
Abstract
Rising poverty in suburbs has led to increased interest in how well suburban safety nets function. Apart from public assistance programs, community-based nonprofit health and human service organizations play a central role in suburban efforts to address racial and economic inequalities. Understanding how nonprofit services are distributed across the suburban and urban landscape, therefore, is critical to assessing how communities may be able to address need. In this paper, we examine the presence and volatility of nonprofit health and human service expenditures in suburban and urban counties across the United States from 2000 to 2017. We find the nonprofit safety net to be more responsive in urban centers than in suburban places, and less robust in suburban areas experiencing high rates of poverty or with a larger share of residents who are Black. Nonprofit health and human service spending also appears less countercyclical than is commonly understood. Suburban-urban disparities in nonprofit health and human service spending persist after controlling for several county-level demographic and socioeconomic factors.
Poverty in U.S. suburbs surged to historic highs in the early part of the twenty-first century. Although poverty was on the rise in many suburban areas during the 1990s, the recession of 2001 and the Great Recession that ended in 2009 led to dramatic increases in the number of poor people living in suburbs (Berube and Kneebone 2013). Scott Allard (2017) finds that suburbs in the largest hundred metropolitan areas were home to nearly as many poor people in 1990 as cities in those same metros—8.6 million versus 9.5 million. By 2012, nearly seventeen million poor people lived in the same suburban census tracts relative to 12.7 million in urban tracts. Economic recovery following the Great Recession reduced the number of Americans in poverty, but roughly four million more poor people lived in the suburbs of the largest hundred metro areas in 2017 than in the cities themselves (Allard and Pelletier 2021). Geographically sensitive data available around the COVID-19 pandemic provides little evidence that the pandemic recession altered the spatial distribution of poverty (Allard and Pelletier 2021; Shrider et al. 2021). Poverty problems in urban centers have not diminished over the last thirty years and poverty rates remain much higher in cities than in suburbs, but the plurality of poor Americans continue to live in the suburbs of American cities.
More than just an interesting demographic trend, the changing nature of poverty across the suburban landscape poses urgent challenges to the U.S. antipoverty safety net. Although a more robust set of publicly and privately funded safety net programs are in place today than thirty years ago, capacity to help low-income families can vary widely from community to community. Of particular concern is variation in the capacity of community-based nonprofit health and human service organizations resting at the core of the modern American safety net—including community health centers, housing services, employment services, and emergency assistance providers. Nonprofit human service organizations deliver many different programs intended to reduce hardship, improve well-being, and increase mobility. Provision of nonprofit services in suburban communities, however, has been shown to trail the capacity in urban areas (Berube and Kneebone 2013; Allard 2017).
Despite emerging interest in suburban poverty and recognition that nonprofit human service capacity lags in suburban areas, little inquiry has been made into how provision of nonprofit health and human services in suburban communities has changed over time, or how changing demographic and economic context may be associated with those changes. To provide more insight into temporal variation in nonprofit health and human service provision across the suburban versus urban landscape, this article focuses on two core research questions: How does the level and volatility of provision of nonprofit health and human services vary between suburban and urban communities over time? Do observed differences in nonprofit health and human service provision vary by the racial composition and economic context of a community?
To answer these questions, we examine urban-suburban differences in nonprofit health and human service provision across metropolitan America from 2000 to 2017.1 In addition to drawing attention to the disparities in nonprofit service provision between urban and suburban areas, descriptive findings highlight substantial volatility among suburban nonprofit service providers. Analyses focus on the gaps in access to nonprofit services in high-poverty and racially diverse suburban areas.
SUBURBAN (AND URBAN) NONPROFIT HEALTH AND HUMAN SERVICE SAFETY NETS
Community-based nonprofit health and human service programs, for simplicity often referred to as nonprofit human service programs, are a critical component of the antipoverty safety net.2 Nonprofit health and human service organizations are defined here to be legally incorporated, tax-exempt entities providing social assistance to low-income or otherwise marginalized communities through three main categories of services: public and behavioral health, social, and child and family. These types of organizations range from large human service providers such as YMCAs or Boys & Girls Clubs to smaller organizations such as local food pantries or family resource centers. We analyze organizations providing a wide range of services, including substance abuse prevention and treatment, employment and vocational services, adult education programs, transportation assistance, food and housing supports, preschool and daycare, and youth activities and mentorship. Such services complement public cash and in-kind programs of assistance, such as Supplemental Nutrition Assistance Program (SNAP) and the Earned Income Tax Credit (EITC), by filling needs that public assistance programs do not cover and reaching low-income populations not eligible for public benefits.
Funding for nonprofit human service programs often comes from federal and state governments through competitive grants and contracts, provision of direct goods or food commodities, Medicaid insurance reimbursement, and voucher payments (see Allard and Smith 2014). In addition to public funding streams, service providers also commonly draw on private sources of revenue, such as private giving or service fees, to complement public funding within operational budgets. Nonprofit health and human service expenditures exceed $100 billion annually, which reflects the central role that publicly financed, but privately and locally administered, nonprofit human services play in the American antipoverty safety net (Allard 2009, 2017).
Rather than operating as a single consistent entity across the country, therefore, the nonprofit health and human service sector is inherently local. Researchers find evidence that the services available to low-income households vary widely from place to place and over time within a given place (Allard 2009; Murphy and Wallace 2010). Spatial and temporal variation in nonprofit human service provision reflects how those programs are funded. Public and private nonprofit service funding fluctuates substantially from place to place, reflecting local variation in wealth, tax base, support for public intervention, and the strength of charitable philanthropy (Allard 2009, 2017; Berube and Kneebone 2013). Unlike some public assistance programs, such as SNAP or the EITC, that expand when need rises, many public and private funding streams for nonprofit human service programs often do not automatically expand during times of need in that economic downturns typically correspond with fewer public resources and dampened private giving (Allard 2009). Complicating matters, local communities grapple with competitive pressures that can depress local safety net responses. Scholars typically argue local places will underprovide or choose not to provide any type of safety net assistance with own-source revenues due to local concerns that those programs will attract low-income families and place greater burden on local budgets (Downs 1997; Peterson 1981; Tiebout 1956). As a result, nonprofit human service programs appear only sluggishly responsive to rising need (Allard 2009, 2017; Allard and Pelletier 2021).
Scholarship leads us to expect provision of nonprofit human services to vary with the racial and ethnic composition of local communities. Historically, the decentralized antipoverty safety net in the United States allowed local places to treat communities of color differently and to restrict access to programs of assistance (Lieberman 1998; Soss, Fording, and Schram 2011). Racial and ethnic segregation in the United States corresponds to lower quality schools, public amenities, housing, and employment opportunities (see Galster and Sharkey 2017). Racial stereotypes about the poor and notions of deservingness undermine public and private commitments to the provision of antipoverty safety net assistance (Gilens 1999; Johnson 2003; Soss, Fording, and Schram 2011). This may manifest in funding decisions; evidence indicates, for example, that government funding of nonprofit organizations is less responsive to local need in neighborhoods with a larger share of Black residents (Garrow 2014). Similarly, service providers may choose not to locate in or near areas with large concentrations of racial and ethnic minorities due to concerns about quality office space, staff retention, and proximity to philanthropic partners (Allard 2008, 2009). Evidence also indicates that local places may underprovide human services to ethnic immigrant communities (Allard and Roth 2010; Roth, Gonzales, and Lesniewski 2015), particularly places that have become immigrant destinations in recent years (Everitt and Levinson 2016; Roth and Grace 2018). Consistent with these expectations, research finds evidence that communities of color have less access to nonprofit human services than predominantly White communities (Allard 2008, 2009; Roth and Allard 2016) and that providers located in communities of color experience more volatile funding than those in predominantly White places (Allard 2009).
As poverty has increased in suburban America, the adequacy and stability of nonprofit health and human service programs operating in suburban communities has been called into question (Allard 2017; Lewis-McCoy et al. 2023, this issue). Central cities have been the focal point of most public safety net program spending and antipoverty policy for most of the last sixty years, which policy has been the catalyst for growth of the nonprofit human service sector in urban centers. Suburban areas, however, remain home to far fewer nonprofit organizations and less robust local public or charitable philanthropic support for human service programs. Limited awareness of suburban poverty problems means that the suburban nonprofit sector receives less attention than urban nonprofit organizations. Organizations also face challenges in operating fragmented human service delivery systems across large and complex suburban regions (Allard 2017). Underscoring these realities, recent research finds that nonprofit service providers in large urban counties in 2017 spent roughly twice as much per poor person on a broad array of human service programs, on average, then providers in suburban counties (Allard and Pelletier 2021).
Spatial variation in the presence and volatility of nonprofit human service programming may have a number of downstream consequences relevant to the well-being of low-income households. First, greater service accessibility within a given local place should affect the costs and burdens associated with seeking assistance. Lower commuting costs for eligible households make it easier to visit offices with application questions, necessary documentation, and eligibility recertification, which should translate into a higher likelihood that an eligible household receives assistance (Allard, Wathen, and Danziger 2021; Martin et al. 2003; Morrissey, Allard, and Pelletier 2022). We expect closer proximity to nonprofit health and human service programs will increase exposure to information about and referrals for various programs of support available locally, which should then translate into higher take-up rates of assistance (Allard 2009, 2017; Allard, Tolman, and Rosen 2003). Less access may have channel effects that amplify household ambivalence or concern about stigma that then increases hesitation to seek assistance (Allard, Wathen, and Danziger 2021; Mabli and Worthington 2017). Less reliable or consistent nonprofit human service program funding and provision within a given local place should compromise the stability of the sector, creating even greater barriers to participation and take-up.
Emerging evidence indicates that suburban communities lag urban centers in nonprofit service program capacity and that the nonprofit service sector overall may be less responsive to need than is understood, yet relatively little research examines how nonprofit service provision varies across suburban communities or how provision varies within suburban communities over time. To better understand the spatial and temporal contours of suburban nonprofit health and human service safety nets, we therefore pose two core research questions: How does the level and volatility of provision of nonprofit health and human services vary between suburban and urban communities over time? Do observed differences in nonprofit health and human service provision vary by the racial composition and economic context of a community? Greater understanding of suburban nonprofit safety nets will not only strengthen scholarly understandings of the devolved and decentralized American antipoverty safety net, but also help inform future public policy and strategic philanthropic investments intended to reduce poverty.
DATA AND METHODS
To address these questions, this article analyzes a unique county-level data set tracing nonprofit health and human service expenditures across urban and suburban areas from 2000 to 2017. To these nonprofit expenditure data, we link county-level economic and demographic data, including information about racial and ethnic composition of the population, total population in poverty, poverty rates, educational attainment, and political context. Combined, these data provide insight into how nonprofit service provision varies across urban and suburban areas over a two-decade span that saw significant economic and demographic change.
