
Abstract
We analyze Illinois families facing multiple barriers and their interactions with public-sector services. Using administrative data from five state agencies to identify families’ receipt of child welfare, mental health, and substance abuse services as well as adult and juvenile incarcerations, we identify individuals across systems using probabilistic record-linkage techniques, defining family clusters based on networks of individuals who share child welfare and food stamp cases. We show that 23 percent receive services in two or more of these areas. This concentration accounts for 86 percent of the funding for these services used by the entire sample. They experience more and more severe problems. This population is otherwise heterogeneous, engaging with different types of services and clustered in certain parts of the state.
The public system that has developed over the past half century to address social issues such as criminal behavior, juvenile delinquency, child maltreatment, mental illness, and substance abuse is a set of fragmented funding mechanisms, services, and programs (Wilkins 2012). These problems affect both the individual and their family members. Multiple family members with these problems are likely to increasingly challenge a family’s most basic normative roles. Having a deeper understanding of families’ circumstances is critical to any community’s approach to using the scarce resources available to address the needs of vulnerable families. We aspire to characterize the involvement of multiple systems in families’ lives as a way to understand overall need of families as well as to quantify the share of the total government effort and funding spent on multisystem families.
Understanding the number and characteristics of multisystem families requires multiple sources of data because primary data collection from a general population or even a targeted one would not be feasible from either a cost or data quality perspective. Simply the question of who in a household would be able to report reliably on the participation of each family member in the government programs listed already takes addressing this question to a higher degree of difficulty. Multiple household members would have to recall their participation in these programs. It has been shown that household members cannot accurately recall participation in the food stamp program, and the participation of vulnerable individuals, often with disabilities, in these five programs makes collecting the data needed for this study an even more difficult task (Meyer and Goerge 2011).
Therefore, we rely on state agency administrative data. Just as Andrew Penner and Kenneth Dodge write that “it is difficult to imagine survey data tracking all of the classmates that a student had” (2019), it is difficult to imagine survey data tracking all of the service experiences of multiple household members. Beginning with more than three million Supplemental Nutrition Assistance Program (SNAP) and child protective services participants, we are able to connect their experiences in the juvenile and adult criminal justice systems, publicly funded treatment for mental health and substance abuse problems, and the child welfare system. Moreover, that connections among individuals are captured in these datasets allows us to identify individuals who constitute families in various combinations over a period of time. This, too, would be a challenge for survey research.
The administrative data allow us to provide detailed analyses of experiences as well as cost estimates. We show that, for low-income families participating in government programs, these five publicly provided services are concentrated in a fraction—23 percent—of families, and those families use 86 percent of the fiscal resources that are spent on these services for these families. This indicates a disproportionate concentration of resources and interventions. Given that too few resources are available to address the problems, additional clarity about these families’ experiences is necessary to develop appropriate public responses to avoid the ongoing cumulative effects of the conditions as well as policy and programmatic fragmentation. In this study, we only begin to tap the richness of the administrative data and provide a set of analyses that would guide additional policy and programmatic interventions for this large, vulnerable group.
BACKGROUND
Although health and human services systems are designed to address specific problems, individuals often experience co-occurring challenges and conditions that complicate attempts to address any single problem. For example, the parent of a child in foster care may also be receiving substance abuse services and another family member may be incarcerated or newly unemployed. These individuals live in the context of a family and a community, which determine, to a large extent, their current and future well-being. A premise of this article is that U.S. family policy, as operationalized in what government does for individual and families, does not incorporate the fact that families have multiple challenges as well as multiple assets.
Interventions designed to serve families with more holistic approaches can address these kinds of complex and interrelated concerns. “The family as a unit should be one of the basic foci of all interventions . . . individual services will be more effective when viewed in this context,” Andrew Selig argues (1976, 527). It is crucial to recognize families’ complex needs because these families require services that run both horizontally, across a variety of service domains, and vertically, across generations (Spratt 2011).
Just as familial and environmental factors can make it difficult to address an individual’s problem in a vacuum, so too improving family circumstances and dynamics can improve individual challenges. Family members can be positive influences on one another (Selig 1976). Qualitative work shows how a history of trauma or mental illness for a parent can adversely affect other family members and how therapeutic interventions that address adults’ histories can mitigate these adverse impacts (Krumer-Nevo 1998; Sacco, Twemlow, and Fonagy 2008). Families facing pressures from multiple directions are particularly important places to intervene because, left unassisted, they set the stage for children to grow up with “fewer chances to permanently fend off in a constructive way the negative consequences of life events that put pressure on them” (Tausendfreund et al. 2016, 9).
This article measures and characterizes the population of families that face multiple barriers and the ways those families interact with public-sector services. We present the results of a rigorous descriptive analysis using administrative data from several public agencies in Illinois—the Department of Human Services, the Department of Healthcare and Family Services, the Department of Children and Family Services, the Department of Corrections, and the Department of Juvenile Justice—to identify families that interact with two or more of those systems and to characterize those families and their needs.
Ultimately, we show that nearly 25 percent of families served by the state programs that address households and families have members involved in at least two of the costliest programs of the state, a group of families that accounts for 86 percent of the funding for these programs used by all the families in our study population. These families experience more and more severe problems than the other families served by these systems. But apart from the scale of their service use, these families are a diverse group; they are clustered in a few areas around the state and they engage with different combinations of the five programs we analyze.
In the nearly ten years since this work began, we have found that these findings are of significant interest to Illinois state leadership. Actionable applications of these results have been limited, however. The nature of federal financing, privacy concerns, information sharing, and the siloed structure of the public sector makes integrated operations at the scale necessary to address the multiple problems of family members out of reach (Potter et al. 2005).
This research was an important first step in quantifying at a systemic level the extent of cross-system overlap at the family level. Recognizing the heterogeneity of this population, however, we believe that additional analysis is needed to unpack patterns and subpopulations in these results for it to have a direct impact on policymakers’ decisions. In particular, the recent introduction of network analysis applications in the social sciences suggests promising new methods to uncover additional insights into this population. It is our hope that applying translational data science to explore the underlying patterns will suggest targeted opportunities for the public sector to integrate resources, data, and expertise across systems in specific applications, reaching families where these methods can make the biggest difference.
UNDERSTANDING MULTIPLE SYSTEM INVOLVEMENT
The concept of families that face multiple areas of challenge and engage with public services through a variety of means has a rich basis in literature from psychology, social work, sociology, and public policy. Various terms have been used to describe these families, but the most frequently used is multiproblem families.
The early literature on what would later be called multiproblem families developed in the 1950s and focused on the social deviance and isolation of these families, and particularly on chaos, disorganization, and dysfunction as their primary characteristics (Matos and Sousa 2004; Sousa, Ribeiro, and Rodrigues 2007). In child maltreatment literature, scholars developed the concept of multiproblem families when they began to focus on parental characteristics that increased the risks of harm to children, leading to an increasing awareness that child abuse could be a seen as a product of parental circumstances, experiences, and particularly traumas (Spratt 2011). Frack Sacco, Stuart Twemlow, and Peter Fonagy describe this as “transgenerational transmission of trauma” (2008, 34).
