reforms by maternal education and by race-ethnicity. We test for significant differences in βm and βk coefficients from separate models predicting outcomes by maternal education and race-ethnicity (Clogg et al. 1995). For example, to test for different effects of care access reforms by education, we calculate z statistics  , where βN indicates βk from equation (1) when predicting birth weight among mothers with no college education and βC indicates βk when predicting birth weight among mothers with college. Significantly larger coefficients for mothers with high risk of administrative burdens (Black, Latina, no college education) would support hypothesis 3.
, where βN indicates βk from equation (1) when predicting birth weight among mothers with no college education and βC indicates βk when predicting birth weight among mothers with college. Significantly larger coefficients for mothers with high risk of administrative burdens (Black, Latina, no college education) would support hypothesis 3.
Using annual state-level data, we use a similar model to estimate effects on Medicaid enrollment. Estimates are less precise because we rely on state-year aggregate measures and predict Medicaid enrollment or payments in state (s) in year (t). Positive βm coefficients when predicting enrollment or payments would support hypothesis 1.
SENSITIVITY ANALYSES
We conduct multiple sensitivity analyses to assess the robustness of results to our methodological approach. We repeat the main analyses when including a narrower or wider window of birth months before and after expansion in each state. The width of the window creates a trade-off between internal validity and power. We repeat analyses when including twenty-four, thirty-six, and sixty birth months on each side of the expansion date. Results are consistent with those in the main analyses, which include forty-eight birth months on each side of the expansion date.
We add interactions between the running variable (birth month from expansion) and the treatment indicators for births after Medicaid expansion and the reform combinations. This allows the trends in infant health and prenatal care measures to vary before and after Medicaid expansion. Results are consistent with the main analyses. Effects may differ by the expanded state poverty threshold at which pregnant women are eligible for Medicaid after expansion. We therefore repeat analyses when controlling for the eligibility threshold, interacted with the post-expansion indicator. Results are consistent with the main analyses.
One of the assumptions of our methodological approach is that states with each reform combination had similar trends in infant health before expansion. Figure A.2 shows pre-trends in the rate of low birth weight for each reform. Trends are generally parallel, except for states that allowed expedited eligibility. This supports our approach, but we repeat our analyses when controlling for reform-specific pre-trends to address potential differences. Results, presented in table A.6, are generally consistent with results from the main analyses.
We repeat analyses when limiting the sample to first births for each mother because the benefits of Medicaid reforms may differ by number of previous births. We fit the models with and without including controls and find consistent results. We also repeat analyses when including the first eight birth months after expansion and find consistent results.
MECHANISMS
To understand how Medicaid reforms may have influenced infant health and why effects may vary by maternal race-ethnicity, we conduct two additional sets of analyses. First, we repeat the main analyses when predicting potential mechanisms related to maternal health behaviors during pregnancy, including rates of tobacco and alcohol use, daily cigarettes smoked, and weekly alcoholic drinks consumed. Evidence suggests maternal mental health improves with expanded public benefits, which can reduce stress and coping behaviors (Gennetian and Shafir 2015; Milligan and Stabile 2011; Strully, Rehkopf, and Xuan 2010; Ettinger de Cuba et al. 2019; Oddo and Mabli 2015). Lowering administrative burdens to Medicaid and care could improve infant health by reducing prenatal stress-related coping behaviors, such as alcohol and tobacco use. However, the benefits may be lower for Black and Latina women because of biased treatment by officials or health-care providers (McLemore et al. 2018; Bridges 2011; Davis 2019). Varying effects on these stress-related behaviors could offer suggestive evidence of which groups experienced lower administrative burdens from the reforms. These measures are only available after 1988 and analyses are therefore suggestive, relying on births in fifteen states with expansion dates after 1988.
Second, we repeat the main analyses in states with high and low physicians per capita. Reducing administrative burdens may matter little for infant health or prenatal care in states with a physician shortage. Effects may also vary more by maternal race and education in states with a physician shortage, because White or college-educated mothers can use their resources to access care despite limited physicians. To assess potential varying benefits of reducing administrative burdens, we estimate effects of Medicaid reforms separately in states above and below the 1991 median level of licensed physicians per capita: two physicians per one thousand residents (data from Johnson 2002, 89).