We define urban and suburban counties following Office of Management and Budget (OMB) definitions of metropolitan area boundaries and primary urban centers (U.S. Department of Agriculture 2013). Urban counties are defined as those containing the primary urban center of a given metropolitan area and suburban counties are those counties that are defined as part of the same metropolitan area, but do not contain the metro’s primary city. Large urban counties are defined as those within the largest one hundred metropolitan areas and small as those located in metropolitan areas outside the largest hundred. Small urban counties have fewer than five hundred thousand residents generally and small suburban populations, whereas large urban counties are home to about 75 percent of the U.S. population and include the vast majority of suburban residents. Tract-level data then is used to sort large urban counties into three categories: less than one-third of the county population in suburban municipalities; one-third to two-thirds; or more than two-thirds.3
Our approach here is useful for addressing questions about nonprofit service provision. First, counties are key administrative units for public assistance programs and are common geographic boundaries for nonprofit human service program catchment areas. Institutional charitable philanthropy supporting nonprofit human services often is bounded within a given county or set of counties in a region. More practically, it is difficult to get information about nonprofit expenditures at levels of geography below the county, such as at the municipal or neighborhood level. Our operationalization of urban and suburban geography is quite similar to other articles in this issue that examine national data (see Lichter, Thiede, and Brooks 2023; Rastogi and Jones-Correa 2023, this issue; Rutan, Hepburn, and Desmond 2023). Similarly, articles in this issue that focus on suburban case studies define those suburban locations in consistent alignment with our approach (see Clergé 2023; Frankenburg et al. 2023, this issue; Simms 2023, this issue; Zapatka and Tran 2023).
We use data from the 2000 Census and American Community Survey (ACS) 5-year estimates from 2005–2009 through 2015–2019 to compare urban and suburban counties with different demographic characteristics (U.S. Census Bureau 2021a, 2021b). We report descriptive results separately for counties with a high poverty rate (20 percent or more of the population has income below the federal poverty line) and a low poverty rate (less than 20 percent of the population is in poverty). We also group counties by the racial and ethnic composition of their populations. A county is considered to have a low percentage Hispanic or Black population if the share of the county’s population identifying as Hispanic or Black is more than half a standard deviation below the mean for urban or suburban counties in a given year. Similarly, we categorize a county as having a high percentage Hispanic or Black population if the population share for that group is more than half a standard deviation above the mean for urban or suburban counties in that year.4 The online technical appendix provides more detail about how we constructed these measures, and reports descriptive statistics about poverty and the racial composition of urban and suburban counties.
In regression analyses, we control for the share of the adult population in a county that has a college degree or higher, using data from ACS 5-year estimates between 2005–2009 and 2015–19. For each year of nonprofit expenditure data, we merge in the ACS 5-year window with a midpoint matching that year. For example, for the year 2007, we use ACS 2005–2009 5-year estimates. College degree holders are defined as those with associate’s, bachelor’s, professional, or doctoral degrees.
We also control for county political context by including the percentage of voters who voted for the Republican candidate in the presidential election closest to that year (MIT Election Data and Science Lab 2018). In the case of a year halfway between two presidential elections, we use the earlier presidential election results (for example, for 2010, we use the Republican vote share from 2008).
We use nonprofit health and human service organization expenditure data from the National Center for Charitable Statistics (NCCS) for the years 2000 to 2017 to create county-level measures of nonprofit health and human service provision (National Center for Charitable Statistics 2021). We aggregate nonprofit health and human service organization-level expenditures reported in the NCCS across three broad service categories. Public and behavioral health services encompass public health promotion organizations, substance abuse prevention and treatment organizations such as rehab centers, and residential- and nonresidential mental health service providers such as community counseling centers. Social services include adult education organizations, employment counseling and training groups, food banks and soup kitchens, housing assistance organizations and homeless shelters, and human service providers such as neighborhood centers, American Red Cross or Salvation Army chapters, or organizations that provide transportation or financial counseling. Finally, child and family services include preschool and daycare centers, organizations such as Boys & Girls Clubs that provide recreational and social activities for children, and human service organizations specifically aimed at families with children.5 Descriptive analyses examine county-level trends in nonprofit service expenditures using four primary measures: total expenditures; expenditures per poor person; arc percentage change in total expenditures; and arc percentage change in expenditures per poor person. Given nonprofit expenditures in two consecutive years Ey–1 and Ey, the arc percentage change is:
Measures of change will examine year-to-year changes, as well as changes over longer intervals of time between 2000 and 2017.
Although useful for assessing broad patterns in the national nonprofit sector, data from the NCCS have a few limitations relevant to the study of place and human service provision. NCCS data reflect only nonprofit organizations that submit Internal Revenue Service (IRS) 990 forms verifying tax-exempt status. Many small nonprofits and religious congregations do not file such forms and are thus not present in the data.7 In addition, nonprofit data from the IRS contain location information only for an organization’s administrative headquarters, not separate subsidiary offices where services may be delivered. IRS data, therefore, may not capture the true geographic reach of many large human service nonprofits that are headquartered in a central city or population center, but operate programs in rural regions or suburban communities. Despite these limits, IRS 990 data remains the most consistent source of information about nonprofit human service provision at the local level.
We have shaped our measures and analyses in several ways to account for these structural features of the NCCS data. First, we aggregate data from individual organizations to the county level. Counties often are the geographic jurisdiction that bound nonprofit service activities, so aggregating to the county-level should provide as accurate a relative impression about the capacity of local nonprofit human service organizations as is possible with available data. Second, in addition to reporting measures for all nonprofit organizations, we also report county-level expenditure measures for nonprofits with annual revenues of less than $10 million, which should exclude extremely large national or regional administrative headquarters that would distort expenditure totals. Even with these modifications, the limitations of the NCCS data have important implications for our analysis. When we analyze nonprofit spending in a certain type of county, those figures reflect service provision by all organizations with their headquarters located in that type of county. This may lead to some underreporting of service provision in suburban areas, as we expect some urban-based providers to provide programming in nearby suburban counties. We are cautious in our interpretations of results accordingly. Nevertheless, we believe that the findings discussed here present valuable conceptual and practical insights into the realities confronting local safety nets in suburban and urban America.
FINDINGS
Table 1 presents aggregate sums of health and human service expenditures across all nonprofits and those with annual revenue under $10 million. Compiling across the columns of table 1, health and human service nonprofits across all metropolitan areas reported over $111 billion in expenditures in 2017, an increase of more than two-thirds from roughly $68 billion in 2000 (see table 1, top panel, third row). Nonprofit service organizations with revenues under $10 million annually reported $30.2 billion in total expenditures in 2017, up from $25.4 billion in 2000 (increase of 19 percent, see table 1, bottom panel, third row). Combined, these figures underscore the key role that nonprofit organizations—large and small—play in the safety net today.
Nonprofit Health and Human Service Expenditures Across Urban and Suburban Counties, 2000–2017
As we would expect from prior research, health and human service nonprofit organizations are highly concentrated in urban counties. Nonprofit service providers in urban counties reported nearly $88.7 billion dollars in expenditures in 2017 relative to $22.8 billion in suburban counties (see table 1, top panel, third row). Roughly four of every five dollars in nonprofit health and human service spending is centered in urban counties today, as has been the case for the last two decades. Similar trends are apparent when looking at smaller nonprofits in the bottom panel of table 1. Rates of growth in nonprofit human service expenditures were comparable between urban and suburban areas from 2000 to 2017. For example, total nonprofit service expenditures increased by 52.5 percent in the least suburbanized urban counties located in the hundred largest metro areas (see table 1, top panel, column 1), while total nonprofit expenditures increased by 62.3 percent in suburban counties (see column 4). Evidence, however, indicates that nonprofit human service funding in both urban and suburban counties had slower rates of growth in the wake of the Great Recession than in the decade prior. For example, whereas total expenditures increased by about 60 percent in suburban counties from 2000 to 2010, expenditures in these counties barely changed between 2010 to 2017, rising only 3 percent. Similar trends are present in urban counties overall, where expenditures grew 53.6 percent from 2000 to 2010 but by only 6.7 percent from 2010 to 2017. These figures underscore the impact of the Great Recession on public and private funding of community-based nonprofit organizations, but also indicate that the spatial distribution of nonprofit human service expenditures has not shifted appreciably over the past twenty years.
Aggregate nonprofit expenditures mask important trends within the health and human service sector. Table 1 and figure 1, therefore, also trace total nonprofit health and human service spending on public and behavioral health services, social services, and child and family services across urban and suburban county geography. Human service spending grew at a faster rate than public and behavioral health services or child and family services across urban and suburban counties when looking at all nonprofit organizations. A similar but subtle trend is evident in looking at smaller nonprofit service organizations in the bottom panel of table 1 and panel B of figure 1. Spending among public and behavioral health nonprofits with revenues under $10 million declined or stayed flat from 2000 to 2017 for most urban and suburban counties. Child and family service nonprofits similarly saw modest increases from 2000 to 2017 across the urban and suburban landscape. Aggregated human service expenditures among smaller nonprofits, however, increased slightly and eclipsed total spending on child and youth services by 2017.
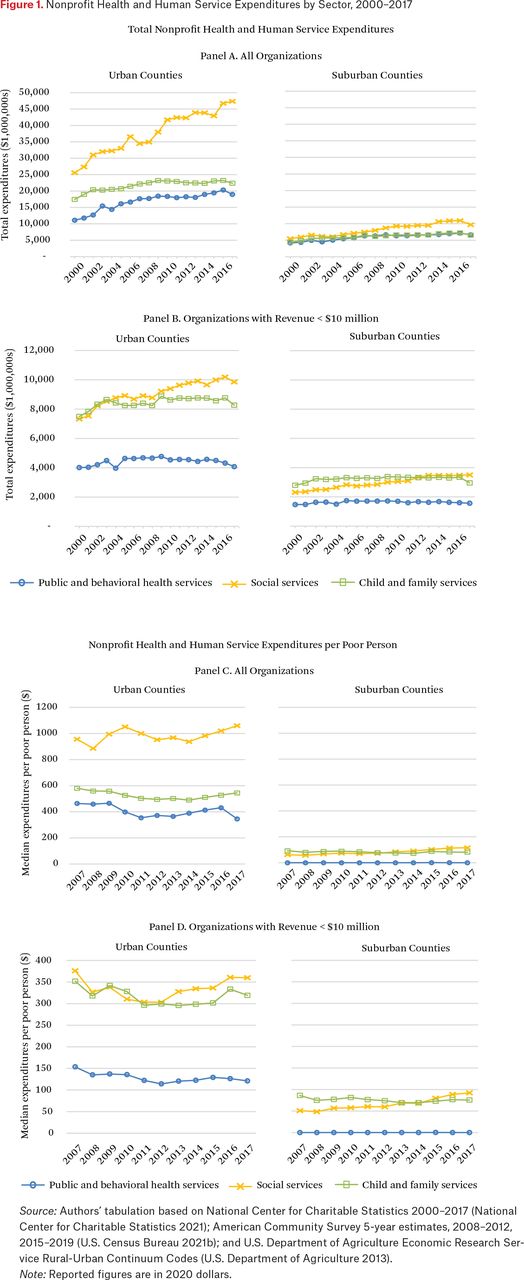
Nonprofit Health and Human Service Expenditures by Sector, 2000–2017
Source: Authors’ tabulation based on National Center for Charitable Statistics 2000–2017 (National Center for Charitable Statistics 2021); American Community Survey 5-year estimates, 2008–2012, 2015–2019 (U.S. Census Bureau 2021b); and U.S. Department of Agriculture Economic Research Service Rural-Urban Continuum Codes (U.S. Department of Agriculture 2013).