The multiproblem family label comes most directly from literature that classifies families with a certain number of defined barriers or challenges, such as mental and physical health conditions, problems in school, problems in the family, and legal problems (Mazer 1972; Sharlin and Shamai 1995). Different articles have considered the necessary quantity, variety, complexity, severity, and persistence of problems necessary to merit inclusion in the multiproblem family definition (Tausendfreund et al. 2016). The phrase multiproblem family does not have an agreed upon definition, making it difficult to compare descriptive research on these families across studies or to quantify incidence in the general population.
In particular, scholars disagree on whether poverty is part of defining multiproblem families. Ana Matos and Liliana Sousa argue that the interplay of problems within a family transcends class (2004). Shlomo Sharlin and Michal Shamai assert that the concept of multiproblem families is rooted in “poverty culture”—the dysfunction that is inherited across generations in these families represents “poverty personality.” Sharlin and Shamai agree that middle-class families can be multiple problem families, but only when they “have not managed to overcome the values and habits that characterize lower-class multiproblem families” (1995, 94). Some researchers take a middle approach, using household poverty and related characteristics (such as housing instability) as contributing problems in their definition of multiproblem.
In more recent years, the traditional multiproblem family concept as defined through a set of barriers and challenges has been criticized as a deficit view, focusing on what families lack and where they struggle rather than their strengths and opportunities. Instead, researchers are beginning to move toward language that focuses on the external circumstances and environments that affect these families—using terms such as stress, trauma, and recurring crises (Sousa, Ribeiro, and Rodrigues 2007). Similarly, Tim Tausendfreund and his coauthors point out that in the German context, scholars avoid the concept of multiproblem families because they think this label situates the problem at the family level and ignores the role the broader environment and systemic factors have to play, both in creating the problems the families face and in helping address them. Tausendfreund and his colleagues opt to use the phrase “families in multiproblem situations” as a compromise between respecting that environmental factors create multiproblem families and recognizing “the complexity of interactions between socioeconomic and psychosocial problems”—the interplay of systemic and familial factors that characterizes these families (2016, 5).
Another way of viewing multiproblem families, and an approach that is closely related to our work, is to define the families in the context of the systems they engage. Milton Mazer characterizes this as the conventional approach to defining multiproblem family: “[a family] that becomes known to social and welfare agencies because of the multiple and long-term services it requires” (1972, 792). Defining multiproblem families as those that engage with multiple systems emphasizes the need for, and corresponding lack of, coordinated care for these families (Sousa, Ribeiro, and Rodrigues 2007). However, it also runs the risk of defining problems based not on families’ true circumstances but instead on bureaucratic distinctions in service delivery (Spratt 2011). To the extent that systems engagement is used to define multiproblem families, they can be defined not only in the breadth of systems they engage, but also by the extent and complexity of support that they need, and the corresponding difficulty siloed agencies have in providing that support (Tausendfreund et al. 2016).
Some scholars have articulated that in addition to engaging a breadth of systems, multiproblem families have particular ways of interacting with those systems. They may be particularly likely to be referred to service systems by alerts from other systems, rather than by directly reaching out and seeking support (Matos and Sousa 2004). They also often fall into one of two groups, either resisting interventions and exiting systems quickly, or receiving steadily increasing and diverse services, public agencies becoming enmeshed in the life and network of the family (Matos and Sousa 2004; Tausendfreund et al. 2016).
A precise operationalization of the construct of participation in multiple programs is problematic because of how many ways it might be conceptualized. Ultimately, any particular characterization of multiprogram participation depends on the research question or policy issues at hand. However, across disciplines and definitions, the core idea that some portion of the population with a given challenge is struggling on multiple fronts at the same time remains clear.
For this analysis, we concentrate on the type, breadth, and relative cost of public-sector services received by the family. Our analysis is targeted specifically toward policymakers at the state and federal levels and is intended to help policymakers and public-sector managers understand overlaps in service provision and opportunities to design interventions around a high need portion of the population. We capture only a set of the problems and challenges families face and for which they have engaged assistance. To clearly distinguish between this approach and a traditional multiproblem family classification, we use the term multisystem family.
We characterize multisystem participation at the family rather than at the individual level because the family or household is the case, or the entire family is affected by any member participating in any of the programs.
However, literature is minimal on the definition of family in these multiple problem or multiple system engagement circumstances. The family or household unit is discussed as discrete and static although we know that is not the case, particularly for this population. As noted, there is no single way to operationalize this concept so there are no studies that characterize the incidence of multiproblem families in the general population (Spratt 2011).
DATA SOURCES
We use administrative data, data collected for administrative purposes (that is, service provision) by public agencies, for this analysis. These data include the universe of individuals and families at a point in time that engage with these public-sector services, the key population for our research goal. Survey data on public benefit receipt and engagement with social service systems is prone to underreporting (Meyer and Goerge 2011) and likely subject to social desirability bias. And, to identify the multiplicity of combinations, a population-based sample survey would be infeasible because of cost and complexity.
Cross-system analyses like this one require access to data from multiple agencies. Accessing the data from the relevant state agencies involves challenges (Goerge 2018). Also, linking data from disparate sources, which range from data manipulation to implementing record-linkage algorithms, entails technical challenges. The work described here was made feasible by Chapin Hall’s Integrated Database on Child and Family Programs in Illinois (IDB), which compiles microdata from Illinois, Cook County, and Chicago government agency sources over three decades (Goerge, van Voorhis, and Lee 1994; Kitzmiller 2013). Chapin Hall stewards and manages data for the agencies, and Chapin Hall researchers use the data to address questions approved by the data providers (government agencies) under strict conditions specified in data-sharing agreements. The multisystem families project was funded in part by the state of Illinois.
The database is a linked set of files (tables) rather than an online transactional system that would lend itself to rigorous in-depth exploration of an individual or family. Our focus for this analysis is to generally understand the program participation of individuals in families rather than the specific trajectories that individual or families might have within particular programs, which is also possible with the data in the integrated database.
One frequently mentioned limitation of administrative data for use for research purposes is that data quality may be inconsistent or poor, with duplicate records and fields left blank or entered incorrectly (Hotz et al. 1998). However, researchers generally agree that administrative data are most reliable for fields that are directly applied to the work for which the data were originally collected. This study analyzes program participation and benefit receipt. These topics are fundamental to program operations. As a result, we have confidence in the quality and validity of the relevant data points—a confidence shared by our agency partners, who use the same fields in their regular reporting. We do believe that the data include duplicate records, particularly when a person is engaged with the program, leaves, and subsequently returns. We address this limitation with our record-linkage methods, which include logic to de-duplicate individuals within the same program, as well as identifying the same individual in multiple programs.
We selected five areas of treatment or program participation (mental health treatment, substance abuse treatment, juvenile incarceration, adult incarceration, and child welfare) because together these services represent Illinois’ costliest areas of targeted social service expenditure. In fiscal year 2008, 29.5 percent of Illinois state expenditures were for Medicaid. A report from the U.S. Department of Health and Human Services’ Substance Abuse and Mental Health Services Administration noted that, in 2009, 10.4 percent of national Medicaid spending was for mental health treatment and 1.4 percent for treating substance use disorders (Substance Abuse and Mental Health Services Administration 2014). In fiscal year 2008, 3 percent of Illinois’ budget went to corrections (National Association of State Budget Officers 2009).