RESULTS
Descriptive statistics for infants born up to five years before or after Medicaid expansion are shown in table A.2. The average infant weighed 3,369 grams (about 7 pounds 7 ounces) and a gestational length of thirty-nine weeks. Rates of low birth weight and preterm birth were low (6 percent and 9 percent, respectively) and 98 percent of infants received prenatal care during gestation, averaging eleven prenatal visits and seven months of prenatal care. The average maternal age was twenty-six years, and about 65 percent of mothers were White, 16 percent Black, and 12 percent Latina.
MEDICAID ENROLLMENT AND SPENDING
Table 2 shows estimates from state-level models predicting enrollment and spending per residents in poverty. Including state and year fixed effects as well as time-varying controls, states that implemented the Medicaid access combination (MAC) of reforms increased Medicaid enrollment rates among those in poverty by about 14 percentage points and increased payments by about $493 per resident in poverty relative to states that did not implement the reforms. These increases represent nearly a half standard deviation increase in Medicaid enrollment rate and nearly a third standard deviation increase payments per resident in poverty. In contrast, the prenatal care access combination (PAC) of reforms had no effect on Medicaid enrollment or spending. These results are consistent with hypothesis 1 and suggest that the MAC reforms increased enrollment.
Regression Estimates Predicting Changes with Medicaid Expansion and Reforms
INFANT HEALTH AND PRENATAL CARE
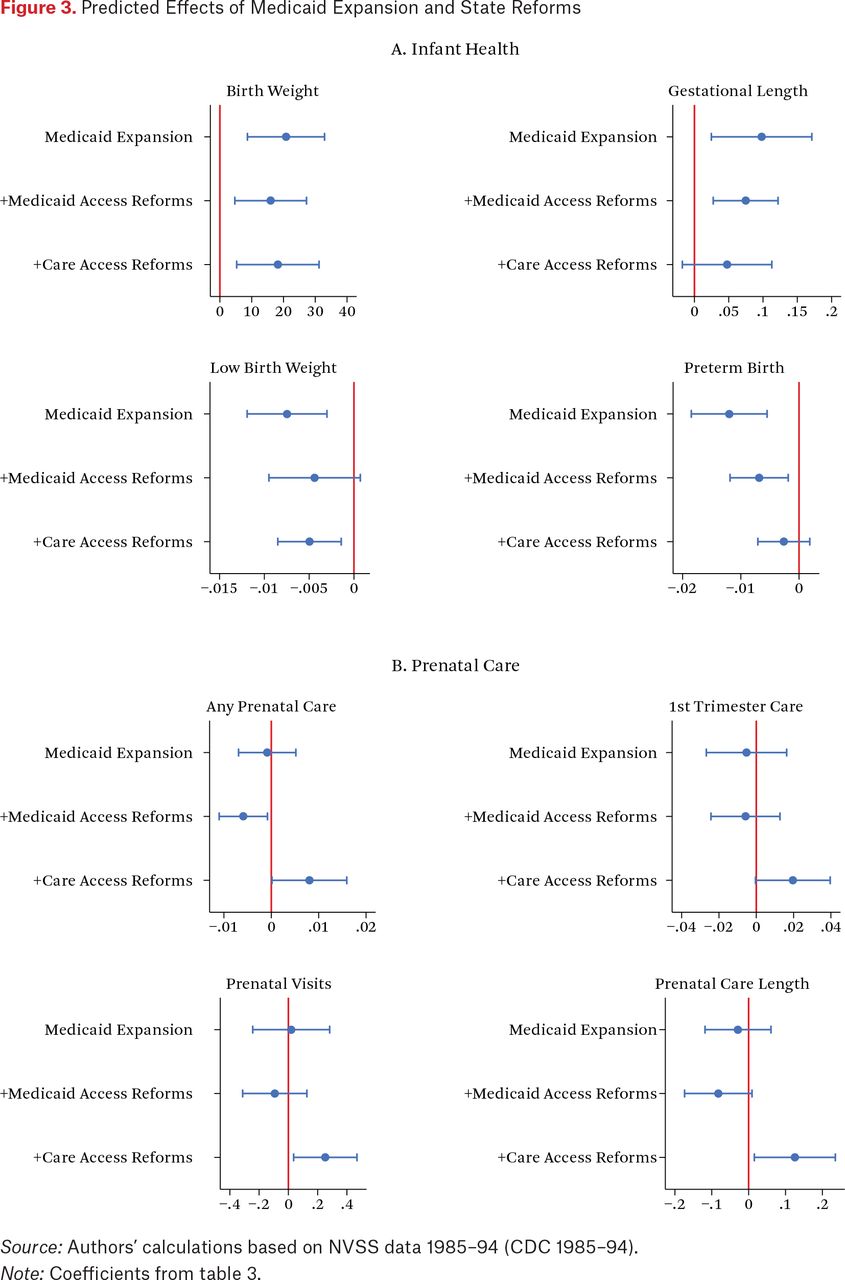
Table 3 shows coefficients for the MAC and PAC reforms when predicting infant health (panel A) and prenatal care (panel B). Consistent with hypothesis 1, mothers living in states that made all five MAC reforms had significantly larger increases in birth weight and gestational length with Medicaid expansion than mothers living in other states. This combination of reforms almost doubled the effect of Medicaid expansion alone on birth weight and gestational length. The likelihood of preterm birth also decreased by an additional half a percentage point in states that adopted all five reforms. Coefficients are shown in figure 3.
