
Abstract
Could we combat poverty by reducing the number of unintended and nonmarital births? This article proposes a federal policy that would provide all women with information about, and free access to, a range of contraceptive services, including long-acting reversible contraceptives; reviews what it is that we do and do not know; discusses several dynamic selection mechanisms by which this policy could lead to poverty reductions; stresses the need for longitudinal randomized intent-to-treat pilots that would provide causal evidence on whether this policy would in fact reduce poverty; and provides rough estimates of take-up, costs, and benefits were such a policy to substantially increase the use of highly effective contraceptive methods.
- nonmarital fertility
- unintended pregnancies and births
- long-acting reversible contraceptives
- dynamic selection
- longitudinal intent-to-treat trial
- poverty reduction
In this article we discuss whether a federal policy providing all women with information about, and free access to, a range of contraceptive options, including long-acting reversible contraceptives (LARCs), could lower the number of unintended and nonmarital births, and whether this would reduce poverty in the United States. LARCs have attracted recent attention but also considerable controversy (see, for example, Gomez, Fuentes, and Allina 2014; Gubrium et al. 2016; Northridge and Coupey 2016; Sawhill 2014; Secura 2013). For these reasons, we (1) provide details about a potential federal policy that would provide all women with information about, and free access to, a range of contraceptives, including LARCs; (2) review what we do and do not know from research and policy efforts to date; (3) discuss specific behavioral mechanisms by which LARCs could have concrete anti-poverty effects, including dynamic selection mechanisms that, to our knowledge, have not been previously emphasized; (4) stress the need for longitudinal randomized intent-to-treat pilots, which would provide the sort of causal evidence needed to determine whether such a policy would, in fact, reduce poverty and increase well-being, particularly in disadvantaged segments of the U.S. population; and (5) provide rough estimates of take-up, costs, and benefits were such a policy to substantially increase the use of highly effective contraceptive methods by women during their reproductive years.
Modern contraceptive technologies now provide ways for women and couples to avoid a pregnancy, thus allowing considerable, albeit incomplete, control over the timing and number of births. Although some, on religious or other grounds, prefer not to contracept, most Americans have used some form of contraception at some point in their lives. But effective contraception often requires effort—taking a pill every day or reaching for a condom in the heat of the moment. And relative to other advanced industrialized nations, the United States is unusual in having large numbers of unintended pregnancies and births.
LARCs provide a way that we could level the playing field by providing women with a safe and highly effective method of contraception that requires little effort. For example, an intrauterine device (IUD) requires minimal effort to use save for an initial visit to a doctor or health-care provider for initial insertion, coupled with semiannual check-ups to ensure that the IUD remains in place. LARCs are also reversible: those desiring to become pregnant need only to visit a health-care provider to remove the implant or IUD.
As a practical matter, any policy addressing childbearing, pregnancies, contraception, and sexual activity must also contend with the fact that these issues are often highly controversial. Yet, from a policy standpoint, it is also the case that these issues involve private behaviors that are simultaneously central to the public good. When, whether, and with whom to have a child are profoundly personal decisions that society leaves for individuals—whether single, married, divorced, or remarried—to decide for themselves. Yet children represent the future of any society and thus ensuring the well-being of current and future generations is inescapably a critical public good. Finally, we think it critical that policy discussions on these issues cannot and should not ignore a historical legacy in which advocates for birth control in the United States also encompassed a eugenics movement that led to the forced sterilization of targeted groups of women—minorities, immigrants, the “feeble-minded,” and the “sexually promiscuous” as evidenced by a nonmarital birth (Gordon 2002; Kline 2002; Stern 2005; Lombardo 2008).
For these reasons, we think it especially important to state an explicit set of principles that, in our opinion, should guide policy:
Policy should both acknowledge and respect the childbearing preferences, choices, and decisions of individuals.
Policy should likewise both acknowledge and respect the fertility-related preferences, choices, and decisions of individuals, that is, the preferences, choices, and decisions that may or may not lead to a birth.
Policy should, to the extent possible, be responsive to the changing needs and circumstances of individuals.
The proposed policy of providing information about, and free access to, a range of contraceptive methods follows these principles. It thus acknowledges and respects the preferences of those choosing to delay sex until marriage. But it also acknowledges that the majority of women will in fact not delay sex until marriage by further acknowledging, respecting, and addressing the contraceptive needs that may result from such a choice.
The policy we propose takes as given that the preferences and choices of individuals will vary on these and other fertility-related matters. What it does not do is to seek to influence or alter preferences, instead focusing on eliminating barriers such as cost or a lack of information that may prevent individuals from achieving their contraceptive preferences and goals.1
The proposed policy would achieve these goals in the following ways.
For women with health insurance coverage from an employer-provided plan, the proposed policy would require insurers to provide, at no cost, counseling and access to U.S. Food and Drug Administration–approved contraceptive methods and services when prescribed by an in-network provider.
For women who lack health insurance coverage from an employer-provided plan, the proposed policy would require insurers and other providers to provide, at no cost, the same counseling and access to FDA-approved contraceptive methods and services as provided by employer-provided insurance. Providers would be reimbursed for these services at the same rate as that for employer-provided plans.
This policy thus puts decisions about these matters in the hands of the individual. It treats with equal respect the decision by some to delay sex until marriage and the decision by others not to do so. It likewise treats with equal respect the decision by some to contracept and the decision by others not to contracept. It seeks to remove from all such decisions barriers such as lack of information or cost, thus allowing those who wish to contracept to choose a course of action that best suits their needs. The goal is thus to level the playing field by providing equal contraceptive access to all women, regardless of income, health-care coverage, or marital status. But as was the case for federal policies that sought to encourage sexual abstinence or to promote marriage, states would be allowed to opt in or to opt out, with this policy thus providing federal funding only to those states choosing to participate.
The proposed policy is also far less costly than many other potential and existing policies aimed at reducing poverty, thus providing policymakers with the opportunity to combine it with other policies, including those considered elsewhere in the two RSF issues on this subject. For example, estimates of the direct cost of providing no-cost contraception through an employer-provided insurance plan range from a 1998 estimate of $21 per enrollee per year by Buck Consultants, a 2007 estimate of $41 per enrollee per year by Price Waterhouse, and a 2011 estimate of $26 per enrollee per year by the Actuarial Research Corporation (Bertko et al. 2012). These authors also note that these estimates of premium costs are very likely too high because such estimates ignore the costs to employers of unintended pregnancies such as the cost of prenatal care, complications during pregnancy, and delivery. When these costs are included, “the net effect on premiums is close to zero” (Bertko et al. 2012).
Perhaps most importantly, the proposed policy provides a simple message to women—that of no-cost, universal access to contraception. Currently, contraceptive access, particularly for poor women, is highly unsatisfactory from a policy perspective: the current U.S. system poses the most barriers precisely to those most likely to have the greatest unmet contraceptive needs.
BACKGROUND
Although any potential policy concerning contraception and other fertility-related behaviors will affect the lives of all women making decisions about whether, when, and with whom to have a child, policies to date have placed a particular emphasis on nonmarital pregnancies and births. For example, the 1996 Personal Responsibility and Work Opportunity Reconciliation Act (PRWORA) declared that the “prevention of out-of-wedlock pregnancy and reduction in out-of-wedlock birth are very important Government interests” and directed states to “establish goals and take action to prevent and reduce the incidence of out-of-wedlock pregnancies” and to establish numerical goals for reducing the proportion of births that occur outside of formal marriage (Section 402).