Note: Reported figures are in 2020 dollars.
Per poor person, nonprofit health and human service expenditures from 2000 to 2017 reveal several important spatial realities of the contemporary nonprofit safety net (see table 2 and figure 1, panels C and D).8 First, consistent with the earlier discussion, suburban counties dramatically lag urban counties overall. For example, the median large urban county where two-thirds or more of the population lives in a primary city has total nonprofit service spending more than eight times that in the median suburban county in 2017 ($3,431 versus $404 respectively, table 2, third panel, top row). Second, the urban-suburban gaps in per capita nonprofit service expenditures have persisted since 2000. Although median per capita nonprofit health and human service expenditures rose across suburban and urban counties from 2000 to 2017, spending in large urban counties with small suburban populations has consistently outpaced spending in suburban counties by a factor of between eight and nine. Third, urban-suburban inequality in nonprofit expenditures exists within the three major service sectors examined here. Whereas nonprofits in the median urban county in the largest hundred metropolitan areas spent between $496 and $599 per poor person on public and behavioral health services in 2017, the median suburban county had no nonprofit organizations working in this sector (see table 2, third panel, second row). Similarly, nonprofit organizations spent $116 per poor person on social services—education and training, food and housing assistance, and other human services—in the median suburban county in 2017, roughly one-sixteenth of median per capita social service spending in the most urbanized counties (see third panel, third row). Finally, the nonprofit service sectors in more highly suburbanized urban counties consistently lag behind less suburbanized urban counties. Among large urban counties, mean and median per capita health and human service expenditures consistently decrease as the share of the suburban population increases. Taken together, findings in table 2 reveal large and persistent urban-suburban gaps in health and human service provision relative to need. These gaps are evident when comparing formally defined suburban counties with all urban counties, and even when comparing among urban counties with varying degrees of suburbanization. These findings are consistent with our expectations that suburban nonprofit safety nets may be less robust and responsive to local need than in urban areas.
Nonprofit Health and Human Service Expenditures per Poor Person Across Urban and Suburban Counties, 2000–2017
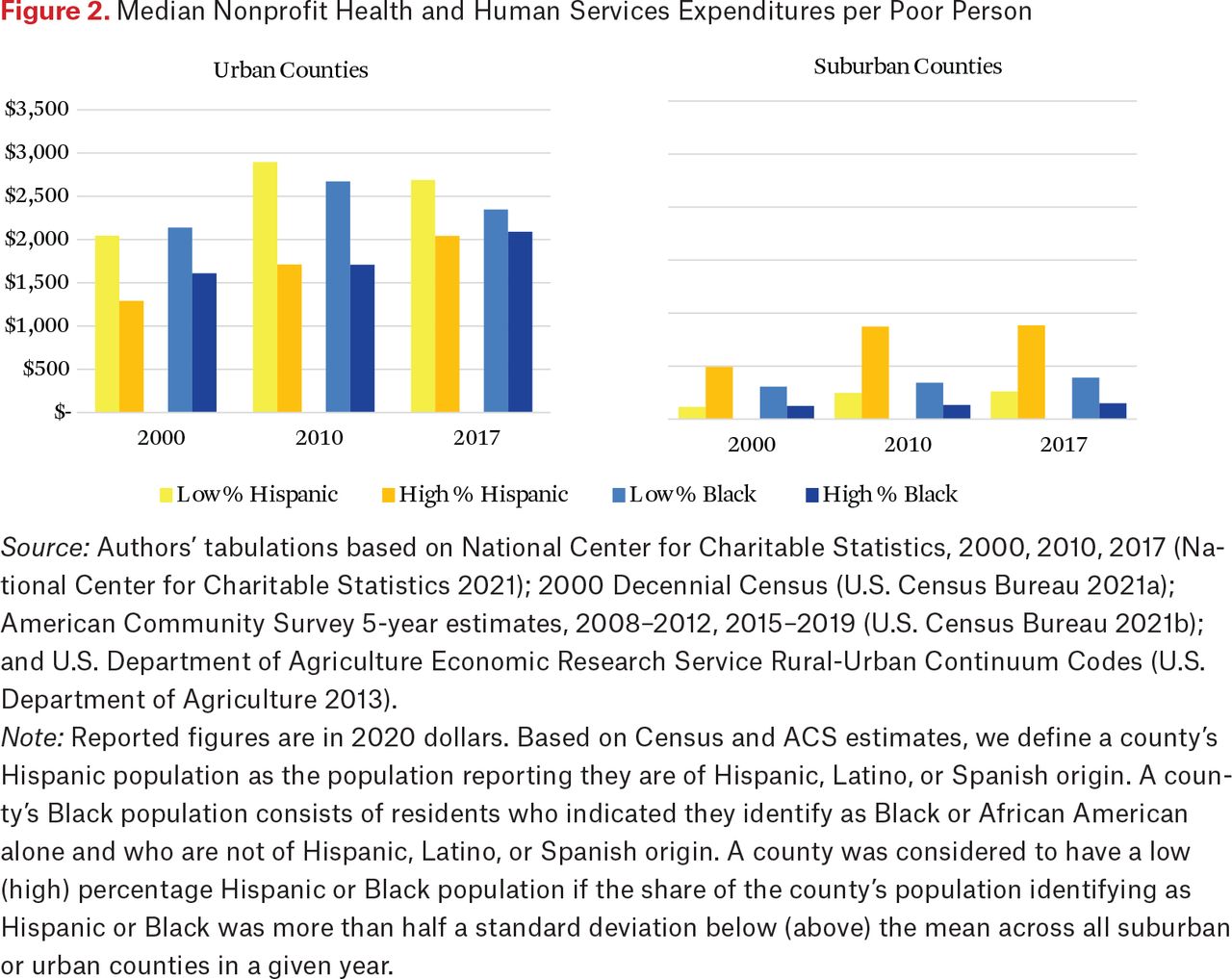
Also consistent with our expectations, figures 2 and 3 demonstrate that nonprofit health and human service capacity in the typical, or median, county varies by the racial and ethnic composition of the population and the county-level poverty rate. We find that the median suburban county in which non-Hispanic Black residents are a large share of the population or that has a high rate of poverty has much lower nonprofit health and human service expenditures per capita than urban counties with similar demographic and socioeconomic characteristics. Figure 2 demonstrates that the median urban and suburban counties where Black residents are a relatively large share of the population have lower expenditures per capita relative to counties where Black residents make up a comparatively smaller share.9 The gap in per capita expenditures between suburban counties where Black residents make up a relatively high share of the population and suburban counties where they make up a relatively small share has been quite persistent over the last twenty years. In 2017, nonprofits in the median suburban county with a low percentage of Black residents spent more than two and a half times as much as those with a high percentage. These findings are consistent with research demonstrating underinvestment in human service organizations in neighborhoods with a larger share of Black residents (Garrow 2014).
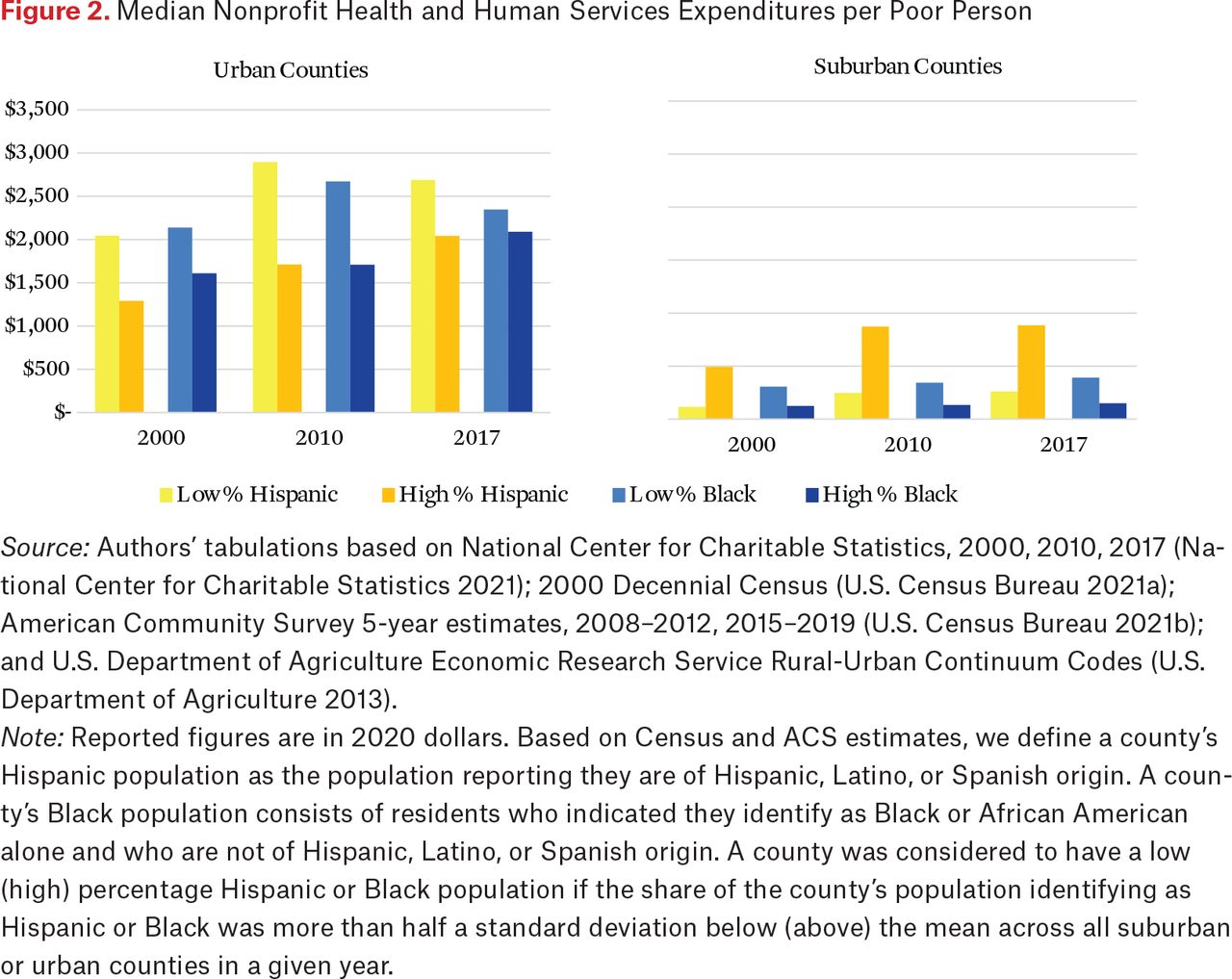
Median Nonprofit Health and Human Services Expenditures per Poor Person
Source: Authors’ tabulations based on National Center for Charitable Statistics, 2000, 2010, 2017 (National Center for Charitable Statistics 2021); 2000 Decennial Census (U.S. Census Bureau 2021a); American Community Survey 5-year estimates, 2008–2012, 2015–2019 (U.S. Census Bureau 2021b); and U.S. Department of Agriculture Economic Research Service Rural-Urban Continuum Codes (U.S. Department of Agriculture 2013).