A general principle of our study is that once an individual is associated with another who has been in one of our five systems, the effects of that experience last a lifetime (Metzler et al. 2017; Shonkoff et al. 2012). The trauma experienced with one of the problems that led to the system involvement can clearly last a lifetime and lead to the need for additional services provided by the public sector, be they one of the five we examined or others, such as the need for workforce training, disability services, special education, or other such programs. Clearly, incarceration has lifetime effects on family members (Wakefield, Lee, and Wildeman 2016). Foster care has effects on both children and parents for a lifetime (Pecora et al. 2006). Substance abuse and mental illness similarly are challenges for an extensive duration, even if treated (Jordan et al. 2002; Teplin 1994).
The following data sources were combined for use in this research. For each source, we describe the population and time frame included.
SNAP participation. One of the primary drivers of our study population was the universe of households participating in the Supplemental Nutrition Assistance Program in Illinois from 1989 to 2008. We received this data as monthly extracts from the Illinois Department of Human Services, which administers food and cash assistance programs in the state.
Because SNAP assistance is provided at the household level (the assistance unit for SNAP is defined as the group of individuals in the home who shop and prepare food together), it is a good source, albeit not without error, of information about which individuals share a household. Case-level records are linked to the individuals who are current or former participants in the assistance case.
The SNAP data also contain monthly records of household addresses and their changes through time. We geocoded these records and used them to locate families spatially. Historically, mailing addresses were where program recipients received their benefits, so the quality of these addresses was considered very high. Since the introduction of an electronic benefit transfer system in 1997, that quality is less certain, although initial addresses are verified. However, because we use addresses largely to characterize patterns at regional and county levels, we do not think quality concerns about these data are so significant as to undermine the validity of conclusions.
Child welfare involvement. Child welfare service records from the Illinois Department on Child and Family Services (DCFS) were another source of data for our sample population, and these data also provided information about problems in the family represented by involvement with DCFS. DCFS tracks children and families receiving services. Child welfare service data were included from 1977 to 2008. These data included both cases where children were removed from the home and records about services provided to intact families, where the children remain in the home of their parent or parents and DCFS provides supports to the household. We also looked at substantiated allegations of abuse and neglect as recorded by DCFS. Abuse and neglect records were included from the early 1980s.
Incarceration. Incarceration records were included from both the Illinois Department of Corrections (adult incarcerations) and the Illinois Department of Juvenile Justice (juvenile incarcerations). Records were pulled from data on admissions and exits from 1990 to 2008—anyone who began or ended a spell of incarceration during those years would be included in the sample. These data sources reflect only confinement in state prisons, not time spent in county jails or detention centers or on probation. Including less severe measures of involvement with the criminal justice system would likely only increase the number of connections found between family involvement with criminal justice and involvement in other service systems.
Medicaid claims. We identified individuals receiving publicly funded mental health and substance abuse treatments through Medicaid claims records from 1994 to 2008. We also used claims data to look at intentional injuries.
Record linkage. One of the significant technical challenges involved in creating an integrated longitudinal database to conduct this research is accurately linking the records of individual clients across agencies and over time. This process is complicated by the fact that no single identifier, even social security number (SSN), can be completely relied upon to establish the identity of a client across the records of all agencies, although Social Security Act Title programs like SNAP do typically verify and validate SSNs. Probabilistic record-matching, first developed by researchers in the fields of demography and epidemiology, allows such linkages to be made reliably (Fellegi and Sunter 1969; Newcombe et al. 1959).
Probabilistic record-matching is based on the assumption that no single match between variables common to the source databases will identify a client with complete reliability. Instead, this approach calculates the probability that two records belong to the same client using multiple pieces of identifying information. Such identifying data may include name, social security number, birth date, gender, race-ethnicity, and residential address. When multiple pieces of identifying information from two databases are comparable, the probability of a correct match is increased.
Once a match has been determined, a unique number is assigned to the matched record so that each record can be uniquely identified. The end result of a record-matching exercise is a series of crosswalk files between each agency’s client identification number and a multisystem identifier (the new unique number assigned to the entity).
Chapin Hall routinely uses record linkage to create the IDB, which was used for this project (Goerge, van Voorhis, and Lee 1994). In the design of the IDB, each component dataset is unduplicated against itself, and then datasets are matched against each other. In the cross-system matches, one and only one match is allowed for each unique individual to reduce the chances of multiplying error.
METHODOLOGY FOR DEFINING FAMILIES
We began with two groups of individuals from which to build our population of households.
One population was drawn from the universe of SNAP families. However, to limit this to families that had received SNAP in a recent year, we chose an index population of all women in the SNAP population during fiscal year 2007–2008 who were eighteen to forty-five years of age. We included everyone in the index population and everyone who ever shared a case with an index person.1 The women who served as index individuals did not have to be on SNAP for the entire time, but needed to appear active at some point during that window. We chose these women because we believed they were most likely to have belonged to families with children. This selection also included nearly all families who received Temporary Assistance for Needy Families and nearly all families who received Medicaid with an income of below 130 percent of the federal poverty level, given that these families were highly likely to have received SNAP.2 This process yielded a pool of 318,927 families.
The second population was all families receiving child welfare services at any point from 1977 to 2008, a population that has been shown in the literature to have many additional problems other that the placement of children in the foster care system, and the effects of the maltreatment and foster care, in most cases, have an impact on their future well-being and service use (Metzler et al. 2017). This process yielded 286,408 families.
The key analytic unit is the family network. This family is defined through the analytic concept of a supercase, a connected component of the graph of all individuals in these two populations where edges represent shared membership in a case. All individuals who share a case are grouped in the same supercase and individuals in a supercase do not share cases with individuals in any other supercase.