We also know that in the United States, childbearing outside of marriage has become an inextricable part of the lives of many poor mothers and their children, as a large and growing body of empirical research has amply documented. There is, however, far less consensus on whether nonmarital childbearing is a cause of disadvantage, with this question being the subject of considerable and continuing debate (see, for example, Geronimus 1991; Mayer 1997; McLanahan and Percheski 2008; McLanahan, Tach, and Schneider 2013). What we do know is that such families are very often fragile and poor. We know that childbearing outside of formal marriage now encompasses two out of every five births in the United States and that much of the increase in recent decades is due to births to unmarried parents who are living together. We know that these unmarried parents typically have very high hopes for themselves and the child at the time of the child’s birth. Yet we also know that this “magic moment” is often fleeting: only three in ten unmarried parents are still together, on average, five years after the child’s birth (McLanahan and Beck 2010; Gibson-Davis 2014). And we know that many of these single-mother families are poor and that poverty is especially acute among never-married mothers. These stylized facts have led to concern within both the research and policy communities.
Could a policy providing universal and no-cost contraception reduce nonmarital fertility in the United States? And would such reductions in turn lead to improvements in the well-being of those segments of the U.S. population most likely to be poor? It is important to note that the research and policy literatures do not provide firm answers for these and other questions. Because of this, we turn to theory, discussing behavioral mechanisms involving dynamic selection via job and relationship churning, stress, and employer learning that suggest how improved contraception could plausibly have concrete anti-poverty effects and thus improve the lives of those most at risk of poverty. But given our current state of knowledge, it will be especially important to conduct longitudinal randomized intent-to-treat pilots that would provide the sort of evidence needed to determine if the policy proposed here would in fact be successful in achieving its intended goals.
The policy we advocate would not target LARC use per se, but would instead provide information about, and free access to, a range of FDA-approved contraceptive methods. For a woman choosing a LARC, this policy would cover the initial cost of insertion or injection, but also the cost of removal, reinsertion, or reinjection at some later date, as well as any costs associated with discontinuing LARC use in favor of a different method. It is likewise important that such a policy be able to respond when a woman’s circumstances change, thus allowing individuals to choose different options over time in response to changing needs.
Our proposed policy thus levels the playing field by letting women make informed choices about which method best suits their needs, with choice moreover unconstrained by cost. This stands in sharp contrast with what exists currently, which is that information barriers and the high up-front cost of LARCs may deter the use of such highly effective methods by both married and unmarried women, but perhaps most especially among those most likely to be poor.
Long-Acting Reversible Contraceptive Methods
LARCs refer to a class of birth control methods that are long acting and reversible. LARCs approved by the FDA for use in the United States are the copper IUD; hormonal IUDs, which release small amounts of a progestin hormone contained in many birth control pills; and subdermal contraceptive implants. Although highly effective at pregnancy prevention, LARCs do not offer protection against sexually transmitted infections (STIs) and so should be used with barrier methods such as a condom to reduce STI risks, a point we return to later. LARCs require an initial visit to a doctor or health-care provider to insert the implant or IUD. Removing the implant or IUD requires another visit, with fecundability—the term demographers use to refer to the ability to conceive—returning to its previous age-related state for the woman in question, save for instances in which some other intervening event occurs (for example, rare complications associated with LARC use or a STI affecting fecundability; see Hov, Skjeldestad, and Hilstad 2007).
Four hormonal IUDs (Kyleena, Liletta, Mirena, and Skyla), one copper IUD (ParaGard), and three subdermal contraceptive implants (Implanon, Implanon NXT, and Nexplanon) are FDA-approved for use in the United States. The copper IUD, ParaGard, is effective for up to twelve years; among hormonal IUDs, Mirena is effective for up to six years, Kyleena for up to five years, and Skyla and Liletta for up to three years (Espey and Ogburn 2011). Semiannual check-ups are recommended to ensure that the IUD has remained in place. The three subdermal implants (Implanon, Implanon NXT, and Nexplanon) are effective for three to four years.
LARCs require an initial visit to a doctor or health-care provider to insert the implant or IUD, but after this initial visit, LARCs provide a safe and highly effective contraceptive method that requires little effort. Their policy potential lies in the fact that they are safe and extremely effective at preventing a pregnancy.2 Table 1 reproduces estimates by James Trussell (2011) that show that the far greater effectiveness of LARCs in preventing pregnancies relative to other contraceptive methods is almost certainly due to their ease of use. For example, table 1 shows that for the pill, which is one of the most effective non-LARC methods, an unintended pregnancy during the first year of use is thirty times more likely under “typical” use relative to “perfect” use. This thirty-fold difference reflects inconsistencies such as forgetting to take the pill that occur for the average pill user. By contrast, unintended pregnancies are rare—between ten to 180 times less likely—for LARCs relative to the pill, this difference being due, in no small part, to the virtually identical effectiveness of LARCs under typical and perfect use.
Table 2, taken from Amy Branum and Jo Jones (2015), shows that LARC use in the United States is low but has increased in recent years. Megan Kavanaugh, Jenna Jerman, and Lawrence Finer find that among LARC users in 2012, 89 percent used an IUD and 11 percent used an implant, with notable increases in LARC use occurring among Hispanic women, those who had not yet given birth, and those with employer-provided health insurance (2015).
One disadvantage of LARCs is that their up-front costs can be as high as $700 to $1,000, depending on the health-care provider and LARC chosen (Trussell et al. 2015). Such up-front costs may pose barriers to LARC use for many women, particularly those with low incomes or who lack health insurance. Eliminating such cost barriers is thus a key component of our proposed policy of universal and no-cost contraceptive access. A second disadvantage, as noted, is that LARCs do not protect against STIs, thus requiring those using a LARC to also use a barrier method, such as the condom, to reduce the risk of an STI.
FERTILITY-RELATED BEHAVIORS AND PAST POLICY
The design of policy requires an understanding of the behaviors of interest, and nonmarital fertility involves behaviors that pose unique challenges to researchers and policymakers alike. To clarify issues, consider a premarital first birth, that is, a first birth to a never-married woman. Then, for social scientists, an immediate challenge is that any understanding of this phenomenon requires confronting the fact that premarital first births will involve, at a minimum, two behavioral processes—one involving marriage and the other involving fertility. That is, at any age t, we will observe some childless and never-married women transitioning to a first marriage and others remaining childless and never married; likewise at any age t, we will observe some childless and never-married women transitioning to a first birth and others remaining childless and never married (Wu 2015).3
For this reason, both research and policy have tended to proceed along two tracks, one focusing on the marriage side of nonmarital fertility and a second on the fertility side of nonmarital fertility. In the United States, marriage promotion and sexual abstinence among the unmarried have been the two policies to date whose goal was to reduce nonmarital fertility. In the case of marriage promotion, Congress in 2005 approved $100 million in annual funding, followed by another $75 million in 2010, for a set of policy interventions aimed at encouraging marriage among unmarried couples with children. One such program, “Building Strong Families” (BSF), featured the random assignment of economically disadvantaged and unmarried parents to an education program designed to improve relationship skills, this program having shown success at strengthening the relationships of married couples from more advantaged groups. However, a rigorous evaluation of BSF showed that for unmarried parents, this effort at promoting marriage failed to increase marriage, relationship stability, or the economic well-being of children (R. Wood et al. 2014).