Note: Reported figures are in 2020 dollars. Based on Census and ACS estimates, we define a county’s Hispanic population as the population reporting they are of Hispanic, Latino, or Spanish origin. A county’s Black population consists of residents who indicated they identify as Black or African American alone and who are not of Hispanic, Latino, or Spanish origin. A county was considered to have a low (high) percentage Hispanic or Black population if the share of the county’s population identifying as Hispanic or Black was more than half a standard deviation below (above) the mean across all suburban or urban counties in a given year.

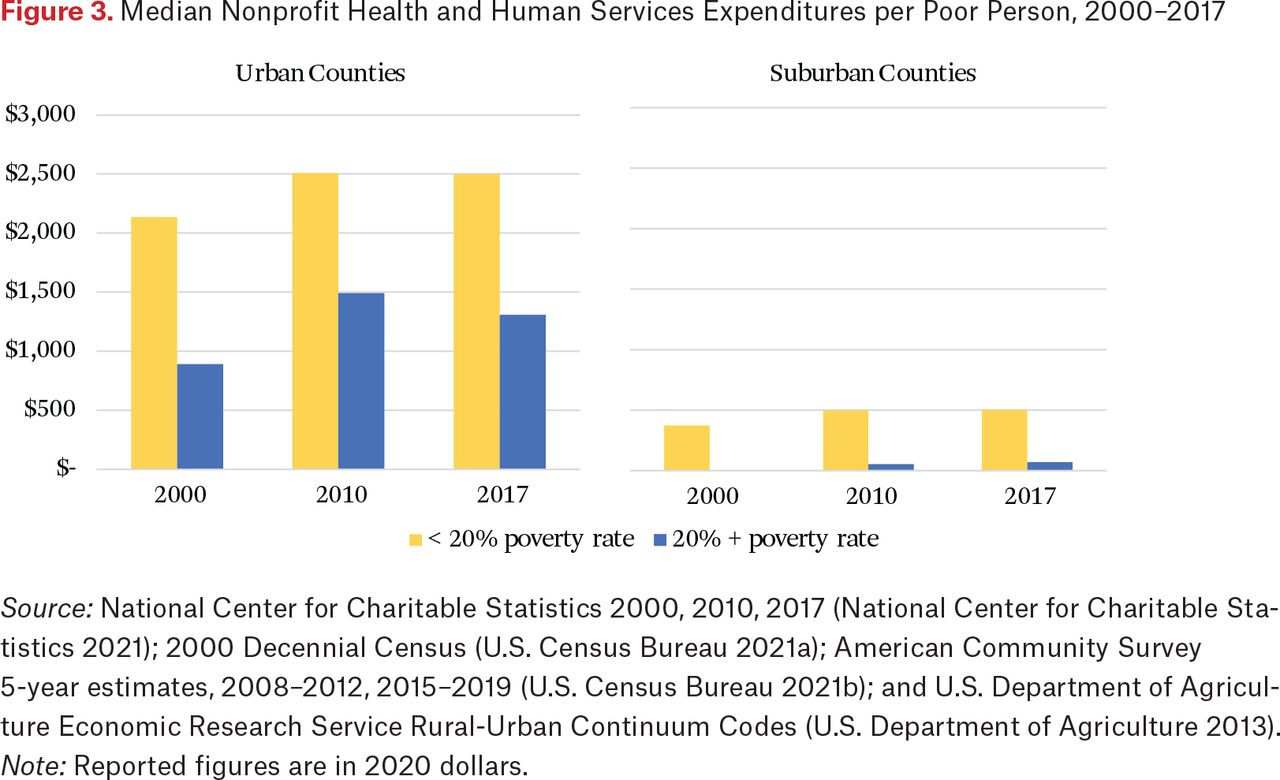
Median Nonprofit Health and Human Services Expenditures per Poor Person, 2000–2017
Source: National Center for Charitable Statistics 2000, 2010, 2017 (National Center for Charitable Statistics 2021); 2000 Decennial Census (U.S. Census Bureau 2021a); American Community Survey 5-year estimates, 2008–2012, 2015–2019 (U.S. Census Bureau 2021b); and U.S. Department of Agriculture Economic Research Service Rural-Urban Continuum Codes (U.S. Department of Agriculture 2013).
Note: Reported figures are in 2020 dollars.
In contrast, we find some evidence that the median suburban county with a relatively high percentage of Hispanic residents has higher nonprofit expenditures per capita than those relatively lower percentages. These findings run counter to our expectations and the prior literature suggesting that suburbs with a higher share of Hispanic residents tend on average to have a more robust nonprofit human service sector than those with a lower share. In general, however, suburban counties with a higher share tend to have higher median household income and higher percentages of adults with college degrees than those with a lower share. Many of these counties are located in traditional Hispanic or Latino immigrant gateway regions and outside large cities with wealthy suburbs, such as metro Washington, D.C., San Francisco, Chicago, and New York City (Singer 2004). By contrast, suburban counties with a higher share of non-Hispanic Black residents are overwhelmingly located in the south and have higher poverty rates than those with a lower share. We return to discussion of this and other bivariate relationships when we present cross-sectional regressions examining a larger set of factors related to per poor person spending.
Significant differences also emerge when we compare median per capita nonprofit expenditures in counties with high federal poverty rates (over 20 percent) to those with lower rates (under 20 percent). Figure 3 illustrates that the median urban county again reports much higher nonprofit expenditures per capita than suburban counties regardless of year or poverty level. In 2017, health and human service organizations in the median high-poverty urban county outspent organizations in the median high-poverty suburban county by a factor of nineteen. The typical low-poverty urban county had more than five times the per capita level of spending present in the median low-poverty suburban county. Notably, spending per poor person in high-poverty urban counties, although lower than in low-poverty urban counties, is still nearly three times that in low-poverty suburban counties and more than eighteen times that in high-poverty suburban counties. Nonprofit organizations in low-poverty urban and suburban counties consistently spend more per poor resident than organizations in high-poverty urban or suburban counties. Among suburban counties, for example, nonprofits in low-poverty suburbs spent more than seven times as much per poor resident than those in high-poverty suburbs. These results are consistent with the literature and our expectations that suburban safety nets lag urban safety nets in capacity, particularly in suburban settings where need may be greatest (Allard 2017; Berube and Kneebone 2013).10
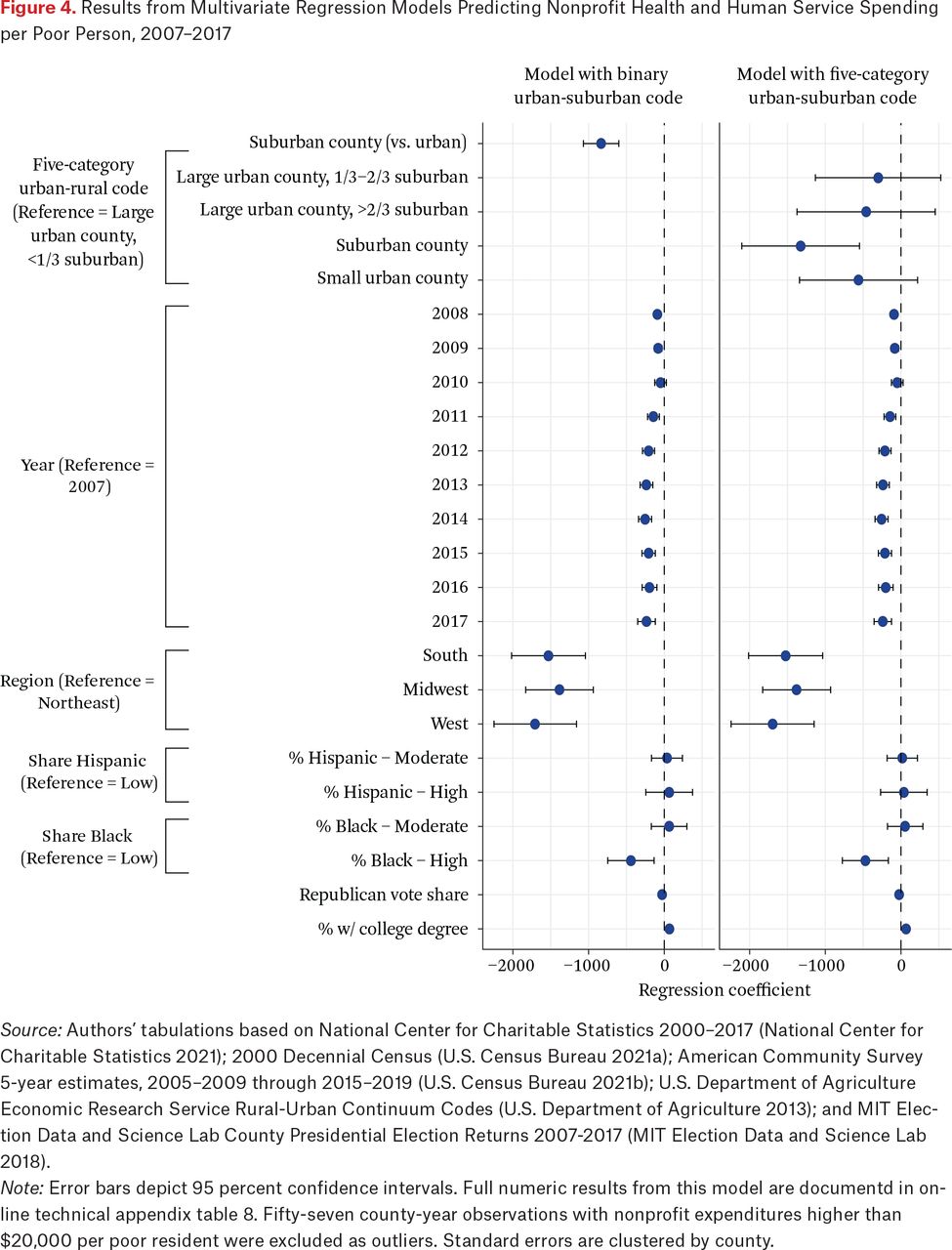
As noted, we present cross-sectional descriptive regressions analyzing factors associated with county-level nonprofit spending per poor person in figure 4. Specifically, we estimate pooled linear regression models predicting per capita spending in each county for each year between 2007 and 2017 with standard errors clustered by county.11 To capture county geography, we estimate models using both a dichotomous urban-suburban measure and a five-category urban-suburban continuum code. We control for year, region, racial and ethnic composition of the county, Republican vote share in the most proximate presidential election, and share of adults with a college degree. Figure 4 depicts coefficients and confidence intervals from these models; technical appendix tables 8 and 9 show full numeric results.