Coefficients for Medicaid Expansion and Reform Combinations

The PAC reforms also yielded significant benefits. States that implemented all three reforms had a significantly larger increase in birth weight with Medicaid expansion than other states. The likelihood of low birth weight also declined by an additional 0.5 percent in these states. Coefficients for the PAC reforms are similar in magnitude to those for the MAC reforms when predicting infant health.
Both the MAC and PAC reforms improved infant health. However, only the PAC reforms increased prenatal care receipt. Consistent with hypothesis 2, mothers living in states that made the PAC reforms had significantly larger increases in rates of prenatal care, number of prenatal visits, and length of prenatal care than mothers living in other states. Specifically, the PAC reforms increased the proportion of births receiving prenatal care by nearly 1 percentage point and added an additional quarter of a prenatal visit, on average. These estimates are shown in figure 3.
VARIATION BY RACE, ETHNICITY, AND EDUCATION
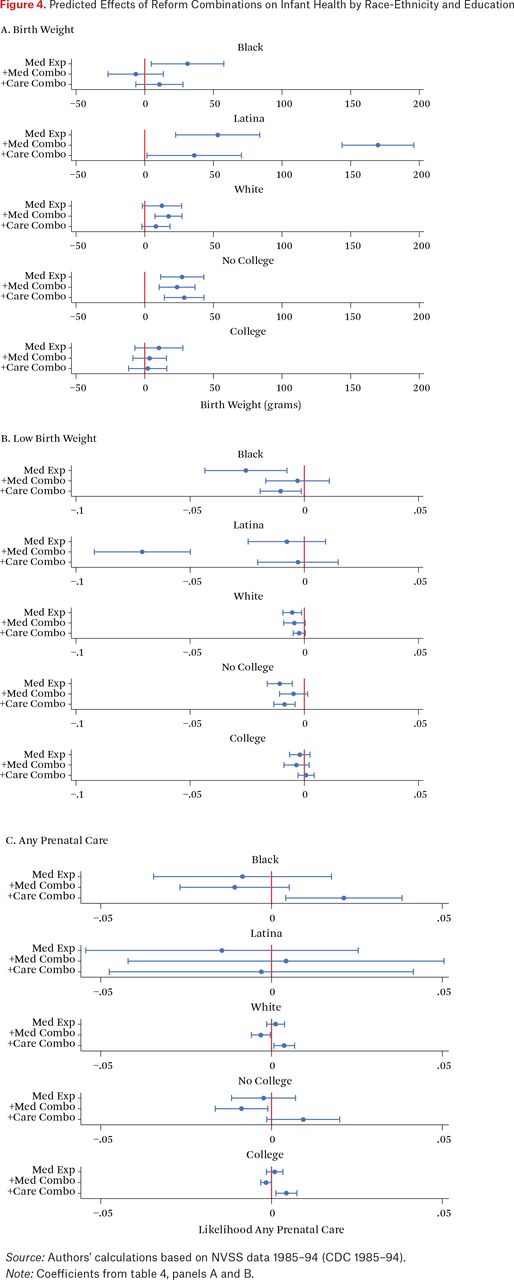
Reforms to facilitate access to Medicaid and care are expected to improve outcomes more for mothers with fewer economic resources given higher eligibility rates and higher risk of administrative burdens before expansion (hypothesis 3). Table 4 shows estimates of the effects of the MAC and PAC reforms by race-ethnicity and by education. The MAC reforms significantly increased birth weight among Latina, White, and non-college-educated mothers. Shown in panel A and illustrated in figure 4, this increase was about 20 grams (two-thirds of an ounce) among White mothers and those without college education, but about 170 grams (one-third of a pound) among Latina mothers. Consistent with hypothesis 3, the benefit of the MAC reforms was significantly larger among Latina mothers and those with no college education than among more highly educated and White mothers. In contrast, the MAC reforms had no effect on birth weight among Black mothers and this estimate differs significantly from the benefit among White mothers.