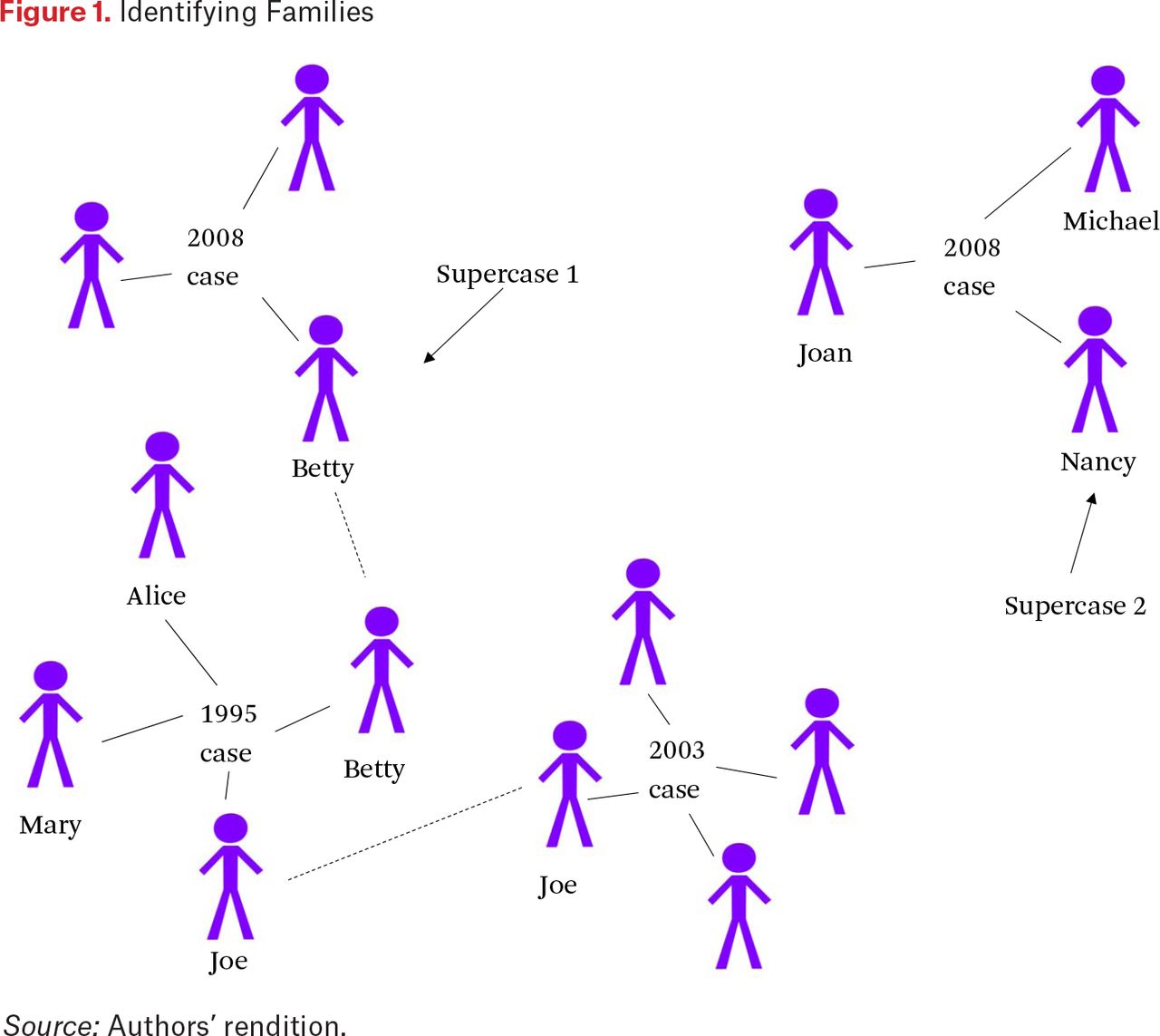
Figure 1 demonstrates this process at the individual level with two example cases:

Identifying Families
Betty is an index individual from the SNAP data (a woman between the ages of eighteen and forty-five who received SNAP during fiscal year 2007–2008). We find all public assistance cases associated with Betty going back to 1989. She was a child in 1995 on a case with her mother (Alice) and siblings (Joe and Mary); they all become part of her SNAP supercase. Similarly, all individuals on her SNAP case during 2007–2008 are part of her SNAP supercase. Finally, her brother Joe has a SNAP case in the early 2000s with his family—because Betty and Joe were on the same SNAP case in 1995, this case is also considered a part of the same family network.
Nancy is a second index individual from the SNAP data. She is on a SNAP case in 2008 with her children, Michael and Joan. That case is the only public assistance case any of them have been on in Illinois since 1989, so the three people on this case form a discrete family network.
We completed a similar process with child welfare cases and then combined the two groups of supercases into a single, unified set of supercases, representing our ultimate sample of families. Altogether, we identified 502,165 discrete family networks in our sample—the union of the SNAP and child welfare case populations. The result of this process was a dataset containing the unique cross-system identifiers of all the people associated with these families in either public assistance or child welfare data, along with their corresponding assigned supercase or family identifier. We linked information about the five problem domains (child welfare, adult incarceration, juvenile incarceration, mental health services, and substance abuse services) at the individual level. This information was easily aggregated to the family level for our primary results.
Limitations. We believe that our results both are representative of the families engaging with public services in Illinois and are useful for informing human services policy and practice, but we highlight a few limitations stemming from our data and approach.
Ideally, we would use either the full population of Illinois families or the full population that encountered any of the five systems as the base population. The nature of the administrative data available to our analysis significantly limited our opportunities on this point, however. In particular, because our research question is about families rather than individuals, we needed to form our base population from datasets that captured populations of families. Without access to vital records, tax returns, or decennial census records, there is no comprehensive population-level database of families. David Grusky, Michael Hout, Timothy Smeeding, and Matthew Snipp’s proposed American Opportunity Survey would provide exactly the kind of base dataset needed for this work in the future (2019). The next best option would be a base population of all families who touched any of the five systems, but only the child welfare system captures relationships among family members in its participation data. We thus used the universe of child welfare families combined with the universe of food stamp families (to provide a broad sample of Illinois families) to comprise our base population.
The limited nature of our base population limits the interpretation of population-level statistics. However, a primary goal of our work is to provide policymakers and program administrators with evidence about the populations they encounter across systems. For this purpose, being able to characterize the rate of multiple system involvement within a group of families that routinely interact with the state through two of its largest human service systems is of great value. Although using our results to define the prevalence of multisystem families in the general population is difficult, the results demonstrate the high rates of multiple system involvement among the very families with whom the state already works.
To contextualize the extent to which our population is representative of the state of Illinois, we can compare our total count of families (502,165) with the estimates from the 2008 American Community Survey (ACS). The 2008 ACS counted 3,138,757 family households in Illinois (households containing at least two people related by marriage, birth, or adoption), of which fewer than half are families with children younger than eighteen. Our sample included households from the child welfare system and the households of women of childbearing age from the SNAP population, so the number of families with children is probably a better proxy than the overall population of families. When we compare with the population of low-income families, the numbers are much closer: 400,751 families were under 130 percent of the federal poverty line in 2008 in Illinois, including 311,900 families with children younger than eighteen. Although it is difficult to compare too precisely our universe of families derived from decades of administrative data to point-in-time populations, it is evident that our sample captures less than one-third of Illinois families overall but likely represents an extremely high proportion of low-income families.3
Although the proportion of the overall Illinois population represented in our universe is small, that our population is centered on households living in poverty means that the count of families in our sample in certain communities is very close to the population-level count. This allows us to infer some community-level conclusions about the percentage of all families that are multiple system involved, even though we cannot make those conclusions for the full state.
We think using networks to capture families appropriately represents the concept of a family unit. The median supercase (family) size was four family members; the mean was 5.9. However, opportunities exist to further refine this approach in subsequent analyses—in particular, by incorporating temporal information more granularly, to better distinguish close family relationships (that is, people who lived together at more time points). As family size increases, families are more likely to include individuals with various points of system contact. It would strengthen the findings to confirm that these additional contacts are not from individuals who were only tangentially connected with the family.
Another limitation that derives from the use of administrative data is that the sources of data that identify biological relationships among family members frequently omit fathers. Birth certificate data is the single most important source of information needed to obtain a more accurate construction of family units. Although our method for identifying families attempted to include as many adult males as possible, we do not believe that we identified them particularly well. One indicator for that is that only 33 percent of the adults in the corrections population were connected to the families we identified. We believe that this is our largest source of error and that it artificially decreases both the number and percent of multisystem families in our sample and the costs attributed to them.