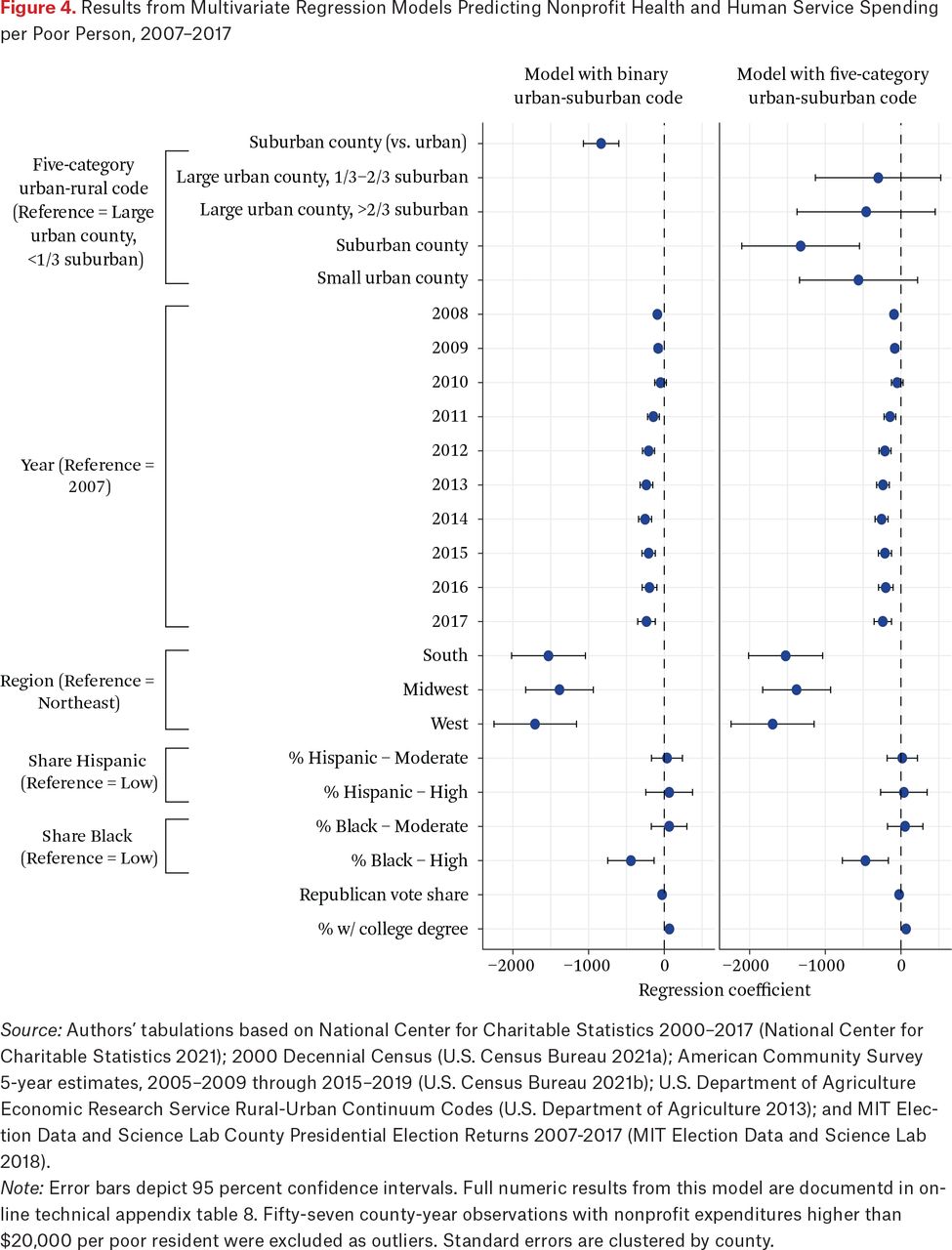
Results from Multivariate Regression Models Predicting Nonprofit Health and Human Service Spending per Poor Person, 2007–2017
Source: Authors’ tabulations based on National Center for Charitable Statistics 2000–2017 (National Center for Charitable Statistics 2021); 2000 Decennial Census (U.S. Census Bureau 2021a); American Community Survey 5-year estimates, 2005–2009 through 2015–2019 (U.S. Census Bureau 2021b); U.S. Department of Agriculture Economic Research Service Rural-Urban Continuum Codes (U.S. Department of Agriculture 2013); and MIT Election Data and Science Lab County Presidential Election Returns 2007-2017 (MIT Election Data and Science Lab 2018).
Note: Error bars depict 95 percent confidence intervals. Full numeric results from this model are documentd in online technical appendix table 8. Fifty-seven county-year observations with nonprofit expenditures higher than $20,000 per poor resident were excluded as outliers. Standard errors are clustered by county.
These descriptive regression models illustrate that disparities in nonprofit spending between suburban and urban counties persist after controlling for key elements of demographic, socioeconomic, and political context. Using the dichotomous urban-suburban designation, suburban counties spent $835 less per poor resident, on average, than urban counties.12 Nonprofits in counties in the Northeast spent the most per poor resident, followed by Southern, Midwestern, and Western. Counties with a larger Black share of the population had significantly lower per capita expenditures. A higher share of the population voting for a Republican in the closest presidential election was associated with lower nonprofit spending per poor resident. Finally, higher county educational attainment was associated with higher per capita spending. These results underscore the patterns of persistent suburban-urban disparities we find throughout our descriptive analyses; when comparing urban and suburban regions with otherwise similar characteristics, suburban nonprofit safety nets are significantly less robust than local need.
Unlike the bivariate relationships discussed, however, our descriptive regressions do not provide evidence of statistically significant differences in expenditures between suburban counties where Hispanics made up a larger versus smaller share of the population when controlling for other county-level characteristics.13 Instead, observed mean differences in human service spending across suburban counties by Hispanic population may be more closely connected to other socioeconomic or political characteristics of suburban counties than to the relative size of the Hispanic community. We also interpret these results with the limitations of these data in mind. Not only do our census data smooth over important variation within Hispanic communities, but higher human service expenditures in suburban counties with large Hispanic communities also do not necessarily equate with services accessible to or used by Hispanic residents of those communities.14 Combined, our findings indicate need for greater scholarly inquiry into the complex relationships between the composition of the Hispanic population and nonprofit human service provision in suburban America.
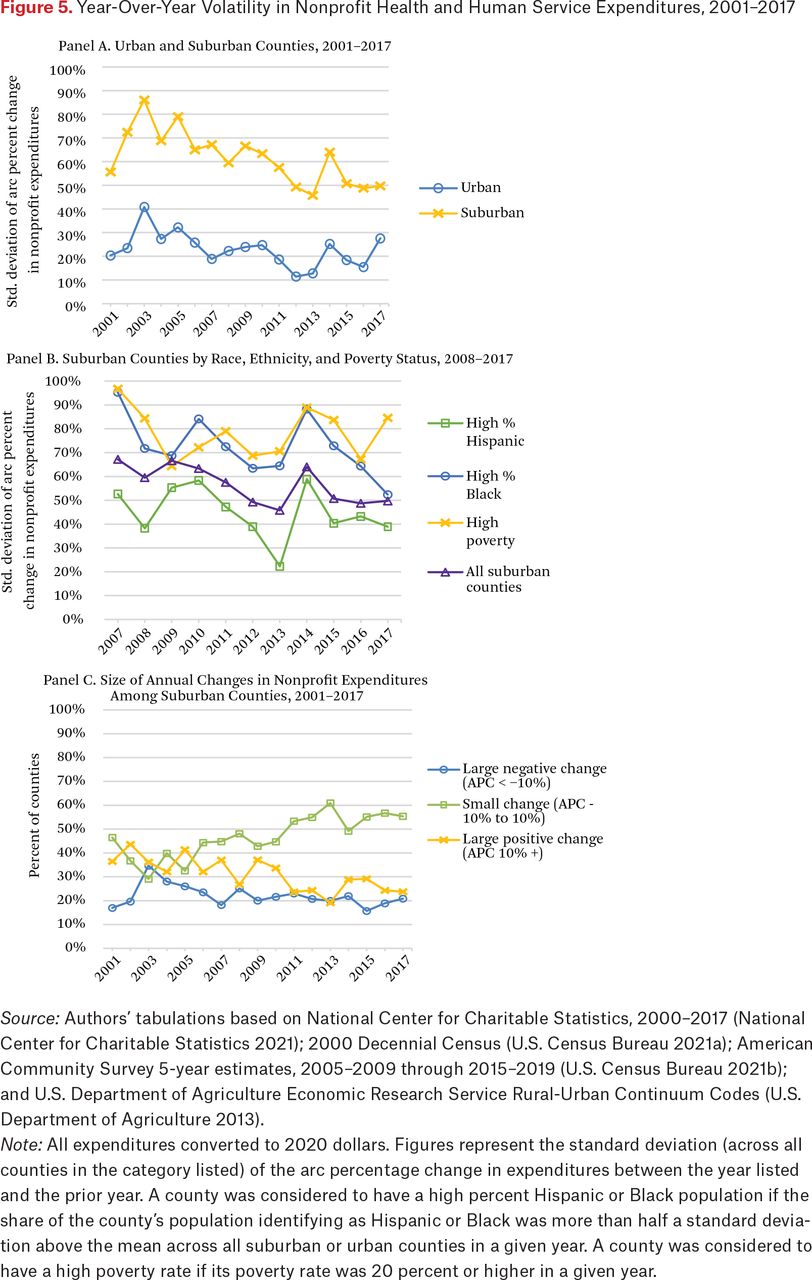
Next, we examine volatility and change in nonprofit health and human services expenditures across urban and suburban geography. Figure 5 presents year-to-year volatility of total expenditures by health and human service organizations in counties.15 To capture year-to-year volatility in expenditures, we first use the standard deviation of the arc percentage change as our main summary statistic (see Dahl, DeLeire, and Schwabish 2011).16 This measure captures the spread of year-to-year arc percentage changes among a group of counties, summarizing the overall volatility of nonprofit expenditures in that group of counties from one year to the next.17
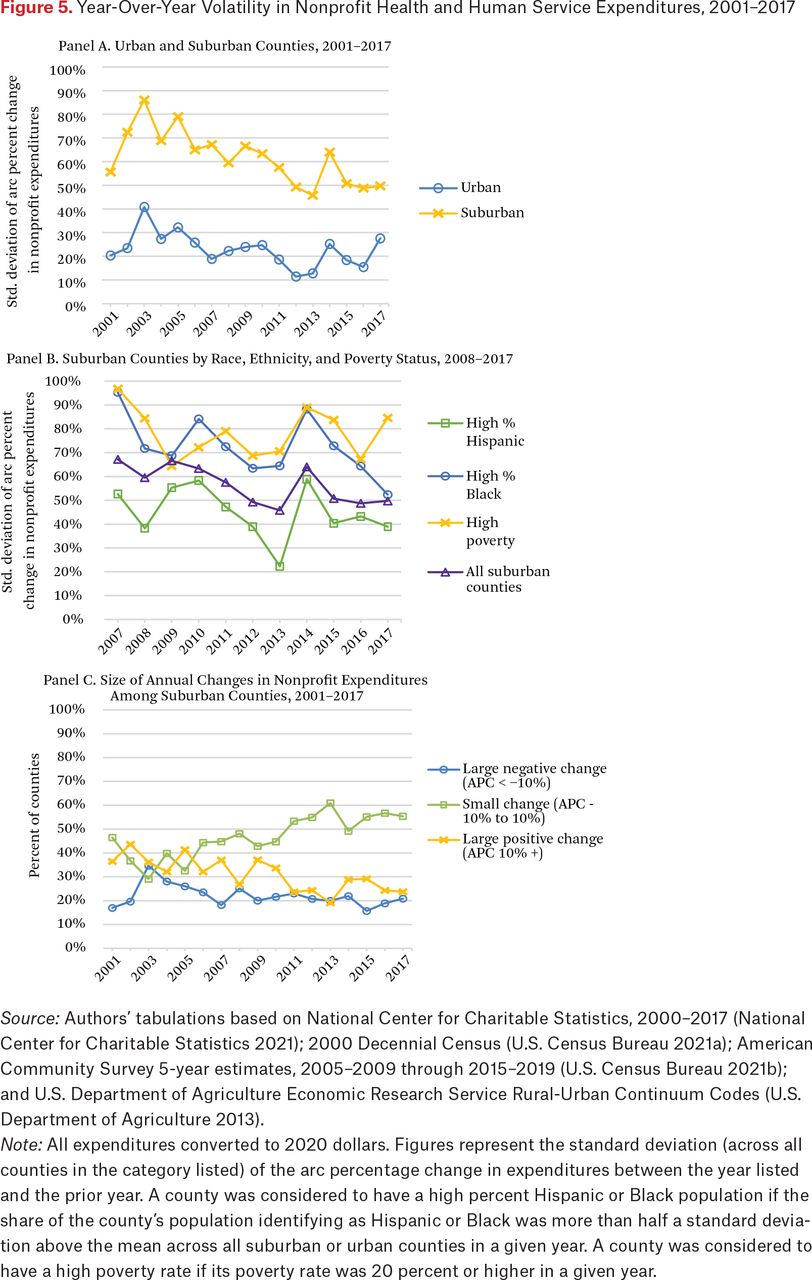
Year-Over-Year Volatility in Nonprofit Health and Human Service Expenditures, 2001–2017
Source: Authors’ tabulations based on National Center for Charitable Statistics, 2000–2017 (National Center for Charitable Statistics 2021); 2000 Decennial Census (U.S. Census Bureau 2021a); American Community Survey 5-year estimates, 2005–2009 through 2015–2019 (U.S. Census Bureau 2021b); and U.S. Department of Agriculture Economic Research Service Rural-Urban Continuum Codes (U.S. Department of Agriculture 2013).