PRWORA also provided substantial funding for programs that sought to encourage teens and young adults to abstain from sex until marriage. These programs were also unsuccessful in attaining their stated goals. An evaluation of sites that randomly assigned students to courses that followed abstinence-only guidelines in PRWORA found no difference four to six years after intervention between treatment and controls for a wide array of outcomes, including whether the student had initiated sexual activity, age at onset, recent sexual activity, STIs, pregnancy, and whether the student had given birth or fathered a child (Trenholm et al. 2007).
What might account for the lack of success of policy efforts to date? Consider abstinence, that is, policies intended to encourage young adults to delay sex until marriage or, less ambitiously, to delay the onset of sexual activity. A first difficulty with such policies is the near-universal levels of premarital sexual activity among young adults in the United States (Wu, Martin, and England 2017). Nevertheless, the core argument of abstinence proponents reflects a central demographic principle—that when onset is delayed, exposure to risk will decrease, thus resulting in fewer premarital first births, all else being equal. But post-onset factors such as poorer contraceptive use or knowledge will also lead to more premarital first births, leading skeptics of abstinence policies to argue that reductions in premarital first births would be best achieved by reducing post-onset risks. The empirical policy issue then concerns the relative influence of these factors, with the available evidence to date suggesting little empirical support for the potential role of abstinence in reducing nonmarital fertility (Trenholm et al. 2007; Wu and Martin 2015).
With respect to marriage promotion, one factor that may account for why this policy was unsuccessful is marriage itself—or more precisely, differences between married and unmarried couples with respect to the quality of their relationship. This hypothesis relies on two related pieces of empirical evidence, the first being that marriage promotion efforts intended to foster couple skills helped to strengthen the relationships of married couples, and the second being that a similar program was unsuccessful in strengthening bonds between unmarried couples. Couples who choose to marry are likely to do so because they perceive their relationship as being relatively strong. But if so, this also implies that the relationships of couples who we observe to be unmarried will be, on average, of lower quality than those of married couples. Thus, if the quality of relationships were, on average, higher among married couples than unmarried couples, this could explain why this policy was unsuccessful in strengthening bonds for unmarried couples but was helpful to married couples. But this also raises the possibility that efforts to promote marriage among unmarried couples will, on average, be targeting those in lower quality relationships, thus increasing the difficulty and complexity of policy efforts to promote marriage in such a population. This also raises the possibility that marriage promotion, even were it to be successful, could at the margin serve to encourage marriage among those who would otherwise not have chosen to marry, thus potentially increasing the number of lower quality marriages.
What about the fertility side of nonmarital fertility? The proximate determinants framework used by demographers (Davis and Blake 1956; Bongaarts 1978; Wu and Martin 2015) notes that nonmarital fertility will be influenced by behaviors such as sexual activity while unmarried, contraception, and the formation and dissolution of a relationship, cohabiting union, or marriage. From this perspective, two facts would appear particularly relevant. A first is that large numbers of nonmarital births in the United States are reported as unintended. Half of all U.S. pregnancies are unintended, and unintended pregnancies account for 80 percent of all pregnancies to teens and more than 70 percent of all pregnancies to unmarried women age thirty or younger (Finer and Zolna 2014; Zolna and Lindberg 2012). A second is that nonmarital first births continue to occur at quite early ages. Table 3 shows that in 2015, the modal age at a first birth was twenty for unmarried mothers but twenty-nine for married mothers.
For many social scientists, these patterns suggest that differences in contraceptive behaviors are a likely cause of why some women bear their first child within, and others outside, of marriage. This line of reasoning is not, however, accepted by all. Many economists, for example, see differences in contraceptive behaviors as causally determined by two factors: first, the opportunity cost of taking a pregnancy to term, with greater opportunity costs thus leading to the use of more effective contraceptive methods and in more effort expended in assuring effective contraception; and, second, by how much a future outcome is discounted, with a higher discount thus reducing contraceptive effort and increasing willingness to use a less effective method. Frank Furstenberg provided an early critique of these arguments by noting that they imply that outcomes would be identical under two scenarios, one in which women were required to expend effort to avoid a pregnancy, and another in which they were by nature contraceptively protected, with effort needed to become fecund (1992). LARCs thus provide a way women can effectively minimize their pregnancy risks with little effort, thus changing, as Isabel Sawhill notes, the “default” option by requiring women to expend effort to become pregnant (2014).
What do we know about the actual contraceptive behaviors of young adults in the United States? One clue is the substantial decline in teen births, perhaps because teens and young adults have become increasingly aware of the risk of STIs such as HIV. Yet the United States remains an outlier in having large numbers of unintended pregnancies and births relative to other advanced industrialized nations. Another seeming paradox is qualitative evidence that many unmarried couples say that they are not seeking a pregnancy yet also report that they contracept inconsistently (Edin et al. 2007; England et al. 2016). A study analyzing weekly data on sexual activity and contraceptive use finds that large numbers of female respondents report “pregnancy scares.” Many of these women subsequently report an unintended pregnancy (Gatny, Kusunoki, and Barber 2014). Yet another possibility is that individuals may use a condom during initial sexual encounters and in early stages of a relationship, but may then seek STI testing and transition to a different contraceptive method in later stages of the relationship (Sayegh et al. 2006). The picture that thus emerges from these and other studies is one of inconsistent contraception among many who are sexually active while unmarried.
A POLICY PROVIDING INFORMATION ABOUT, AND NO-COST ACCESS TO, A RANGE OF CONTRACEPTIVE METHODS
Two broad goals are at the heart of the policy we propose. The first is to provide women with the simplest possible message—that no-cost coverage is available to all. Providing free and universal access thus differs from what exists currently, which is that coverage is not universal and the cost of different methods varies in complicated ways depending on the woman’s circumstances and the provider or providers available to her. The second is to provide funding that will allow health-care providers to maintain adequate contraceptive supplies and to ensure that frontline staff have up-to-date knowledge and training. These goals can be achieved via coverage for women with health insurance from an employer-provided plan, coverage for women who do not have health insurance from an employer-provided plan, dissemination of user-friendly information about the advantages and disadvantages of all FDA-approved contraceptive methods, and funding to ensure both adequate contraceptive supplies and up-to-date knowledge and training of frontline providers.
Provisions in the Affordable Care Act (ACA) have moved some distance toward providing women with no-cost access to a broad range of contraceptive methods. Yet, ACA coverage is far from complete, provider compliance with the ACA’s contraceptive provisions may vary substantially, and whether the ACA will survive in its current form or if it will be modified, repealed, or replaced is currently unclear. Whatever the fate of the ACA or its contraceptive provisions, the intent of what is proposed here is simple—to provide no-cost and universal access that will address the contraceptive needs of both current and future generations of women.