METHODOLOGY FOR MEASURING SYSTEMS ENGAGEMENT
For the group of families described, we tracked receipt of five areas of service, each of which represented a problem facing the family: child welfare, adult incarceration, juvenile incarceration, mental health services, and substance abuse services. Family members are exposed to individual mental illness, alcohol or substance abuse problems, incarcerated adults or juveniles, and child maltreatment serious enough to require out-of-home placement or are themselves beset with these problems. We defined multisystem families as those that engaged with two or more of these areas of service.
We estimated costs for each service differently depending on data availability. Our goal was not to arrive at a precise accounting of all costs, but to have an estimate consistent across family service and program participation combinations that would allow for relative comparisons. For the Departments of Corrections and Juvenile Justice, we began with the yearly cost of incarceration per individual across all facilities, reported by those departments, and calculated a per diem amount. We multiplied that amount by the numbers of days incarcerated for each individual and summed that over all of the individuals in the family. For youth served by the Department of Juvenile Justice, we also calculated the cost of after-care similarly. For substance abuse, mental health services, and other Medicaid-reimbursed services, we used the paid claim amount for each service received, summing all paid claims for an individual and then for the family. For child welfare costs, we calculated the cost of substitute care per day and applied that to the number of days experienced by each child in the family. For Medicaid and child welfare costs, we do not include administrative costs, which are included in the Corrections and Juvenile Justice estimates. Estimates of Medicaid administrative costs range from 2 to 5 percent (Yong, Saunders, and Olsen 2010). Estimate of administrative costs for foster care is 35 percent (Stoltzfus, Stohl, and Seibold 2011). Given other sources of error described in the limitations section, these would not change the nature of our results greatly.
RESULTS
Of the 502,165 families in our sample, 23 percent were multisystem families, and these families accounted for 86 percent of the funding for health, mental health, criminal and juvenile, and child welfare needs for the full sample of families. Another 34 percent of families received services in one of the five areas and accounted for the remaining funds. Table 1 presents these populations in more detail.
Total Engagement by Families in Sample
Table 2 presents the five most prevalent combinations of the programs studied. These combinations account for 75 percent of all multisystem families. The most common is mental health services and substance abuse treatment (25.0 percent of multisystem families). The second most common is child welfare involvement and mental health services (18.2 percent). The third most common is child welfare involvement, mental health services, and substance abuse treatment (11.6 percent). This is not surprising given that most families in the child welfare system have challenges related to mental illness and substance abuse; these conditions often motivate entry into the system. The fourth most common is child welfare involvement, adult incarceration, mental health services, and substance abuse treatment (9.8 percent). The size and relative intensity of services received by this group presents opportunities for a particularly targeted focus on them, as their cross-system penetration is quite significant and suggests multiple health, psychological, and social challenges.
Top Five Combinations of Program Use by Multisystem Families
Of the funding that supported the participation of the multisystem families in these programs, 34 percent was for child welfare service costs, 23 percent for mental health services, 21 percent for adult corrections, 9 percent for substance abuse treatment, and 7 percent for juvenile incarcerations. We also tracked expenses for long-term care paid for by Medicaid since mental health services and substance abuse treatment account for a significant portion of diagnoses of individuals using long-term care. It accounted for 5 percent of the costs for multisystem families (Simon, Lipson, and Stone 2010).
These findings cannot be interpreted as the prevalence of families with multiple challenges in the general population. Our base population was SNAP- and DCFS-involved families, so we assume the rate to which multisystem families are reflected in our sample is significantly higher than it would be in the general population. Furthermore, we measured rates of system involvement for treatment and services, not the prevalence of mental illness, drug abuse, child abuse and neglect, and so on in the population. An uncertain number of other families in the state with the same problems have not received state services.
However, these findings clearly demonstrate that a significant minority of the families that engage with the state through large human service programs are engaging in multiple areas—and they are major cost drivers within those areas. Their cumulative use of these programs greatly exceeds that of the one-system families because the duration of participation is built into the cost calculation. It certainly could be the case that this could not be so disproportionate if the one-system family members were participating in the one system in a more intensive way than members of the multisystem families.
We believe our method of defining supercases effectively captures familial networks, but recognize that it is unlikely that some of the larger “families” constructed from the administrative records are groups that live in the same household at one time. To test the sensitivity of our results to this definition, we restricted family size to a maximum of ten. Looking only at this universe of more traditionally sized families, the percentages do not change substantially. Where 23 percent of all families are multisystem families, 17 percent of the traditionally sized families are multisystem families. We expect this rate to be a little lower because larger families are more likely to be engaged in multiple ways.
Multisystem families experience more and more severe problems than the other families these systems serve. When we compare the multisystem families with other families on problems that go beyond the components of our definition, including inpatient mental health and substance abuse services, substantiated allegations of abuse or neglect, and cases of intentional injury, we find these problems are more frequent and severe for the multisystem families.
More than 56 percent of the multisystem families have experienced an inpatient hospitalization for either mental illness or substance abuse treatment. In fact, 25 percent of all multisystem families have experienced inpatient hospitalization for both reasons.
Although not one of our five primary programs, we analyzed data on family violence and found 73 percent of the multisystem families had had a substantiated investigation of abuse or neglect. This is not just a product of the families with child welfare cases; 63 percent of the families that did not receive child welfare services have had a substantiated investigation of abuse or neglect. Finally, nearly 49 percent of multisystem families have a member who has experienced an injury diagnosed as intentional (according to International Classification of Diseases) for which they received health care reimbursed by Medicaid. Altogether, nearly 82 percent of multisystem families have either a substantiated report of abuse or neglect or an injury due to violence.