Note: All expenditures converted to 2020 dollars. Figures represent the standard deviation (across all counties in the category listed) of the arc percentage change in expenditures between the year listed and the prior year. A county was considered to have a high percent Hispanic or Black population if the share of the county’s population identifying as Hispanic or Black was more than half a standard deviation above the mean across all suburban or urban counties in a given year. A county was considered to have a high poverty rate if its poverty rate was 20 percent or higher in a given year.
Panel A of figure 5 reveals that nonprofit health and human service spending is significantly more volatile in suburban counties than in urban ones. From one year to the next, that is, suburban counties are more likely than urban counties to experience a dramatic change in nonprofit expenditures in either direction, suggesting less stable or established sectors and funding streams than in urban areas. The gap between expenditure volatility in urban and suburban counties has narrowed slightly over time, and the overall downward trend in volatility has been downward among both types of counties since the early 2000s.
Panel B of figure 5 presents expenditure volatility across subgroups of suburban counties. Relative to the average for all suburban counties, year-over-year volatility in health and human service expenditures is generally higher in suburbs with a relatively large percentage of the Black population as well as in suburbs with a poverty rate above 20 percent. Taken together, panels A and B of figure 4 illustrate that the groups of counties we observed to have lower total and per capita expenditures, on average, also exhibit more volatility in expenditures over time. Moreover, we find that suburban counties overall have less stable nonprofit health and human service sectors than urban counties. Suburban counties with a relatively large Black population or high poverty rates appear to have the most unstable or volatile nonprofit health and human service sectors. Again, these findings are consistent with expectations derived from the literature that suburban counties—perhaps particularly those in which people of color are a large percentage of the population—may lack the capacity in their nonprofit human service sectors to respond to community need.
The standard deviation of the arc percentage change measures overall volatility but does not reveal the extent of positive versus negative changes in expenditures. Panel C of figure 5, therefore, examines both the size and directionality of year-to-year changes in nonprofit expenditures among suburban counties over time. Note that the y-axis in panel C depicts the percent of counties experiencing different sizes and magnitudes of year-over-year changes in nonprofit expenditures, in contrast to the y-axis in panels A and B, which depict the standard deviation of the year-over-year arc percentage change in expenditures. A significant and rising share of suburbs showed only a small change in expenditures (defined as an increase or decrease of 10 percent or less), mirroring the overall decline in expenditure volatility illustrated in panel A of figure 5. The share of counties with large positive changes (a more than 10 percent increase) has typically but not always been higher than the share with large negative changes. In each year between 2010 and 2017, between 25 and 35 percent of suburban counties saw increases of more than 10 percent, whereas around 20 percent saw them fall by more than 10 percent.
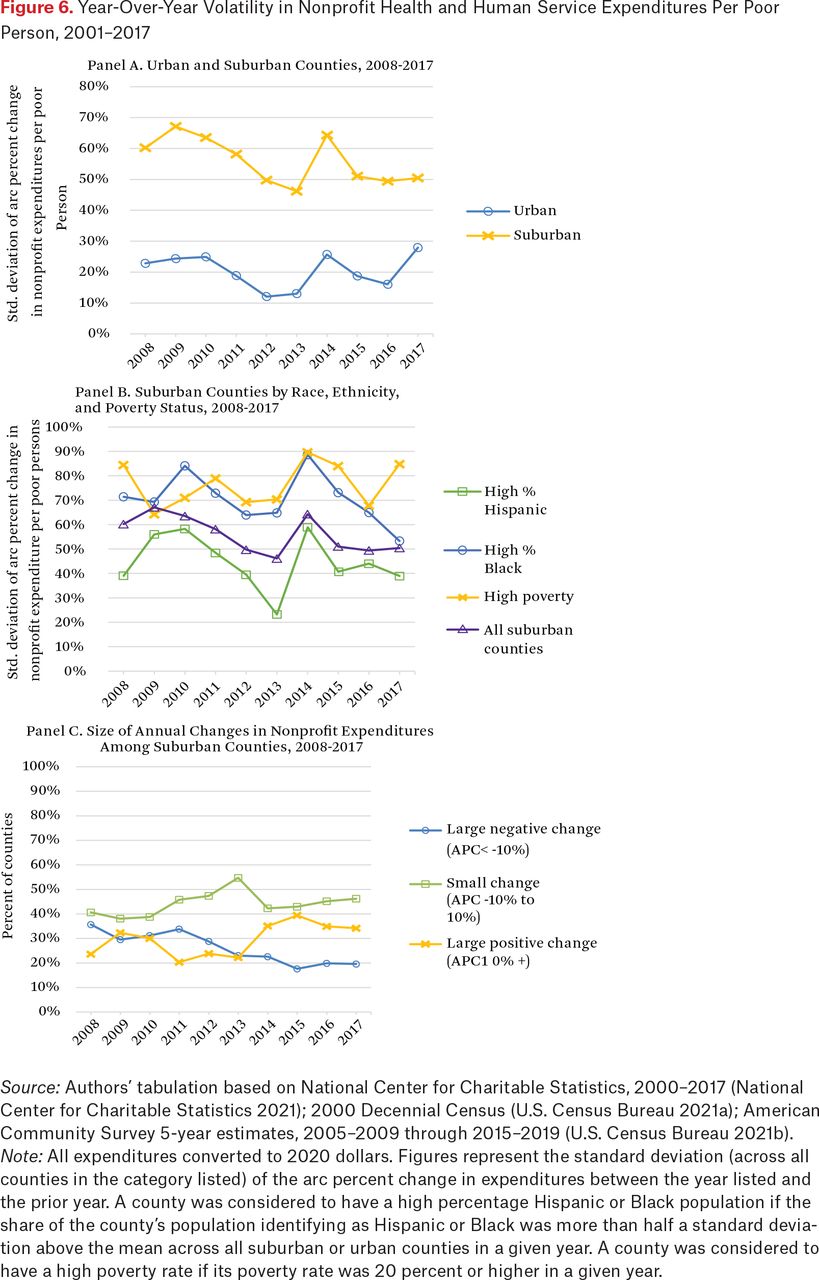
Figure 6 uses the same methodology to examine year-over-year volatility in nonprofit expenditures per poor person across counties. A similar story emerges when looking at this measure that has been adjusted to capture expenditures in relation to need. Panel A indicates that suburban counties see significantly more year-over-year volatility in per capita health and human service expenditures than urban counties do. Suburban counties with a relatively large Black population or with a high poverty rate also tend to have more volatility in per capita nonprofit expenditures than other types of suburban counties (see panel B). Finally, panel C illustrates the distribution of year-over-year changes in per capita expenditures in suburban counties by size and directionality. The share of counties experiencing a small change in this metric from a given year to the next ranges between roughly 40 and 55 percent, peaking in 2013. In recent years, more counties have experienced large positive changes than large negative ones, although the opposite has been true in some years. This is consistent with the overall growth in the sector in the period we examine. That said, a significant share of suburban counties sees large drops in nonprofit spending from one year to the next. Between 2016 and 2017, 20 percent saw more than a 10 percent decrease in per capita spending by health and human service organizations.

Year-Over-Year Volatility in Nonprofit Health and Human Service Expenditures Per Poor Person, 2001–2017
Source: Authors’ tabulation based on National Center for Charitable Statistics, 2000–2017 (National Center for Charitable Statistics 2021); 2000 Decennial Census (U.S. Census Bureau 2021a); American Community Survey 5-year estimates, 2005–2009 through 2015–2019 (U.S. Census Bureau 2021b).
Note: All expenditures converted to 2020 dollars. Figures represent the standard deviation (across all counties in the category listed) of the arc percent change in expenditures between the year listed and the prior year. A county was considered to have a high percentage Hispanic or Black population if the share of the county’s population identifying as Hispanic or Black was more than half a standard deviation above the mean across all suburban or urban counties in a given year. A county was considered to have a high poverty rate if its poverty rate was 20 percent or higher in a given year.