Coverage for Women with Employer-Provided Health Insurance
For women with health insurance from an employer-provided plan, the proposed policy would follow current ACA guidelines that require insurers to provide, at no cost, counseling and access to FDA-approved contraceptive methods and services. These ACA provisions, which were phased in between August 2012 and January 2013, prohibit co-pays or coinsurance fees when using an in-network provider even for those who have not yet met their deductible. Contraceptive methods covered by the ACA include barrier methods such as diaphragms and sponges, hormonal methods such as the birth control pill, contraceptive sterilizations such as tubal ligations, and all FDA-approved LARCs. Were these ACA provisions to be no longer in effect, the policy proposed here would ensure continued no-cost access to these FDA-approved contraceptive methods, including LARCs.
Two exclusions in the ACA limit access to contraceptive benefits even when a woman is covered by an employer-provided health insurance plan (Bearak et al. 2016). Grandfathered plans are exempted from these requirements if the health-care plan was in place prior to March 2010 and if the plan had no subsequent and substantial changes to other benefits. The ACA also exempts certain religious organizations and employers from these requirements. The policy we propose would require that identical services and benefits be provided to women in such circumstances. Health-care providers would be reimbursed by the proposed policy at the same rate that providers charge to nonexempt employer-provided plans.
Coverage for Women Who Lack Employer-Provided Health Insurance
For women who do not have coverage from an employer-provided health insurance plan, a complicated set of policies currently provides contraceptive services and benefits at no cost to some, with others paying sliding fees and still others the full cost of such services and benefits. By contrast, the policy proposed here would provide, at no cost, the same contraceptive services and benefits as those available to women covered by an employer-provided health insurance plan. It thus would provide, at no cost, the same counseling and access to FDA-approved contraceptive methods as that provided to women from a health-care provider through employer-provided insurance. Funds from this policy would reimburse health-care providers for these services at the same rate as services for employer-provided plans.
Currently, a complicated set of policies provide contraceptive access and services to women who lack coverage from an employer-provided health insurance plan. For such women, benefits are available from two sources: from the ACA or from providers receiving Title X funding. For women receiving health insurance from the ACA—either from an ACA exchange or in states that adopted ACA’s Medicaid expansion—contraceptive services and benefits are required by the ACA to be the same as those provided by an employer-provided health insurance plan. For women who lack coverage from either the ACA or an employer-provided plan, contraceptive counseling and services are available from providers funded by Title X. Title X contraceptive services are available at no cost to women who fall below the federal poverty guideline. Women just above this threshold are charged a sliding fee and others the full cost for these benefits and services (Beeson et al. 2014; S. Wood et al. 2014).
From a policy perspective, contraceptive access for this group of women is highly unsatisfactory. Women who lack employer-provided health insurance will be drawn disproportionately from those with low incomes, a disadvantaged group that we know will also be at high risk of unintended and nonmarital births. The current policy landscape thus provides contraceptive services and benefits only to those disadvantaged women who can successfully navigate a highly complex system in which services are available at no cost to some, with availability to others limited to specific providers who can provide services to some at no cost, to others at a sliding fee, and to yet others only at full cost. The current system, in effect, poses the most barriers precisely to those most likely to have the greatest unmet needs.
Disseminating Information About No-Cost Universal Access
A policy of providing a wide range of contraceptive methods at no cost to women would not achieve its goals if women were unaware of the services and benefits provided by such a policy. For this reason, it is important that any such policy also include a dissemination component that would inform a wide audience of policy services and benefits.
The task of informing a wide audience is made easier by the simple and straightforward message that is at the heart of the proposed policy—that access is available to all women at no cost. Social media could also provide a low-cost way of informing large numbers of those in their teens and twenties about available services and benefits as well as providing user-friendly information about the pros and cons of FDA-approved contraceptive methods.
Ensuring Knowledge, Training, and Supplies for Frontline Providers
The policy we propose relies on doctors and other frontline health-care staff to provide both contraceptive counseling and the contraceptive methods themselves. But because discussions between doctors and patients are privileged by custom and law, we think it inadvisable for policy to attempt to dictate the content of contraceptive counseling provided to individuals. Thus, the policy proposed here does not seek to specify any specific protocol for the counseling and information provided to women by doctors or frontline staff.
Nevertheless, a critical component of our proposed policy is that adequate funds be made available to ensure that all providers have up-to-date knowledge and adequate training with respect to the full range of FDA-approved contraceptive methods. We anticipate that this objective will be aided in no small part by ongoing reviews that the medical profession conducts for itself, which is to provide up-to-date guidance and “best practices” that reflect the evolving state of medical evidence and knowledge. For example, the American Congress of Obstetricians and Gynecologists issued a 2012 recommendation that LARCs be made available to adolescents, citing “top-tier effectiveness, high rates of satisfaction and continuation, and no need for daily adherence” but also recommended that “As with all nonbarrier methods, to decrease the risk of sexually transmitted infections (STIs), including human immunodeficiency virus (HIV), health-care providers should advise sexually active adolescents to consistently use condoms along with LARC methods” (American Congress of Obstetricians and Gynecologists, Committee Opinion no. 539, 2012).
It will also be the case that some women will have urgent contraceptive needs, thus making it important for providers to have adequate supplies of the full range of methods—including LARCs—covered by this policy. We thus propose that adequate funding be available to frontline providers for maintaining adequate stocks of all FDA-approved contraceptive methods.
Could No-Cost Universal Access Reduce Poverty?
Could no-cost and universal access to effective contraception reduce poverty? Currently, we lack the sort of firm empirical evidence that would provide a conclusive yes or no answer to this question. Given the absence of such evidence, we instead turn to available theory. We begin by discussing how the choice of a contraceptive method and other fertility-related behaviors might be altered by a policy providing no-cost universal access based on expectations from standard economic theory on choice and consumption.
Preferences and Choice Behavior Under a No-Cost Policy
As may be obvious, we believe that the lives of many would be improved were they able to contracept more effectively. But as emphasized in the principles that we believe should guide policy, we believe even more strongly that whether, when, and with whom to have (or not have) a child are matters that policy should and must leave to individuals themselves. For these reasons, the policy we advocate—no-cost universal access—is deliberately designed to not incentivize any particular method over another. What the policy does seek to do is to level the playing field by setting the cost of all FDA-approved contraceptive methods to zero.
This also has implications for policy expectation under standard models of choice behavior. Standard economic theory posits that the choice of whether to contracept will be much the same as the choice to consume any market good available to consumers. Theory thus predicts that if the price of good A falls but the price of good B remains unchanged, this will in the aggregate lead some to consume A rather than B, with the increased demand for A not because of changes in preferences but rather because of changes in the relative price of goods A and B. Thus, we would expect a policy of no-cost universal access to lead more to contracept, not because it has altered preferences regarding whether to contracept, but because it has lowered contraceptive costs. We would likewise expect the policy to influence the aggregate mix of FDA-approved methods, again not because the policy has altered preferences, but because the policy has reduced the price of all such methods to zero.
The same logic generates expectations with respect to behaviors known to be correlated with STI risks. To fix ideas, consider a sexually active individual who is not in a monogamous relationship. Caution with respect to STIs will then vary with risk aversion, with those who are less risk averse more likely to engage in risky behaviors such as less consistent condom use, casual sex with many partners, or drug use. Again, standard theory generates expectations that such differences will exist but that changes in the relative price of contraceptive alternatives will not alter an individual’s level of risk aversion to STI risks.
It is important to emphasize that these policy expectations are theoretical in nature and thus do not speak to the magnitude of effects or whether there exist other causal factors that could reverse expected relationships. For these reasons and as discussed in greater detail below, we think it extremely important that sufficient funding be available to conduct carefully designed randomized pilots, which would provide firm empirical answers to these and other questions.