Coefficients for Medicaid Expansion and Reform Combinations by Race and Education

Results are consistent when predicting gestational length and the likelihood of preterm birth. The MAC reforms reduced the likelihood of preterm birth by about 1 percentage point among White mothers, but by nearly 8 percentage points among Latina mothers. For all infant health outcomes, the benefit of the MAC reforms was significantly larger among Latina mothers than among White mothers, which is consistent with hypothesis 3. The MAC reforms also improved infant health outcomes among mothers with no college, but did not among Black mothers.
The PAC reforms also had varying effects by maternal race-ethnicity and education. Consistent with hypothesis 3, these reforms increased birth weight by 29 grams (1 ounce) and reduced the likelihood of low birth weight by nearly 1 percentage point among mothers with no college education, significantly more than among mothers with college (table 4, panel A). The PAC reforms had some benefits among Black women, reducing the likelihood of low birth weight by 1 percentage point and increasing the length of prenatal care by about one week. The PAC reforms, however, increased the likelihood of receiving prenatal care by 2 percentage points among Black women, significantly more than among White women. Thus, although the Medicaid access reforms had little benefit for Black women, the prenatal care access reforms did provide them significant improvements in prenatal care and likelihood of low birth weight.
These results complicate earlier evidence of the weak relationship between prenatal care and infant health for Black women (Sonchak 2015; Thurston, Fields, and White 2021). Substantial administrative barriers to prenatal care could limit benefits for Black women. For example, difficulties organizing transportation or medical referrals could be more difficult and stressful for Black women if they are more likely to feel dismissed by providers or live in areas with fewer providers who accept Medicaid (Daly and Mellor 2020; Greene, Blustein, and Weitzman. 2006; Lillie-Blanton, Martinez, and Salganicoff 2001; Roman et al. 2017). The PAC reforms could be particularly valuable in overcoming these additional burdens for Black women. In contrast, the limited benefits of the MAC reforms for Black women could reflect persistent barriers to Medicaid enrollment such as anti-Black racism from enrollment officials (Michener 2018), greater misinformation (learning costs) about Medicaid program rules (Stuber and Bradley 2005), or higher experience of stigma (psychological costs) among Black Americans related to participation in government programs (Stuber and Schlesinger 2006). Thus, unless reforms directly target these unequal barriers to Medicaid enrollment, results suggest reforms facilitating access to prenatal care may yield larger benefits for Black women.
Results for Latina women suggest a different pattern. Lower barriers to Medicaid enrollment were particularly beneficial for infant health and reforms to ease access to care did not increase prenatal care receipt. This could reflect differences in the quality rather than the amount of prenatal care. For example, Latina women have the lowest rates of health insurance coverage (National Partnership for Women and Families 2019), report lower-quality prenatal care (Dayton et al. 2006; Becker and Tsui 2008), and official verification of eligibility for care can improve the quality of care mothers receive (Lillie-Blanton and Hoffman 2005; Bernstein, Chollet, and Peterson 2010). Thus the Medicaid reforms may improve infant health by increasing access to care among Black mothers but do so by increasing the quality of care among Latina mothers.
MECHANISMS
To help understand varying effects of the reforms, we examine stress-related coping behaviors and access to physicians as potential mechanisms. Estimates predicting maternal behaviors during pregnancy are shown in table A.3. Alcohol and tobacco use declined after Medicaid expansion for nearly all groups. However, the MAC reforms reduced alcohol and tobacco use during pregnancy significantly more among Black mothers than among White mothers. The MAC reforms also reduced tobacco use significantly more among mothers without college than among those with a college education. These estimates suggest facilitating access to Medicaid can reduce stress-related coping behaviors, particularly for those at higher risk of administrative burdens. These benefits could reflect lower stress from reduced administrative burdens or from gaining health insurance. The PAC reforms reduced tobacco use more among Black mothers than White mothers and reduced alcohol use more among mothers without than with college education. These reforms were implemented after the public health campaign to reduce smoking among pregnant women and could reflect exposure to health-care providers encouraging pregnant women not to smoke.