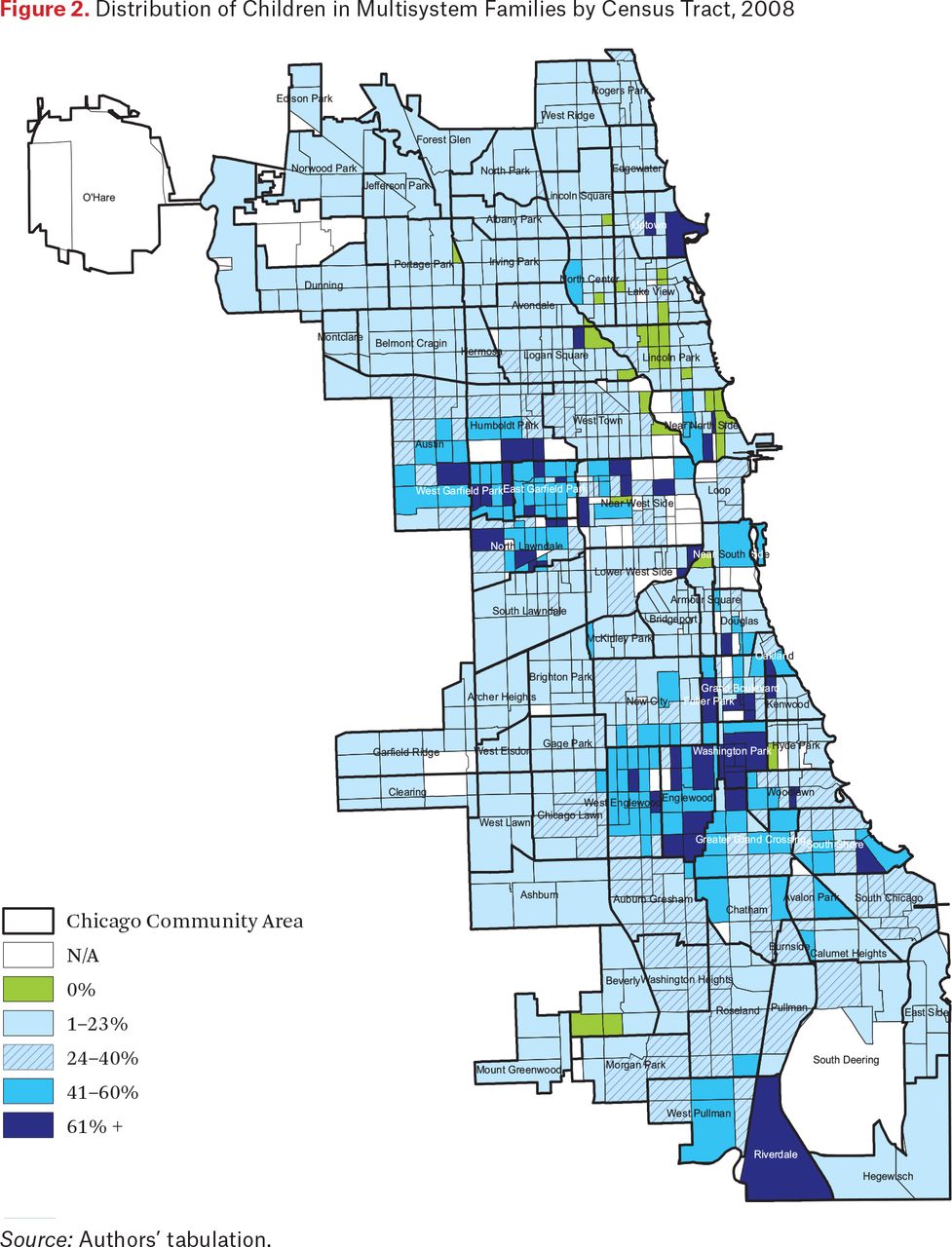
The multisystem families are geographically concentrated. Figure 2 shows the percentage of children living in multisystem families by census tract in Cook County.4 We see that a relative few areas of Chicago exhibit extremely high percentage of children living in families who participate in multiple systems. In a dozen census tracts in Chicago, more than 60 percent of the children, those seventeen years old and younger, live in multisystem families. In a smaller number of tracts, which we do not identify, more than 90 percent of the children live in multisystem families.

Distribution of Children in Multisystem Families by Census Tract, 2008
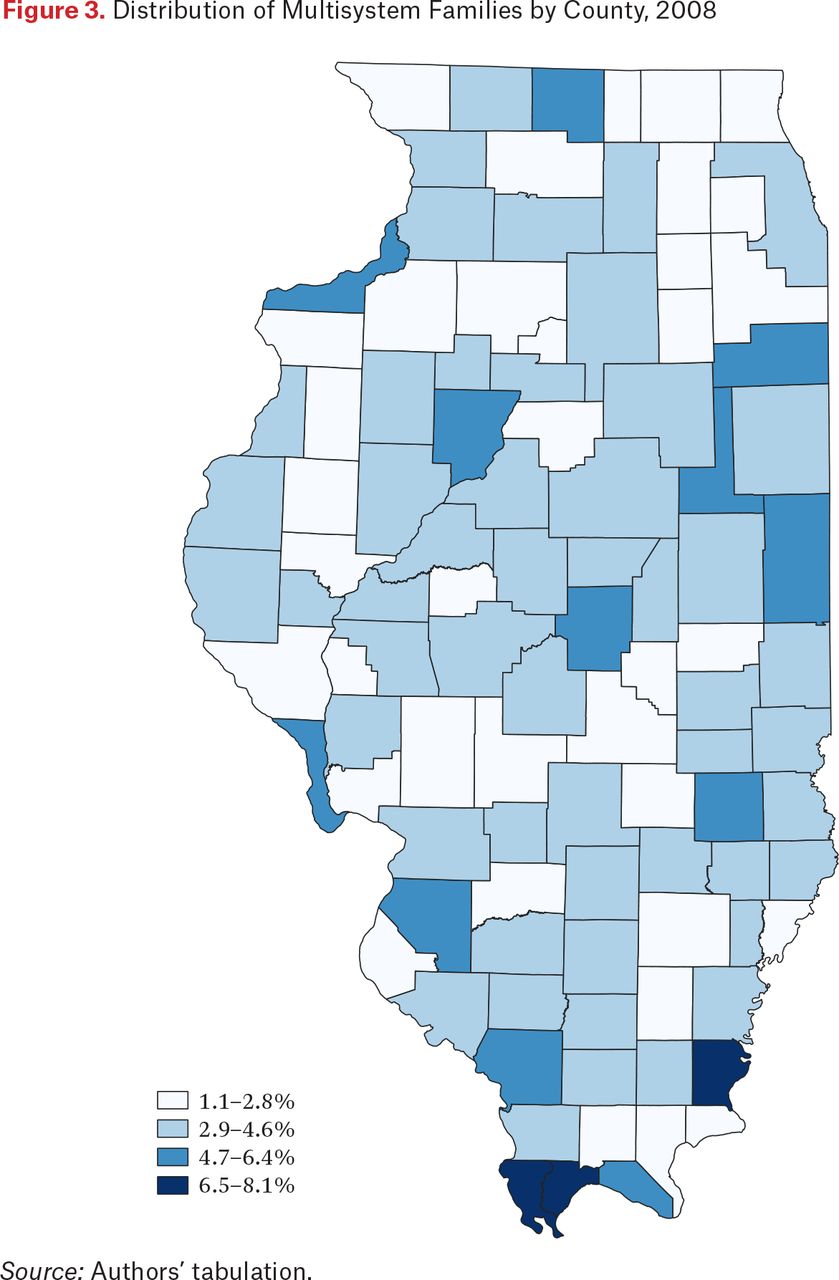
To understand the variation across the state, we calculate the percent of households that are multisystem families by county (figure 3). This is a crude measure (see earlier discussion of comparison with census data), but it does show that proportionately more multisystem families are in counties with smaller urban areas and some of the poorer urban counties. This information provides insight for where policymakers might concentrate efforts. Given the effects of living in these households on children, the impact on schools, the health-care system, public safety, and law enforcement in the areas where these families cluster is significant.