Labor Market and Relationship Churning
Policies to improve the earnings of low-skilled young adults in the United States have often pointed to broad structural shifts in the U.S. economy as creating a situation in which those lacking a college degree now face a labor market in which earnings have stagnated or declined as jobs have been subject to global competition or automation. These issues in turn have often motivated policy proposals such as an expansion of the Earned Income Tax Credit to low-income males, increases in the minimum wage, a universal child allowance, or apprenticeship programs that would, for example, connect young adults who are still in school to potential labor market opportunities. More broadly, this perspective sees human capital as the factor most predictive of income and hence of the poverty status of individuals and households. If so, fertility-related behaviors will be a cause of poverty only to the degree that they causally influence the formation of human capital and other related skills and attributes that employers value.
An alternative possibility stems from the fact that there is often substantial “churning” during the schooling to work transition, with churning referring to the rapid movement of recent labor market entrants through a series of jobs (Topel and Ward 1992; Neumark 2002). A standard economic model explains this churning by positing a search and matching model for job seekers. Under this model, churning occurs because on the supply side, labor market entrants possess attributes that may not be well matched initially to those attributes sought, on the demand side, by employers. Churning will decline with time and labor market experience as workers, either through learning or by chance, find jobs that are better matches to their attributes. Empirical evidence to date has shown positive returns to churning, consistent with the hypothesis that, on average, better matches will occur as labor market entrants move from initial to subsequent matches.
Could the search for a good relationship be at least as complicated as finding a good job? As in the job matching model, this model supposes that each individual brings a different mix of attributes to a potential relationship. Churning will continue until a match occurs that is acceptable to both and that exceeds each person’s idiosyncratic threshold. Note in particular that the model predicts that individuals will churn to an eventual match that will be higher in quality, on average, than initial matches. Findings from one study are consistent with this hypothesis (Bzostek, McLanahan, and Carlson 2012).4
Could an unintended birth affect a young woman’s ability to churn through jobs and relationships? To our knowledge, these questions have been underemphasized in both the research and policy literatures. Yet it is plausible that an unintended birth could decrease a young woman’s ability to move from her current job to a subsequent job that could provide both a better match and a higher wage. What we do know is that combining motherhood and full-time employment poses difficulties even for many married women, particularly when children are infants and toddlers. Thus it is plausible that reductions in unintended and nonmarital births could increase the ability of young women who might otherwise have had these births to work full-time and year-round, thus allowing them to gain substantially in labor market experience.5
The policy counterfactual of interest, then, is to compare two contraceptive regimes, a control regime consisting of the current contraceptive behaviors of sexually active young men and women, and a treatment regime, in which young women have better knowledge about, and free access to, LARCs.6 Under the current control regime, we observe a large number of unintended births occurring to unmarried couples. We know that despite their high hopes for themselves and the child, their relationships are often fragile. Under the proposed treatment policy regime, a women choosing a LARC will avert an unintended birth, thus allowing her (and him) to churn to subsequent relationships. This may, in turn, allow both men and women to find better matches while avoiding an unintended birth in an earlier, lower quality, match. Higher quality matches under the treatment regime could plausibly result in a variety of benefits for him, her, and their child. What we do know is that under the current control regime, the relationships of couples who have an unintended and nonmarital birth are not only fragile, but also subject to frequent discord following a break-up, with fathers viewed negatively by mothers and with the formal or informal child support of nonresident fathers often posing a serious financial burden to him.
This does not exhaust the ways that a policy of no-cost, universal contraception could have plausible positive effects. Consider the following example that, although hypothetical and referring to fictional individuals, nevertheless suggest ways in which universal and no-cost contraceptive access could raise incomes and increase well-being in disadvantaged groups.
Consider M, a young woman who grew up in a poor single-mother family, but who is nevertheless a hard worker with a sunny disposition. After graduating from a not very good high school, she found a job at a fast-food restaurant. She and a guy, J, from her neighborhood, have been together for some time and she starts living with him. J, who is older, has two children born to two different women from previous relationships. He works hard to provide for them, but money is tight.
One day, one of M’s cousins, who she grew up with, has a bad pregnancy scare, and a few months later, M too finds herself pregnant after missing her period. Then six months after giving birth, M breaks up with J. She still sees J sometimes and he helps when he can, but his finances are now stretched even tighter. At twenty, M now sees that having a minimum-wage job while caring for a newborn is much harder than she ever realized and that this is not what she wants for herself or her newborn. So she decides to try for something better, enrolling in a few classes at the local community college. But the baby girl, like all infants, often gets sick, and M’s frequent absences from the classes she is taking means that she’s not doing well. J tries to help but when several absences from work because the little girl gets sick lead his boss to fire him, he scales back the time he spends with his daughter and M, in no small part because of the fights that ensue because of his precarious finances. All of this is extremely stressful for M, who reluctantly decides to drop out of classes at the community college, at least for now. But fragile childcare arrangements and times when the baby is sick make things rough. And the job still pays only a minimum wage.
Now consider M in the alternative policy regime in which she has no-cost access to highly effective contraception. In this world, she still ends up working at a local fast-food restaurant after high school and, as before, she still moves in with J. Her cousin has a bad pregnancy scare, but in this alternative policy world, the two of them learn from a Facebook advertisement just how easy it is to get highly effective contraception at no cost. They schedule an appointment with the cousin’s OB/GYN and, going there together, both opt for an implant. M now avoids getting pregnant and having the baby at twenty. As before, she grows dissatisfied with a minimum wage job, but she now avoids missing classes and so is getting good grades at the local community college. After two years of classes, she is a state-certified health-care aide and gets a job at a local hospital. Her sunny personality and hard work endear her to her supervisors at the hospital. In addition, J is able to hold onto his job, which allows him to get a promotion and help provide for his two children. At twenty-three, M and a different boyfriend decide to have a baby, and she gives birth to a baby boy. As before, she has to call in sick when the infant catches something, but her job now provides her with sick leave and her supervisors, who also have young children, appreciate her hard work and are therefore understanding.
Our analytical point here is not to assert that M and J are typical, but rather that even when individual attributes and preferences are constant and unchanging, outcomes could differ in the two alternative policy regimes because of dynamic selection due to changing circumstances in ways that could, in turn, generate plausible anti-poverty consequences. Thus M, the hypothetical young woman, is hard working and seeks to improve her human capital in both policy worlds, but an early, unintended and nonmarital birth poses barriers in one world that are not present in the other. As Diana Strumbos, Donna Linderman, and Carson Hicks note, parental responsibilities are a key barrier to successful completion of community college (2018). Similarly, employers are better able to assess her value as an employee—her hard work ethic and sunny personality—in one policy world but less able to do so in the other. For J, avoiding an unintended pregnancy could mean the difference between holding a job and being fired. For both M and J, stress is far greater in one policy world than the other, and this too may have consequences for the ability to maintain steady employment and hence experience on the job and in the labor force.
It is again important to emphasize that these arguments are theoretical and that, to our knowledge, there is a general lack of firm empirical findings on these dynamic selection mechanisms.