Smaller infant health benefits of the MAC reforms among Black women could lead one to expect smaller effects on health behaviors among Black women. However, results contradict that explanation for weaker benefits. Rather, the MAC reforms reduced stress-related coping behaviors more among Black women than among White women.
Results of the main analyses suggest the PAC reforms increased receipt of prenatal care, but these benefits could depend on the availability of doctors. Tables A.4 and A.5 show estimates predicting infant health and prenatal care separately in states above and below the 1991 median level of licensed physicians per capita. Among births to all mothers (table A.4), the combination of reforms to increase access to care had significantly larger benefits on infant health and prenatal care in states with high numbers of physicians per capita. Effects of the MAC reforms did not differ significantly by physicians per capita. When examining effects by race and education (table A.5), the PAC reforms have significantly larger birth weight benefits for all groups in states with high doctors per capita. The birth weight benefits of PAC reforms were particularly large for Black, Latina, and less-educated mothers in states with more doctors. Prenatal care benefits of the PAC reforms were also significantly larger for these mothers in states with more doctors.
Results suggest the PAC reform effects are larger in states with more doctors. The MAC reform effects are larger in states with more doctors, but only among White mothers. This may reflect advantages among White women in accessing doctors when more people gain access to Medicaid. In states with a shortage of physicians, these advantages may yield no benefit and everyone may face large burdens to accessing doctors.
CONCLUSION
In the late 1980s, states implemented multiple reforms with Medicaid expansion to reduce administrative burdens to access Medicaid and prenatal care. We use administrative birth data from the National Vital Statistics System to examine effects of these reforms on infant health and prenatal care. Using a difference-in-discontinuities approach, we find that a combination of reforms to facilitate access to Medicaid increased state Medicaid enrollment among those in poverty by about 14 percentage points. Medicaid expansion improved infant health, reducing rates of preterm birth and low birth weight by around 1 percentage point. Reform packages to facilitate access to Medicaid and prenatal care enhanced these benefits for infant health, reducing the likelihood of low birth weight or preterm birth by another 0.5 percentage point. Reducing administrative burdens to enroll in Medicaid and access prenatal care yields infant health benefits almost as large as expanding Medicaid eligibility.
Consistent with previous evidence (Currie and Grogger 2002), we find that individual reforms to reduce administrative burdens generally had little added benefit over Medicaid expansion for infant health or prenatal care. Instead, combined reforms to reduce burdens in multiple ways significantly improved infant health. Similar to the benefits of multiple income support policies for low-income families (Edelstein, Pergamit, and Ratcliffe 2014; Schmidt, Shore-Sheppard, and Watson 2016; Slack et al. 2014), our results suggest benefits of multiple reforms to reduce administrative burdens.
The benefits of Medicaid reforms varied by maternal race, ethnicity, and education. In most cases, reform combinations improved infant health more among mothers with higher risk of administrative burdens. For example, reform combinations had larger health benefits for births to Latina and non-college-educated mothers relative to White and college-educated mothers. Black women are also at higher risk of burdens and the prenatal care access reforms yielded significant improvements in their likelihood of prenatal care and low birth weight. These results suggest that administrative barriers to care may be higher for Black women and removing them may be particularly valuable for Black women and infants. At the same time, Medicaid access reforms reduced prenatal alcohol and tobacco use more among Black women than White women, but had little effect on infant health or prenatal care for Black women. These results suggest persistent barriers, such as anti-Black racism among Medicaid officials (Michener 2018) or stigma related to participation in government programs (Stuber and Schlesinger 2006), that remain higher for Black women despite reforms. Future reforms should target these persistent barriers for Black women.
Overall, the variation by race and ethnicity suggest a different pattern of administrative burdens, with higher barriers to Medicaid enrollment and quality care among Latina women and higher barriers to access prenatal care among Black women. Our results suggest the Medicaid reforms may have improved infant health in different ways: by increasing access to care among Black mothers and by increasing the quality of care among Latina mothers. These complex results underline the importance of an intersectional approach to understanding administrative burdens and health-care experiences (Crenshaw 1989; Michener and Brower 2020).
Reforms facilitating access to prenatal care had larger benefits in states with high physicians per capita, particularly among Black mothers and mothers with no college education. We find weak benefits in states with few physicians, echoing previous evidence that reforms can yield limited or even counterintuitive effects if systems are not adequately prepared (Wishner and Burton 2017; Dugan and Booshehri 2021; Rauscher 2016). Because easing access to prenatal care had larger benefits among Black women, particularly in states with more doctors, increasing the number of physicians in areas with a high concentration of Black women could be another way of reducing barriers and increasing equality of health for Black women and infants.