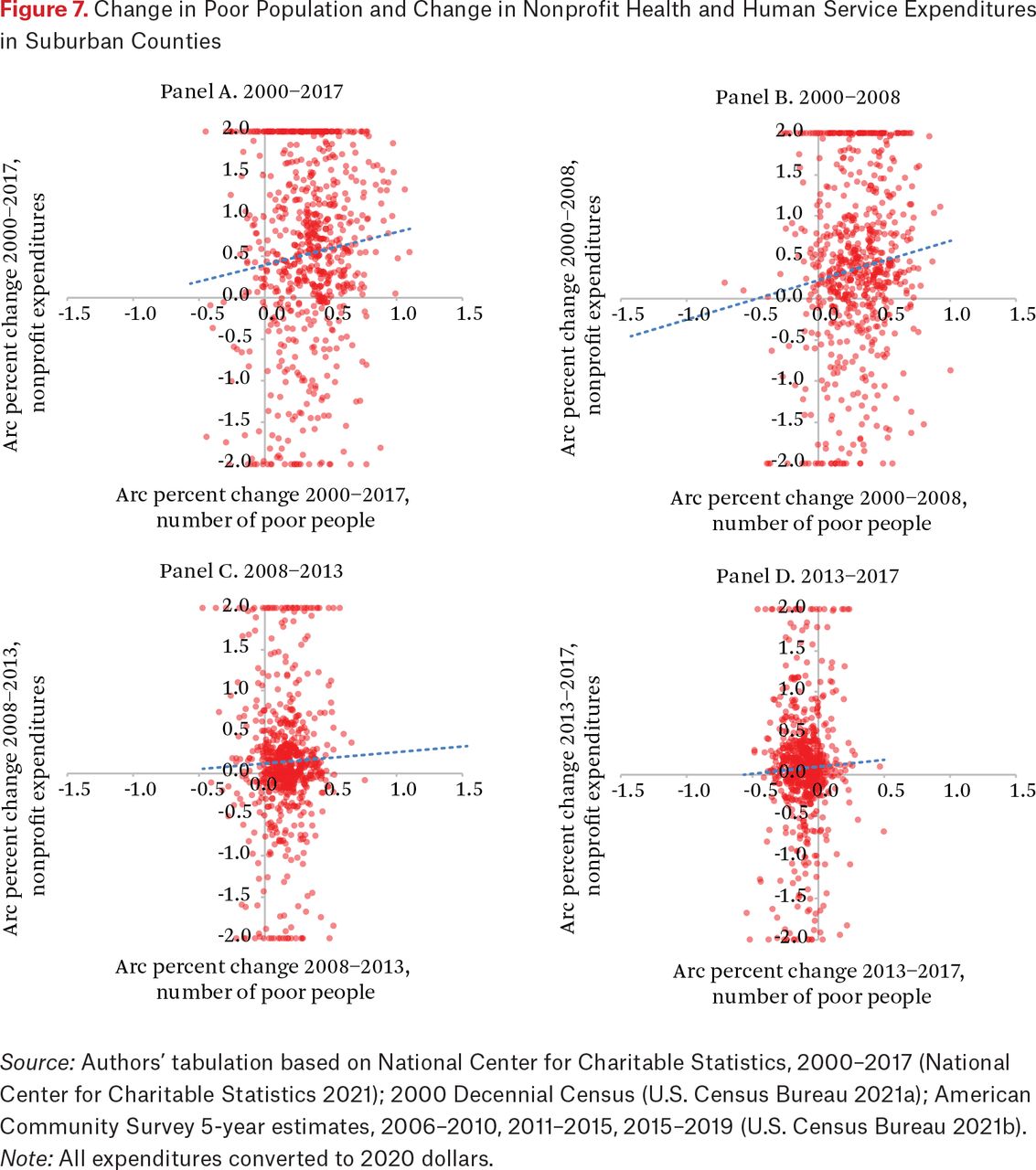
Next, we use a series of scatterplots to examine the full distribution of arc percentage changes in nonprofit expenditures among suburban counties relative to that in the number of poor people in that county. Panel A of figure 7 depicts these changes over a seventeen-year window, plotting the changes in the two metrics for each county between 2000 and 2017. We then examine changes over three periods: 2000 to 2008, representing trends prior to the Great Recession; 2008 to 2013, during and just after the recession; and 2013 to 2017, as the effects receded. We selected 2008 to represent a prerecession year and 2013 to represent the recovery. Counties plotted in the top right quadrant of these plots are where both the population in poverty and nonprofit health and human service expenditures increased. The bottom right quadrant indicates that the county had an increase in poor residents over the period but a decrease in nonprofit health and human service expenditures. Similarly, the left quadrants represent counties that had a decrease in the number of poor residents and an increase (top left quadrant) or decrease (bottom left quadrant) in nonprofit expenditures. A linear best fit trend line is also plotted.
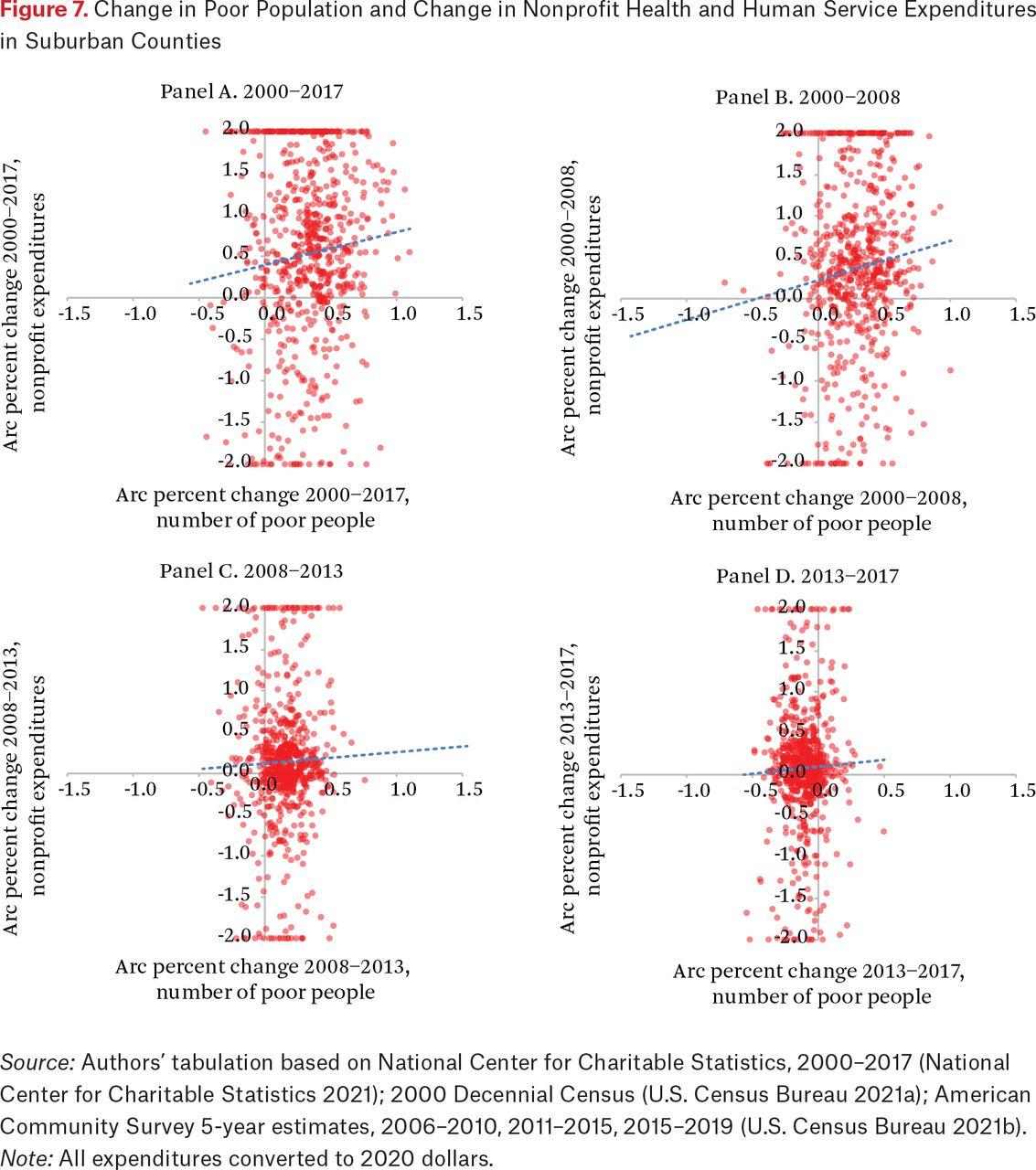
Change in Poor Population and Change in Nonprofit Health and Human Service Expenditures in Suburban Counties
Source: Authors’ tabulation based on National Center for Charitable Statistics, 2000–2017 (National Center for Charitable Statistics 2021); 2000 Decennial Census (U.S. Census Bureau 2021a); American Community Survey 5-year estimates, 2006–2010, 2011–2015, 2015–2019 (U.S. Census Bureau 2021b).
Note: All expenditures converted to 2020 dollars.
Consistent with prior research and table A.1, panel A of figure 7 indicates that the vast majority of suburban counties saw an increase in the number of poor residents between 2000 and 2017. At the same time, most suburban counties also saw a net increase in nonprofit expenditures from 2000 to 2017. The positive slope of the best fit line indicates that, on the whole, positive changes in the number of poor people were associated with positive changes in health and human service spending. A relatively similar trend is evident in panel B of figure 7 when looking only at the years 2000 to 2008. Most counties saw increases in their total population in poverty, as evidenced by the prevalence of the points to the right of the y-axis. An upward slope of the best fit trend line indicates that, in general, rising poverty was associated with rising nonprofit expenditures over this period. This plot also illustrates, however, that many counties with large changes in the poor population that saw decreases in nonprofit expenditures or relatively small increases that did not keep pace with the increase in poverty. Panel C exhibits a different pattern; between 2008 and 2013, the relationship between the change in expenditures and change in poverty is relatively flat—evidence that suburban nonprofit sectors were not, on the whole, responsive to changes in need in this time interval.18 The slope of the best fit line in panel D is also relatively flat, indicating that nonprofit expenditures were less responsive to changes in need between 2013 and 2017. So, even though nonprofit health and human service spending appears to be somewhat responsive to need before 2008, little evidence suggests that it was responsive to need manifest during and following the Great Recession.
Taken together, the findings presented here fit with our expectations that suburban nonprofit human service safety nets not only lag urban nonprofit human service safety nets in capacity, but also lack the local organizational capacity and resources needed to address the rising poverty and hardship that accompanies economic downturns. On the whole, suburban nonprofit human service safety nets are less robust, more volatile, and less responsive to local need than urban counties’ nonprofit sectors, and especially in high-poverty suburbs and suburbs with larger Black populations.