As Isabel Sawhill (2014) notes, LARCs change the “default option” from requiring action to avoid a pregnancy to requiring action to become pregnant. Other, more commonly used birth control options, such as the pill or condoms, exhibit vastly different failure rates between perfect and typical use (Trussell 2011), indicating a disparity between preferences and experienced contraceptive efficacy that would not exist with LARCs. Thus among those choosing a LARC, yet another policy expectation is that there would almost certainly be fewer unintended pregnancies and births, fewer abortions, and thus also decreases in the complex family forms that arise from multipartner fertility in which couples bring children from previous relationships into their current relationship. And, because the mechanism by which a LARC prevents a pregnancy is biological as opposed to behavioral, it also follows that, stated counterfactually, the effect of the treatment on the treated (for example, reductions in unintended births for those choosing a LARC) would likely be virtually identical to the effect of the treatment on controls (that is, reductions in unintended births were those not on a LARC to have been on a LARC). If true, this would eliminate one important source of policy uncertainty—whether the effect of a policy will be the same for the treated and controls—when attempting to predict how outcomes would be changed under a new policy. What this does not address, however, is take-up—how many might in fact adopt a LARC method were no-cost contraceptive access to be universal.
LARC Take-Up
Would a policy of universal and no-cost contraceptive access increase the use of LARCs? A first answer is that we currently lack the sort of evidence that would definitively answer this question. A second answer is to note, following Charles Manski (1995), that the answer to LARC use will necessarily lie between two bounds, one in which LARC use is unchanged by the policy, and the other in which the policy causes all women to adopt a LARC. Both of these answers are, strictly speaking, correct, but as a practical matter, neither provides much in the way of helpful guidance. But we also know that the decisions that individuals make will be influenced by costs and hence that under current policies, the up-front cost of LARC methods will, all else equal, lead many to adopt non-LARC methods. This implies that a policy providing universal and no-cost access to a wide range of contraceptive methods should, all else equal, increase LARC use, but it also follows that eliminating cost differentials will heighten the role of preferences. Some women may choose not to use any method by abstaining from sex until marriage or by relying on natural rhythm methods. But for those choosing to contracept, providing no-cost access to a wide range of available methods would, in principle, better allow all such women to choose the method that she most prefers. But preferences will be influenced not only by whether failure rates of a particular method are high or low, but also by factors such as her immediate situation coupled with her plans for the future, STI prevention, perceived side effects, what methods peers have chosen, and so forth.
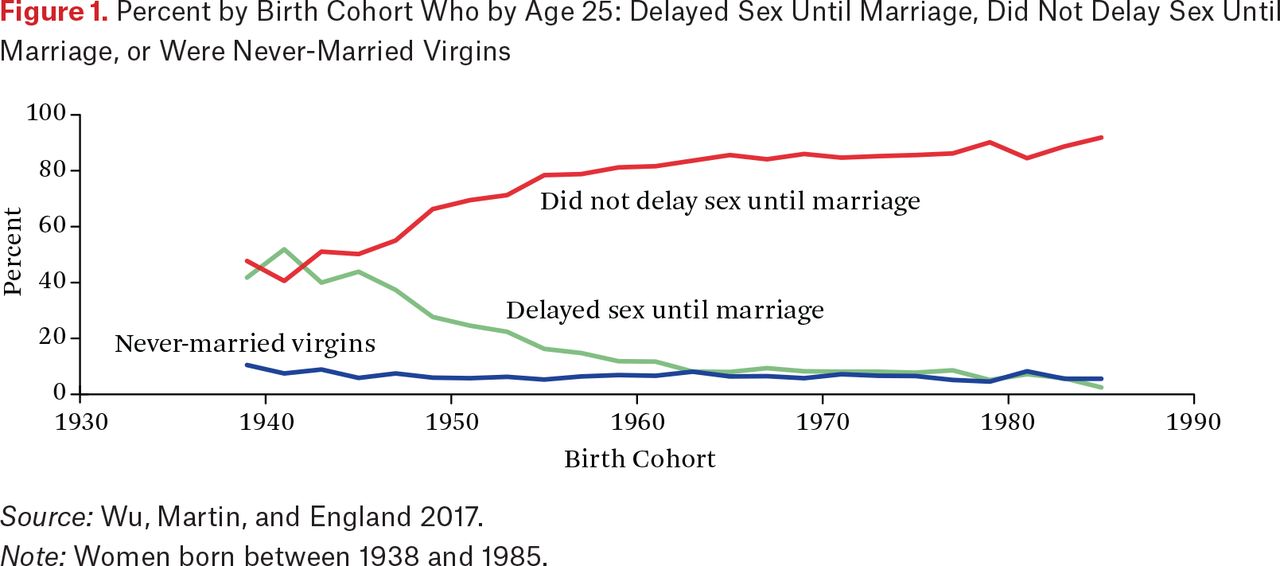
Contraceptive choice is relevant to those who are sexually active and because of this, it is useful to know how many in the United States are sexually active while never-married. Figure 1 presents cohort trends in the percent of women who, by age twenty-five, reported that they delayed sex until marriage, did not delay sex until marriage, or were never-married virgins (Wu, Martin, and England 2017). We see substantial increases in the percent of never-married women reporting that they were sexually active and corresponding decreases in the percent reporting that they delayed sex until marriage. Changes in behavior were especially rapid for women born earlier in the twentieth century, but figure 1 suggests far less change for women born later in the century. What is clear is that the vast majority of U.S. women report being sexually active while never-married, but also that roughly 15 percent of those born after 1965 continue either to delay sex until marriage or to abstain from sex while never married.

Estimates in figure 1 provide potentially important clues that may inform ongoing debates between those advocating abstaining from until sex until marriage versus those far more skeptical of such policies. A potential criticism of no-cost and universal contraception access is that such a policy may well lead to increases in premarital sex among those who would have otherwise chosen to abstain from sex until marriage. Figure 1 shows that any negative consequences would necessarily be limited to the small numbers of those who do in fact choose to abstain from sex until marriage, with this group having declined for successive birth cohorts of U.S. women. Thus in aggregate, negative consequences hypothesized by skeptics will pertain to the smaller numbers who abstain from sex while never married, while positive consequences emphasized by proponents will pertain to the larger numbers not abstaining from sex while never married.
A recent, important study presents findings on IUD use by education and reproductive life cycle for females aged fifteen to forty-four who reported using some form of contraception and who were either married, cohabiting, or in a sexual relationship (Sweeney, Eeckhaut, and Gipson 2016). Using data from the 2006 to 2010 and 2011 to 2013 National Survey of Family Growth, they find that overall IUD use varies little by education. However, they do find substantial education gradients for women at different points in their reproductive life cycle. Among women who have not yet given birth but plan future childbearing, IUD use increases with education, but this educational gradient reverses for women who have had at least one birth. Among those with less than a high school education who plan future childbearing, IUD use is 0.4 percent for those who have not yet had a birth and 23.0 percent for those who have had one or more births. This nearly 60-fold increase would appear difficult to explain from changes in opportunity costs, but could plausibly reflect the need and desire for more effective contraception among those with fewer years of education. This study, while providing estimates of IUD use under current policies, does not speak to the question of what LARC use would be were there to be universal and no-cost contraceptive access.