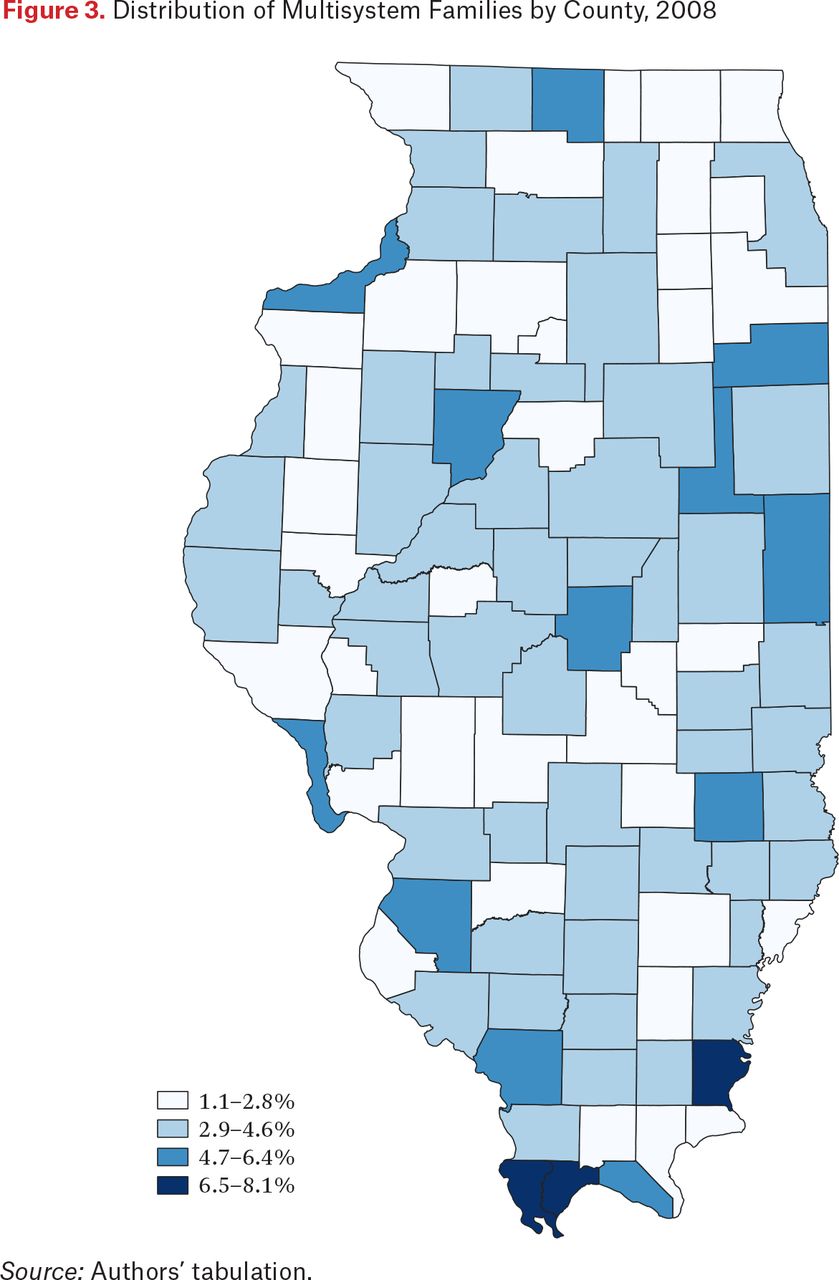
Distribution of Multisystem Families by County, 2008
The geographic clustering of multisystem families suggests the possibility of using geography to target interventions toward these families. It also highlights the variation within multisystem families; these families are concentrated in Chicago and in southern Illinois, but given the very different geographic context it is likely that the specific barriers those families face and the interventions needed will vary. This relates closely to our next finding.
Multisystem families are heterogeneous. As we explore underlying trends around service provision, we must recognize the significant diversity in the quantity, type, and severity of challenges multisystem families face. Table 3 shows the size and percentage of the multisystem population engaged with each service area.
Areas of Systems Engagement
Nearly 94 percent of all multisystem families have received mental health services, and about 60 percent have engaged with services in just two of the five areas, so more than half of multisystem families are multisystem because they receive treatment for mental illness and one of the other five. The most common combination is mental health and substance abuse services, which characterizes 25 percent of multisystem families. Another 18 percent are engaged with both mental health and child welfare systems.
The other 40 percent engaged with three or more of the five service areas. In particular, juvenile justice, adult corrections, and substance abuse are unlikely to exist in isolation. Of families with juvenile justice engagement, 96 percent are multisystem. Of those with adult corrections engagement, 85 percent are. For substance abuse, the corresponding rate is 95 percent. By contrast, smaller proportions of the child welfare–involved population of families (57 percent) and the population of families receiving any mental health services (49 percent) were multisystem families.
Although the juvenile justice-involved population is much smaller than the groups engaged with the other service areas, these families overlap, particularly the group engaged with adult corrections. Specifically, 68 percent of multisystem families with members who have experienced juvenile corrections also experienced adult corrections, whereas about 40 percent of families without juvenile correction experience have had adult correctional experience. Conversely, 11 percent of multisystem families with adult correctional experience have juvenile correctional experience, and 4 percent of families without adult correctional experience have juvenile correctional experience. The correlation is therefore clear of adolescents and adults being incarcerated in these families, either from one individual (perhaps a parent) who was incarcerated and another (perhaps a child) being incarcerated, or from the same individuals being incarcerated as both a child and an adult.
Multisystem families that have members who have been in adult corrections are less likely to have family members who have received mental health services or substance abuse treatment of any kind. For example, 40 percent of families with adult corrections experience also experienced outpatient mental health care, relative to 74 percent of those without adult corrections experience. This may show that families excluded from particular services, such as substance abuse or mental health services, may be the most likely to be involved in the criminal justice system.
Just as the concept of a multiproblem or multisystem family is difficult to isolate across studies, our results demonstrate that the lived situations of these families can be highly variable, even within a single definition.
DISCUSSION
Many families with multiple system involvement live in Illinois, and providing services to those families consumes a significant amount of state resources. Although policymakers and researchers often analyze a single problem, it is obvious that many families at risk must simultaneously address the challenges of economic support, parenting, childcare, health care, handicapping conditions, violence, and substance abuse. It is also clear that all of these issues are related in various ways. Until we can adequately describe the needs of families across these areas, we will not know whether family policy and service programs are meeting the needs of the population.
These findings were shared with policymakers and program administrators shortly after the initial data analysis was concluded in the late 2000s and have sparked conversations and interest across the intervening years through multiple administrations. However, it has proven difficult to implement programs and strategies to address the needs of these families.
Existing solutions are not simple and perhaps more local than at the state or national level (Corbett et al. 2005), although federal rules and regulations are often blamed for the problem at the local level. The problem in part stems from the continued operation of multiple programmatic and agency silos in government designed to deal with a limited set of problems and the inability of these agencies and programs to coordinate efforts, resulting in practitioners often not having the service resources or skills to access the array of interventions a family and its members might need.
As the demand for services changes and the perceived need for services has increased, considerable discussion and effort have focused on the notion of comprehensive service systems for children and families. Service providers often talk about how their cases are becoming more severe and how they lack the service armature to address child and family needs. This perception has led to many attempts at service reform, often without testing the magnitude of the population’s needs. The goals of coordinated or integrated service systems are to weave together the programs and services that cut across service sectors and address the multiple needs that children and their families may present. Integration can occur at the financing, administrative, or casework level, but regardless of the particular strategies, the goals are to address the multiple problems of children and families in a comprehensive manner that increases the likelihood of improved well-being for the entire family.