This study has important limitations. Our estimates of Medicaid enrollment rely on state-level data. Future research using monthly data disaggregated by race and socioeconomic status would provide more conclusive estimates. Our results also depend on several assumptions, which are difficult to assess. Although the Medicaid expansion was exogenous (federally mandated), an important limitation is that the reforms could reflect unobserved state characteristics and the limited number of states and policy combinations presents identification challenges (Blank 2002; Bitler, Gelbach, and Hoynes 2005). We take steps to assess robustness, including examining alternative reform combinations and controlling for time-varying state characteristics.
Reassuringly, states with each reform generally had similar trends in infant health before Medicaid expansion (figure A.2) and results are consistent when controlling for pre-trends in states implementing the reform combinations. Our approach also assumes stable effects of Medicaid expansion (without reforms) across states and that unobserved differences in individual births vary consistently across birth months. State variation in the timing of reforms helps reduce the likelihood that some other policy or nationwide change influenced infant health at the same time. Further, results are consistent in additional sensitivity checks, including varying the number of birth months included before and after expansion, allowing trends in infant health and prenatal care to vary before and after Medicaid expansion, limiting the sample to the first birth for each mother, and estimating effects with and without including controls.
Overall, our results suggest that implementing multiple Medicaid reforms to reduce administrative burdens improved infant health and prenatal care usage, especially for those at greater risk of experience administrative burdens. However, varying effects by race and ethnicity suggest that the reforms mattered in different ways for Black and Latina mothers because of the different patterns of barriers they each faced. Our results raise questions about why particular types of reforms are more beneficial for certain groups of mothers than others. Qualitative data that examine the particular learning, compliance, and psychological costs of participating in public programs faced by Black and Latina mothers with varying levels of socioeconomic resources, including education, would be valuable in efforts to improve equality of infant health.
Findings from this study have several implications. First, administrative burdens are a substantial barrier to accessing health insurance and health care during pregnancy, especially among racially and socioeconomically marginalized mothers. Second, multiple approaches to improve access to Medicaid and prenatal care by alleviating administrative burden are beneficial. Because social factors interact to create unequal administrative burdens (Michener and Brower 2020), addressing those burdens requires combined policy responses that interact to reduce multiple burdens at the same time. Third, targeted reforms to address particular types of burdens that are higher among Black and Latina mothers could enhance benefits of public health insurance and improve equality of infant health.
FOOTNOTES
↵1. See the online appendix at https://www.rsfjournal.org/content/9/4/32/tab-supplemental.
- © 2023 Russell Sage Foundation. Rauscher, Emily, and Ailish Burns. 2023. “State Approaches to Simplify Medicaid Eligibility and Implications for Inequality of Infant Health.” RSF: The Russell Sage Foundation Journal of the Social Sciences 9(4): 32–60. DOI: 10.7758/RSF.2023.9.4.02. The authors are grateful for feedback from colleagues at the Annenberg Institute for School Reform, the Russell Sage Foundation, and journal editors. This research was supported by the Population Studies and Training Center at Brown University, which receives funding from the NIH for general support (P2C HD041020) and training (T32 HD007338). Direct correspondence to: Emily Rauscher, at emily_rauscher{at}brown.edu, Brown University Box 1916, Providence, RI 02912, United States
Open Access Policy: RSF: The Russell Sage Foundation Journal of the Social Sciences is an open access journal. This article is published under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- THEORETICAL BACKGROUND
- POLICY EFFECTS ON INEQUALITY AND INFANT HEALTH
- POLICY BACKGROUND
- MEDICAID REFORMS TO REDUCE BURDENS TO ENROLLMENT
- MEDICAID REFORMS TO REDUCE BURDENS TO CARE
- METHODS
- DATA
- MEASURES
- ANALYSIS
- SENSITIVITY ANALYSES
- MECHANISMS
- RESULTS
- MEDICAID ENROLLMENT AND SPENDING
- INFANT HEALTH AND PRENATAL CARE
- VARIATION BY RACE, ETHNICITY, AND EDUCATION
- MECHANISMS
- CONCLUSION
- FOOTNOTES
- REFERENCES
- Figures & Data
- Additional
- Info & Metrics
- References
Related Articles
Cited By...
- No citing articles found.