Some evidence concerning this question can be gleaned from two sites, St. Louis and Colorado, in which women were provided LARCs at no cost. Beginning in 2007, Jeffrey Peipert and his colleagues conducted a prospective study that followed a sample of 9,253 women in the St. Louis area (2012). Study participants, recruited from an at-risk population, were informed that they could choose a LARC or other contraceptive method at no cost for a two- to three-year period and that they could switch or discontinue any method at any time. Prior to the study, fewer than 5 percent of participants were using a LARC, but when informed about no-cost access to a wide range of contraceptive methods, 74.8 percent chose a LARC. Those choosing a LARC expressed higher satisfaction, had high continuation rates, and had markedly lower contraceptive failure rates compared to those choosing other methods; by contrast, few differences emerged in STIs and other measures of sexual risk-taking behaviors among those who did and did not choose a LARC method (McNicholas et al. 2014). However, design elements in this study may well limit the generalizability of findings. Participants were recruited from specific sites that provided contraceptive counseling and services to at-risk and disadvantaged women. Thus, study participants may not be representative of any larger population of interest. It is also possible that, given study objectives, frontline providers may have been more likely to guide participants to the choice of a LARC as opposed to other methods. Finally, there was no attempt to randomly assign participants into control and treatment groups. For these reasons, this study, although important and highly relevant, is not ideally suited to providing firm causal answers to questions such as what LARC take-up would be were cost barriers to be eliminated by a policy providing free and universal access.
The state of Colorado began a program in 2009 that provided LARCs at no cost to clients at twenty-eight Colorado health-care facilities that received Title X funding (Ricketts, Klingler, and Schwalberg 2014). This program, funded by a private foundation, provided no-cost access to LARCs for clients at these twenty-eight Title X facilities, with other methods available to those above the poverty line at the usual Title X sliding fee. The program also provided funding for Title X staff training on counseling and insertion techniques and for clinics to purchase and maintain current stocks of LARC methods; sixteen of the twenty-eight clinics were thus able to provide LARCs for the first time to clients. Administrative data compiled by Sue Ricketts and her colleagues show that LARC use among fifteen- to twenty-four-year-old Title X Colorado clients was 4.5 percent in 2008, the year prior to this program, but rose to 19.4 percent in 2011, with this trend also accompanied by decreases in births, abortions, and the number of infants served by Women, Infants, and Children (WIC). The Colorado program thus provides population-relevant findings that complement those in the St. Louis study, but these authors do not attempt to disentangle the extent to which increased LARC use was a causal factor in observed trends.
An important recent study provides plausibly causal evidence that increased LARC access led to fewer teen births (Lindo and Packham 2017). Using a quasi-experimental difference-in-difference design, the authors found that in those Colorado counties with clinics receiving funding that increased LARC access there was a 6.4 percent reduction in teen births over five years relative to counties in Colorado and other states in which funding was not provided. The relatively large magnitude of this effect is, to our knowledge, the first plausibly causal evidence relevant to the potential policy effects of increased LARC access. Note, however, that the findings from this study are limited to teen births only, thus underscoring the need for carefully designed longitudinal randomized pilots that could provide much-needed causal evidence on a wide range of outcomes of policy interest.
Table 4 presents estimates that provide a snapshot of LARC use in 2013 by state for women age fifteen to nineteen who sought contraceptive services from Title X providers (Romero et al. 2015). Variation in LARC use by state is substantial, ranging from 0.7 percent in Mississippi and 1.5 percent in Indiana to 19.6 percent in Alaska and 25.8 percent in Colorado. It would seem unlikely the 25.1 percentage point difference observed between Colorado and Mississippi reflects differences in preferences; instead, observed differences across states may well reflect other factors, such as knowledge of contraceptive services and benefits available from Title X providers, the number of and access to providers, and the specific services and benefits available from providers receiving Title X funding. Such factors will again complicate any attempt to assess potential LARC demand.
These studies provide no clear-cut answer to the question of how many more women might adopt a LARC under a policy that provides universal and no-cost access to a wide range of contraceptive methods. They also provide a dauntingly wide range of estimates that, if taken at face value, range from increases in LARC use of around 70 percentage points for participants in the St. Louis study, 23.4 percentage points based on the group comparisons reported by Sweeney and colleagues (2016), 14.9 percentage points from trends in Colorado as documented by Ricketts and colleagues (2014), and a 25.1 percentage point range based on cross-sectional differences across states as estimated by Lisa Romero and her colleagues (2015). Poverty reductions—the goal of this double-issue RSF—will also depend heavily on LARC take-up among particular groups, for example, low-income segments of the U.S. population. And as shown in table 2, LARC use in the United States has increased dramatically over the last decade, albeit from very low initial levels, thus suggesting that attempting to estimate LARC demand may be akin to shooting at a moving target. Nevertheless, the weight of available evidence does, we believe, point to a considerable degree of unmet contraceptive need that may be particularly acute among those facing the most disadvantaged circumstances. If forced to forecast unmet demand for highly effective contraceptive methods in this group of women, we would hazard a guess that under a policy of universal and no-cost access, LARC use might increase from anywhere between 5 to 25 percentage points, with the former and latter being highly pessimistic and highly optimistic guesses, respectively.
The Need for Longitudinal Randomized Intent-to-Treat Pilots
Carefully designed experiments assigning individuals at random to treatment and control groups have provided some of the best evidence to date on whether policies work. It is thus important that the policy proposed here include funding to states choosing to participate to conduct carefully designed randomized trials. Such pilots could follow some of the design elements used in previous trials by targeting economically disadvantaged young women and randomly assigning participants to control and treatment groups.
Answering these questions would ideally require a panel study that followed not only women over time, but also the children born to these women and men fathering these children. One possible design would be to target never-married young women who have not yet had a birth. Such a pilot could then be designed to follow study participants over time, thus allowing comparisons between controls and treatments on outcomes such as satisfaction with the control and treatment contraceptive protocols, unintended pregnancies and births, labor force attachment and earnings, the formation and dissolution of intimate relationships, and, when children are born, measures assessing child development and well-being.
COSTS AND BENEFITS
When not covered by health insurance, the up-front cost of a LARC to a woman can be as much as $1,000. Because LARCs remain effective over periods ranging from three to twelve years, LARCs are cost effective over the long run and provide a method whose failure rate is several orders of magnitude lower than methods such as the birth control pill or the condom (for detail on the cost of LARCs, see Trussell et al. 2015, table 2). And as noted previously, the up-front cost of implants and IUDs may have led many providers to not maintain sufficient stocks of LARCs, thus preventing some from providing the full range of available contraceptive options to women. A final note regarding projections of costs is that contraceptive sterilization through procedures such as a tubal ligation are a surprisingly common contraceptive method for women who have completed their childbearing and who thus do not desire another pregnancy. Typical costs of a tubal ligations can range anywhere from $1,500 to $6,000, whereas LARCs can for many women provide a similar degree of protection from a pregnancy at a lower cost while also providing reversibility should wishes, desires, or circumstances change. (Current contraceptive provisions in the ACA cover both LARCs and tubal ligations, but not vasectomies for men.) It is thus possible that a policy providing universal and free access to a wide range of contraceptive methods could result in some women opting to choose a LARC rather than a tubal ligation. These issues also imply that a full assessment of the estimated direct cost of providing no-cost contraception to all women would require, ideally, estimates of these direct costs over a woman’s full reproductive life cycle.