The term silo has perhaps become overused, but probably because it is so apropos when talking about government services. The use of the term reflects a desire to make “the inability to share information and integrate system activity” more concrete (Roberts 2011, 677). The siloing begins with the federal government and the multitude of programs with similar goals across multiple agencies. These silos reflect and further reinforce federal policy in their own ways at the state and local levels through the separation of programs into separate agencies. They reflect the fragmentation that results from spreading the authority for programs across levels of government and across agencies within government (Farhang and Yaver 2016). Given what we have found, why would all resources related to the problems addressed in this study not be housed and integrated under one agency? Although some states do bring together multiple federal programs into a single agency, they often must still be managed separately and reported on separately, and the data belonging to each can often not be shared across these programs. For example, substance abuse and mental health professionals, child welfare caseworkers, counselors for ex-offenders, and parole officers all sit in separate agencies, often at different levels of government. Therefore, programmatic silos exist at all levels of government and these levels themselves are silos, preventing effective communication and collaboration across levels of government. To be sure, the private and advocacy sectors have their own silos (Civic Caucus 2009). Each condition or diagnosis has a special interest group devoted to competing with others to gather greater shares of the scarce resources.
Unfortunately, as mentioned, the data are also siloed, often under the rubric of privacy or confidentiality. Even with twenty-first-century technology, decades-old rules and regulations restrict data-sharing within the public sector, across agencies and levels of government, not to mention with researchers who are attempting to create better evidence on what works or simply a better understanding of what the problems are. Although computational advances have made it easier to do this work, significant challenges to anything approaching real-time implementation remain, including the resource investments necessary to build the infrastructure, the challenge of maintaining data quality, and the intensiveness of the required calculations. There are better ways to spend the resources involved than in building these large systems, especially given the challenge of implementing interventions to address these findings.
In short, integrated service delivery on a large scale is quite difficult. The technology and data needs to continually inform this work are complex, and the systems that manage these programs are not designed for integrated practice.
RECOMMENDATIONS FOR RESEARCH AND PRACTICE
Now that we better understand the scope and scale of the problem at a systemic level, we believe that further research can convert these findings into more actionable insights with a specific focus on unpacking patterns and subpopulations in the results. Our hope is that subsequent work will yield more tangible results that can help bridge the gap between data and action. The following list includes suggested areas of inquiry.
Timing of engagements. The results include engagements with the systems from as far back as 1990, and we do not consider temporal patterns in systems engagement—which engagements overlap or occur in close succession. We believe that each of the areas explored (mental health, substance abuse, incarceration, or child abuse or neglect) has a lasting impact on the family and the individuals in it. However, further analysis that looked at the relationships in these engagements over time could provide more insights about how and when challenges cluster. As mentioned, looking at timing more closely in the context of refining family definitions could also provide more detail about the types of families included in this analysis.
Individual versus family problems. This study aggregated engagements to the family level. Multisystem families in this study could have one individual in the family who engaged with services in all five areas or five individuals with one point of engagement each. More investigation could illuminate whether a few individuals within families account for a large number of the system engagements.
Magnitude of problems. The study counted multiple instances of engagement with the same system as a single engagement. For example, in a family with ten members, each family member could have received mental health treatment. In another family of ten, one member might have received mental health treatment. In this study, both examples would count as one point of engagement within a family. Similarly, one individual may have received a service once and another person may have received multiple services for the same problem over the course of years. Further research could discriminate among these cases.
Characterization of individual problems. Data are available that would allow for a more detailed picture of problems. For example, within records of mental health treatment are records of different diagnoses. The policy and program response to a family with an instance of clinical depression may be different than one with a schizophrenia diagnosis.
Networked service delivery. This research used familial networks rather than individuals as the unit of analysis. Are there implications for intervention design to consider service delivery via networks as well? Recognizing that families are themselves nodes within broad community networks, is it possible to move from serving even multisystem families to designing interventions for multisystem communities?
TECHNICAL RECOMMENDATIONS
Throughout this article, we note both the unique opportunities to conduct an analysis of this nature using administrative data and the unique challenges, resources, and limitations needed to do that analysis. We close with a few technical recommendations for improving the accessibility of administrative data and creating opportunities for further analyses of this type (see also Goerge 2018).
Develop secure data collections and the infrastructure to manage them. The kind of data preparation and record-linkage work that went into the development of our dataset was a high initial investment. Updating and expanding the data continues to be resource intensive, but the cost of maintaining and updating these kind of collections is much lower than the initial development. Developing infrastructure that allows data to be securely collected, integrated, and responsibly managed for research and analytic purposes will mean that the benefits to this sort of data preparation can be shared more broadly. This would also create opportunities to expand the rigor and complexity of data preparation. For example, having worked with these data as families, we now hypothesize that using family relationship to inform our record linkage might improve the original data integration process.
Train public-sector personnel in evaluation, research, and analysis. The effective use of data in the public sector, and the availability of data for ethical research, requires agency leaders who understand the value of evaluation and research. It also requires staff who are comfortable using and interpreting the results of research and comfortable using data in simple analyses to better understand programs.
Familiarize researchers with state information systems and databases. Many of the limitations and challenges of administrative data stem directly from the way data are collected and stored over time. Researchers who understand these systems can better interpret findings.
Encourage ongoing collaborations among state and local agencies and researchers. For investment value in administrative data to be maximized, program staff and researchers need to partner to bring a depth of understanding and interpretation to the data. Such a partnership will promote both better research and the translation of the research into better services to vulnerable families.
FOOTNOTES
↵1. This index approach allowed us to limit the study to families that had received SNAP in a recent year while still taking advantage of the rich historical SNAP data allowing us to identify the extended family networks of the index participants.
↵2. An alternative was to choose all families in Medicaid, but because Medicaid eligibility is at the individual, rather than household, level, this would have reduced the number of poor nonparent-nonchild individuals included in our populations. Using SNAP allowed us to represent the universe of extended family members who live together.
↵3. All numbers are from the Census Bureau’s American FactFinder based on the results of the 2008 ACS one-year estimates (https://factfinder.census.gov).
↵4. Figures 2 and 3 reflect where families lived in 2008.
- © 2019 Russell Sage Foundation. Goerge, Robert M., and Emily R. Wiegand. 2019. “Understanding Vulnerable Families in Multiple Service Systems.” RSF: The Russell Sage Foundation Journal of the Social Sciences 5(2): 86–104. DOI: 10.7758/RSF.2019.5.2.05. We gratefully acknowledge Cheryl Smithgall, Roopa Seshadri, and Peter Ballard for assistance with the data preparation and analyses described in this article. We also thank our agency partners at the Illinois Department of Human Services, Illinois Department of Child and Family Services, Illinois Department of Healthcare and Family Services, Illinois Department of Juvenile Justice, and Illinois Department of Corrections for their collaboration and support, which made this study possible. Direct correspondence to: Robert M. Goerge at rgoerge{at}chapinhall.org, 1313 E. 60th St., Chicago, IL 60637; and Emily R. Wiegand at ewiegand{at}chapinhall.org, 1313 E. 60th St., Chicago, IL 60637.
Open Access Policy: RSF: The Russell Sage Foundation Journal of the Social Sciences is an open access journal. This article is published under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.