DISCUSSION AND CONCLUSION
Several key findings emerge from our analyses of nonprofit health and human service provision in urban and suburban counties over the past two decades. First, the service safety net appears more responsive to need in urban centers than in suburban areas. Second, nonprofit health and human service spending appears less countercyclical than is commonly understood. We observe higher year-to-year volatility in nonprofit expenditures within suburban counties, which suggests that nonprofits may provide less consistent or reliable supports than urban areas. Finally, nonprofit spending is not as well matched to the geography of poverty as we should expect. In particular, we find evidence that nonprofit health and human service provision per poor resident is less robust in suburban areas, and especially in those experiencing high rates of poverty or areas with a relatively higher share of Black residents. Urban-suburban disparities in nonprofit service provision persist after controlling for a number of county-level demographic and socioeconomic factors in multivariate regression models. We interpret these findings with caution, however, because our county-level analyses smooth over more fine-grained differences in human service capacity across neighborhoods within a given county or metropolitan area as well as between suburban and rural communities at the edges of contemporary metropolitan boundaries.
Evidence presented here suggests several key areas for future research inquiry. Considerable opportunity remains to advance conceptual and empirical understanding of the structural, political, and social factors behind urban and suburban variation in nonprofit safety net capacity. Central to this work is developing greater empirical insight into the circumstances under which urban and suburban nonprofit safety nets are more or less responsive to rising poverty. Given the disparities we observe in nonprofit service provision across communities with large racial and ethnic minority communities, cross-disciplinary research is needed to consider how growing suburban racial and ethnic diversity is changing (or not changing) the work of local public and nonprofit human service organizations. For example, future research should explore the extent to which local organizations adjust program models, outreach, staffing, and leadership structures in response to rising racial and ethnic diversity. Scholars should consider how local and regional charitable philanthropies shift program funding and community engagement in grantmaking in the midst of rising suburban poverty and racial diversity. Additional research should examine how the changing racial and ethnic composition of suburban communities affects the siting or location of human service programs. Finally, future research should seek pathways to overcome the limitations of existing IRS 990 and proprietary data, which do not permit fine-grained geographic analysis of nonprofit health and human service provision across urban and suburban geography. Articles in this and the previous issue of this volume show, however, that greater insights into neighborhood-level access to nonprofit service organizations will emerge from a combination of creative large-N studies and well-crafted case studies.
Urban-suburban disparities in nonprofit health and human service safety nets should prompt discussion about conventional approaches to safety net funding and delivery. The current public-private partnership around health and human service provision appears mutually beneficial for government and nonprofit organizations. Government funds allow federal, state, and local agencies to provide a wider array of services with greater flexibility than would be possible through direct public delivery. Nonprofit service organizations often view public funds as opportunity to increase the scope of services provided, build capacity to advance core organizational missions, and elevate community impact. Yet this arrangement depends on local economic, political, and social conditions. Moreover, institutional realities and competitive pressures limit the ability of local and regional government to respond to increases in hardship. What results is at best a weakly countercyclical and patchwork health and human service safety net that may not provide accessible or predictable assistance to those most in need.
Consequently, we believe that local leaders and policymakers could take a number of steps to strengthen nonprofit human service capacity and program provision. First, it is difficult to build new programs and organizational capacity from scratch overnight, which should lead local communities to use pilot programs as pathways for testing program delivery models, developing local human service capacity, and generating greater public support for future programmatic activity. Second, as Angela Simms (2023, this issue) notes, local policymakers should develop intentional regional partnerships that seek solutions to fragmented delivery systems and puzzles around economies of scale that often reduce service accessibility in suburban areas. Apart from addressing real-time barriers to service provision and access, regional partnerships also can lead to new program funding from state and federal agencies (Allard 2017; Berube and Kneebone 2013). Finally, charitable foundations should reach beyond the traditional urban boundaries that guide their work to establish programming and foster new private charitable giving in suburban communities. Philanthropy also should use its convening power to help promote greater understanding about the realities of suburban poverty and support greater regional provision of social assistance to underserved areas or communities.
Local actors may find that the tools available are unable to fully remedy spatial disparities in provision of nonprofit health and human services in the immediate term. Thus local public and nonprofit leaders should work with state government to identify new federal spending that could invest in suburban human service capacity, as has been done in urban centers since the 1960s. In addition, policymakers should ensure that federal appropriations to key human service funding streams, such as the Community Development Block Grant and the Social Services Block Grant, be increased to reflect rising poverty outside of cities and adjusted annually to keep pace with inflation. The federal government also should create a competitive federal grants race-to-the-top program that incentivizes and rewards innovative regional strategic plans to better coordinate human service programs across urban and suburban spaces within metropolitan America.
Finally, we believe the success of efforts to strengthen the nonprofit health and human service sector in metropolitan America requires a commitment to reduce racial as well as spatial disparities in access to assistance. Evidence presented here and elsewhere that communities of color—in cities and suburbs—have less access to nonprofit programs of assistance than predominantly White communities are a powerful reminder of the persistent presence of racial inequality in delivery of social assistance in the United States. Given the growing racial and ethnic diversity of America’s suburbs (Lichter, Thiede, and Brooks 2023), local policymakers and philanthropy should work to increase the representation of historically marginalized groups in community leadership positions. Such representation will help promote development of local services more responsive to community needs (see also Girouard 2023). If society and policy communities wish to meaningfully reduce racial disparities in poverty and inequality, then we must remedy the racial and ethnic inequalities embedded in the nonprofit human service components of the contemporary safety net.
FOOTNOTES
↵1. Because we analyze data between 2000 and 2017, our analysis does not capture changes in economic need related to the COVID-19 pandemic, the effects of subsequent stimulus funding on nonprofit organizations, or the effects of the Child Tax Credit expansion on poverty.
↵2. The data and methods section and the online technical appendix (see https://www.rsfjournal.org/content/9/2/134/tab-supplemental) provide more detailed discussion about the contours, organizational structures, and fiscal realities of the nonprofit human service safety net.
↵3. L’Heureux Lewis-McCoy and his colleagues (2023, this issue) provide a more thorough overview of how scholarship defines urban versus suburban areas. For more detail on geographic definitions relevant to this study, see Allard 2017; Allard and Pelletier 2021.
↵4. This approach sorts counties into two strata. Elsewhere in this volume, Daniel Lichter, Brian Thiede, and Matthew Brooks (2023) describe suburban patterns of racial and ethnic segregation in detail.
↵5. Nonprofits health organizations are defined as those that self-classify in one of the following National Taxonomy of Exempt Entities (NTEE) codes (see Jones 2019): public health (E70); behavioral health services (F20, F21, F22, F30, F32, F33, F60). Social service organizations are defined as those that self-classify as one of the following NTEE codes: adult education and training (B60, J20, J21, J22, J30, J32, J33); emergency assistance (K30, K31, K34, K35, K36); housing assistance (L40, L41, P84); human services (P20, P21, P22, P24, P27, P28, P29, P50, P51, P52). Nonprofit child and family service organizations are those that self-classify as one of the following NTEE codes: preschool and daycare (B21, P33); child and family services (O20, O21, O22, O23, P27, P30, P40, P42, P43, P44, P45, P46).
6. The arc percentage change is commonly used to measure income volatility (see, for example, Dahl, DeLeire, and Schwabish 2011). It has three useful features. First, it is bounded by -200 and 200, reducing the influence of outliers. Second, it is equal for the same magnitude of increase or decrease from a given base value. Third, it is defined when expenditures are zero in either y or y-1.
↵7. For more details about the NCCS data and the types of nonprofit organizations or religious congregations that are not required to file 990 forms with the IRS, see the online appendix.
↵8. Technical appendix table 3 presents these results for organizations with revenue less than $10 million.
↵9. Our measures of county racial composition distinguish counties with a relatively large or small share of a particular group relative to other urban or suburban counties that year, as described in more detail in the data and methods section.
↵10. Although our focus here is on aggregate trends across urban and suburban counties, technical appendix table 7 presents county-specific per capita nonprofit expenditures for the Atlanta, Chicago, and Seattle-Tacoma metropolitan areas. Closer examination of these three metros in the technical appendix yields findings consistent with those reported here—suburban nonprofit health and human safety nets lag urban centers in capacity. These detailed tables, however, reveal the differences in urban and suburban nonprofit health and human service expenditures by region and the considerable heterogeneity across suburban counties within each metropolitan area.
↵11. Technical appendix table 10 presents descriptive statistics for the samples used in these models.
↵12. We found similar results when we used the five-category urban-suburban scale; suburban counties spent $1,326 less per poor resident when compared to the largest, least suburbanized urban counties. We also tested specifications with county socioeconomic and demographic variables interacted with the urban-suburban indicator. These interaction terms did not improve model fit, suggesting that the association between these variables and nonprofit expenditures was similar for urban and suburban counties. Full results from these models available on request from the authors.
↵13. Technical appendix tables 3 and 4 describe how key characteristics of counties differ across our racial-ethnic composition categories, providing some insight into the types of counties that fall into each of these categories.
↵14. In particular, suburban nonprofit organizations face numerous barriers in serving immigrant communities; available services do not always meet the needs of individuals (see Roth, Gonzales, and Lesniewski 2015).
↵15. Figure 5 depicts volatility in total expenditures unadjusted for local need. The volatility could thus mean that the nonprofit sector is changing in response to changing need. In figure 6, we explore whether the volatility we observe in nonprofit expenditures matches changes in county-level need by calculating year-over-year volatility in human service expenditures per poor resident.
↵16. For more information on how the arc percentage change is calculated and the merits of this measure, see the data and methods section.
↵17. For example, between 2016 and 2017, the mean arc percentage change in expenditures for urban counties was -1.8 percent and that for suburban counties was -0.6 percent. Because the standard deviation of this measure was much larger for suburban counties (50 versus 28 percent for urban counties), suburban counties’ year-over-year changes were much more spread out around this mean, meaning that more suburban counties experienced dramatic swings in expenditures from one year to the next than urban counties did. For example, 50 percent of counties saw their expenditures change by between -4 and 5 percent. In contrast, in suburban counties, only 33 percent of counties had expenditure changes within this range. A larger standard deviation implies a more dispersed distribution of changes, indicating that counties are seeing more year-over-year variability in nonprofit expenditures.
↵18. Technical appendix figures 4 through 7 depict the same analyses for the same time windows (2000–2017, 2000–2008, 2008–2013, and 2013–2017), for specific subgroups of counties based on the racial and ethnic composition of the population and the county poverty rate.
- © 2023 Russell Sage Foundation. Allard, Scott W., and Elizabeth Pelletier. 2023. “Volatility and Change in Suburban Nonprofit Safety Nets.” RSF: The Russell Sage Foundation Journal of the Social Sciences 9(2): 134–60. DOI: 10.7758/RSF.2023.9.2.06. The authors thank the Peter G. Peterson Foundation and Ford Foundation U.S. 2050 Initiative for providing research support of this project. Direct correspondence to: Scott W. Allard, at sallard{at}uw.edu, Daniel J. Evans Endowed Professor of Social Policy, Evans School of Public Policy and Governance, University of Washington, Box 353055, Seattle, WA 98195-3055, United States; Elizabeth Pelletier, at epell{at}uw.edu, Evans School of Public Policy and Governance, University of Washington, Box 353055, Seattle, WA 98195-3055, United States.
Open Access Policy: RSF: The Russell Sage Foundation Journal of the Social Sciences is an open access journal. This article is published under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.