A potentially highly attractive element of a policy providing no-cost and universal access is that the direct costs of the contraceptives themselves are very low, both in absolute terms and when compared with both current and possible future policies that seek to reduce poverty. The cost an individual woman faces in choosing the most expensive contraceptive method—the birth control pill—can be as much as $50 per month or $600 per year. This then provides a hard upper bound on the per capita direct costs of providing no-cost contraception, given that in practice, program costs for methods such as the birth control pill will be far lower than the market price charged to women lacking coverage. Moreover, the per capita direct costs under the policy we propose would occur only for women who currently do not have health insurance from an employer-provided plan. Under the proposed policy, per capita direct costs would thus be incurred only when a woman lacks coverage from an employer-provided plan or for the small numbers of women with employer-provided insurance but whose coverage involves a grandfathered insurance plan or for those whose employer has been exempted from providing contraceptive coverage. In cross-section, program dollars would thus be directed to those subgroups lacking health insurance, thus in effect targeting program resources to those with low incomes and other disadvantaged segments of the U.S. population who may also have serious and unmet contraceptive needs. But in life cycle terms, proposed program dollars are directed to those times when a woman does not have employer-provided health insurance, for example, those periods when she may be employed part time or when she is ineligible for coverage from a parent, spouse, or partner. Put another way, these provisions mean that this proposed policy is, in effect, simultaneously universal and targeted. It is universal by mandating that contraceptive access be available at no cost to any woman who requests these benefits. Yet it is, in effect, targeted by directing program dollars to those without employer-provided health insurance who will be, on average, more disadvantaged than those with it.
Costs per woman could be affected and would depend on the cost of staffing programs providing comprehensive contraceptive information, the numbers of women choosing a LARC or other contraceptive method, and the cost of providing the contraceptive method(s) chosen over a woman’s reproductive life cycle. These costs are nevertheless likely to be substantially less than many policies, current or proposed, that have sought to reduce poverty.
What might be the potential economic benefits from such a program? Any such exercise requires a series of counterfactual assumptions, but Emily Monea and Adam Thomas provide what is perhaps the most comprehensive exercise of this sort to date (2011). Using their estimates, Robert Plotnick puts projected savings at $80,000 per teen birth (2016). Sawhill, also citing Monea and Thomas, estimates that current contraceptive services receiving public funding avert more than 2 million unintended pregnancies per year at a savings of $7.6 billion and that “If we did more to eliminate all unwanted and mistimed pregnancies, we could save an additional $6 billion” (2014, 124). Simulations conducted by Sawhill and colleagues suggest that were a woman able to delay a mistimed birth, outcomes for the child whose birth was delayed would be improved, with increases in high school graduation of 7 percentage points, decreases in teen childbearing of 3 percentage points, increases in college graduation of 8 percentage points, and increases in life-time income of around $52,000 (Sawhill, Karpilow, and Venator 2014).
DISCUSSION
In this article, we have proposed a policy that levels the contraceptive playing field by providing universal and no-cost access to the full range of FDA-approved contraceptive methods, including long-acting reversible contraceptives, which are both safe and highly effective. By guaranteeing the same access to low-income women as that enjoyed by many high-income women, this policy would lead to fewer unintended and nonmarital births, particularly among the most disadvantaged segments of the U.S. population, which would in turn, we argued, increase well-being and reduce poverty.
For policymakers, the proposed policy has a number of distinct advantages. Its modest costs allows it to be combined with other anti-poverty programs. It provides women and couples with the simplest possible policy message—that of universal and no-cost access. It addresses information and cost barriers that are likely to deter the use of highly effective methods of contraception. It is unusual by being both targeted and universal—providing universal access yet simultaneously targeting funding to those likeliest to have the greatest unmet needs. It adheres to a set of principles that acknowledges and respects individual preferences, choices, and behaviors while providing resources that let individuals better align behavior with preferences on whether, when, and with whom to have a child.
FOOTNOTES
↵1. We return later in the article to the issue of how this policy may or may not alter preferences, but in this respect, we follow Isabel Sawhill, who similarly stresses the importance of eliminating cost and information barriers so as to better allow individuals to “align” their preferences with intended outcomes (2014). But Sawhill also argues in favor of stigmatizing unintended births and thus the decision to take an unintended pregnancy to term. We argue instead for the narrower, simpler, and less value-laden policy goal of eliminating barriers that may prevent a woman from achieving that which she prefers on matters such as whether, when, and with whom to have a child.
↵2. Because the subdermal implants release progestin, their safety record parallels that of the birth control pill. The Dalkon shield, an early IUD, had a number of safety issues, most notably by increasing the risk of pelvic inflammatory disease. However, modern IUDs, including those approved by the FDA for use in the United States, have been shown to be extremely safe (see, for example, Farley et al. 1992; Hubacher et al. 2002; on findings from large-scale multisite randomized trials, see also WHO 1982, 1990).
↵3. Yet a third behavioral process that complicates matters is cohabitation. Much of the increase in nonmarital fertility in recent decades has been due to the increase in births to cohabiting couples. The emerging consensus is that the main policy concern for births that occur in cohabiting unions is the stability of such unions. We return to this issue when discussing empirical findings on marriage promotion.
↵4. Note also that this matching model differs from a model proposed by Gary Becker, with the key difference being that Becker posits the existence of some factor that rank orders all individuals in the marriage market (Becker 1981). Matches then occur with the top-ranked male marrying the top-ranked female, and so on. By contrast, the matching model proposed here assumes, as in the job matching model, that matches will be idiosyncratic, thus positing that different criteria will be weighed differently by each participant. This also differs from William Julius Wilson’s (1987) influential “marriageable male” hypothesis, which holds that male earnings (or job stability) is the factor weighed most heavily by all females when considering potential mates.
↵5. Maria Cancian and Daniel Meyer find that although median wages and hours worked increased among former AFDC recipients following welfare reform, only one in four was employed full time. Difficulties with childcare arrangements or illnesses of children were among the most cited reasons for voluntary or involuntary job separations (2000).
↵6. Note, for example, that studies providing plausibly causal estimates of the effect of a teen birth on subsequent outcomes do not in fact speak to the policy counterfactuals considered here (see, for example, Hotz, McElroy, and Sanders 2005; Rosenzweig and Wolpin 1995). For example, Joseph Hotz and his colleagues employ a natural experiment design that uses miscarriages to estimate effects of a teen birth on a series of later life outcomes. The logic is to use miscarriages as an instrument that, in effect, randomizes the key variable of interest—whether a birth to a woman occurs during her teen years. Such a design thus resembles an experiment that manipulates a single factor while leaving unchanged all other factors—in this case, including the contraceptive behaviors of at-risk populations, the key factor of policy interest here. Thus, for example, with respect to fertility, Hotz and his colleagues find that women with a teen miscarriage “do not delay childbearing much past their early twenties” and that “only 56 percent . . . have not had a child by age 18” and that “by age 24, only between 17 and 19 percent . . . have not had a child” (702). As Hotz and his colleagues note, their miscarriage design is not well suited for evaluating the effects on wages because “wage rates are measured only at ages when women work and our estimation strategy does not account for this source of selectivity” (708).
Open Access Policy: RSF: The Russell Sage Foundation Journal of the Social Sciences is an open access journal. This article is published under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.
REFERENCES
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.