
Abstract
This study examines how Americans’ narratives of pain are connected to social inequalities using more than 1,500 in-depth interviews collected as part of the American Voices Project. Our novel mixed-method approach to these “big (qualitative) data” uses machine learning and qualitative analysis to demonstrate that discussions of physical pain are prevalent across groups, but narrative content varies by demographics including educational background and gender identity. Our findings demonstrate (1) that pain is commonly described as a challenge that shapes everyday life, (2) that pain narratives often invoke morality and distinction, and (3) that narratives diverge around discussions of unequal medical treatment, illness identities, vulnerability and suffering. We discuss the implications of our findings for scholarship on inequality and experience, social scientific methods, and health policy.
- inequality
- pain
- suffering
- culture
- health
- computational ethnography
- mixed-methods
- machine learning
- social determinants of health
- in-depth interviews
This article examines what Americans have to say about pain and what their answers reveal about social inequality and suffering. Qualitative and computational analyses of more than 1,500 interviews from the American Voices Project (AVP) support the finding that physical pain, in both acute and chronic forms, is a prevalent and significant health challenge for Americans (Domenichiello and Ramsden 2019; Burke 2019; Fayaz et al. 2016). Although discussions of pain are widespread in these data, narrative content varies by demographic characteristics, including educational attainment and gender identity. Our findings show that Americans from varied backgrounds indicate that pain creates substantial challenges and that pain and its management are framed in moral terms as either stigmatizing or distinguishing; however, accounts diverge around discussions of unequal medical treatment, illness identities, vulnerability, and suffering. We argue that examining pain narratives using these unique data provides insights into how inequalities shape experiences with suffering (Bourdieu 1999), health (Freese and Lutfey 2011), social scientific methods for analyzing large qualitative and mixed-methods datasets (Abramson et al. 2018), and equitable health policies in the wake of the opioid epidemic (Smirnova 2023).
Social Inequality and Disparate Pain
A substantial body of research shows that health and illness rates reflect broader inequities (Freese and Lutfey 2011). Unequal exposure to environmental risks, disparate opportunities for maintaining wellness, unequal treatment by medical institutions, and numerous other mechanisms translate patterns of social disadvantage into negative morbidity and mortality outcomes (Link and Phelan 1995; Geronimus 2023; Smedley, Stith, and Nelson 2003; Woolf and Aron 2013). In the United States, inequalities along socioeconomic, racial, and gender lines influence health from birth (Jones et al. 2019; Smedley, Stith, and Nelson 2003). Social inequalities shape how long we live, our likelihood of remaining in good health, and the supports that are available when we become ill (Abramson 2015; Carr 2019; Woolf and Aron 2013; Newman 2004). An expanding body of empirical evidence supports a core related claim of sociological theory—inequalities get “under our skin,” shaping our health and bodies in ways that connect social structures and biology (Durkheim 1984; Mason 2013; Powell-Wiley et al. 2020; Turner 2008; Walters et al. 2011).
Pain is a central aspect of health and illness. In contemporary integrative accounts, pain is defined as “an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage” (Raja et al. 2020, p. 1976).1 Pain reflects not just biology, but our experiences with the social world, simultaneously shaping behavior in complex ways (Biedma-Velázquez et al. 2022; Zajacova, Grol-Prokopczyk, and Zimmer 2021b). Research indicates that chronic pain (lasting more than three months) can be a powerful barometer of both quality of life and population health, and that reported pain levels in the United States have increased in the twenty-first century (Zajacova, Grol-Prokopczyk, and Zimmer 2021b; Mills, Nicolson, and Smith 2019).2 Pain is a chief complaint driving health-care use; it is associated with lost productivity and contributes to the prescription and use of addictive and increasingly criminalized narcotics (Ballantyne 2015; Voon, Karamouzian, and Kerr 2017; Vowles et al. 2015).3 The divergence in pain levels across groups has been linked to historical disparities in accidents, violence, hazards, and unequal treatment in medical institutions, which shape stress, illness, and well-being (Mullins, Yong, and Bhattacharyya 2022; Janevic et al. 2017). Furthermore, disparities in pain control have been documented along racial, ethnic, and socioeconomic lines (Anderson, Green, and Payne 2009). Addiction to narcotic painkillers can have devastating effects, especially for those who occupy a precarious position in America (Smirnova 2023).4
Dedicated empirical examinations of the meanings of pain have used qualitative methods to contribute alongside work using statistical approaches to chart patterns and trends. Such examinations have focused on the disruptions surrounding chronic pain and their influence on everyday experiences (Charmaz 2002; Toye et al. 2021). This work illustrates how pain can pervade peoples’ lives, limit activity in the present, and create uncertainty about the future (Bunzli et al. 2013; MacNeela et al. 2015). Chronic pain can cause people to feel betrayed by their bodies and limit their interactions with others (Snelgrove, Edwards, and Liossi 2013; Froud et al. 2014; Kirkham, Smith, and Havsteen-Franklin 2015; Nortvedt et al. 2016). Concerns about stigma related to both pain and medical treatment are also common, as is discussion of the challenge and importance of making physical pain legible as legitimate to health care providers (Souza et al. 2011; Hopayian and Notley 2014; Toye et al. 2013; Peilot et al. 2014). These accounts further illuminate how coping requires considerable time and effort for those suffering from chronic pain (Finlay, Peacock, and Elander 2018; Wilson et al. 2017; Ojala et al. 2015).
Pain, Experience and the Social Organization of Suffering
Pain has wide-reaching effects on societies, institutions, and individuals. However, it is a challenging empirical object because its intertwined physical, psychological, and social aspects limit reductionism (Turk and Okifuji 2002). Physical pain is shaped by biology, emotions, beliefs, culture, and socialization (Bendelow and Williams 1995; Peacock and Patel 2008). It is also experienced as a deeply personal phenomenon: subjective distress in bodily sensation. Yet more vulnerable members of society are at an objectively greater likelihood of experiencing trauma, illnesses, and accidents that place them at disproportionate risk for pain and consequently suffering more broadly (Bourdieu 1999; Farmer 1996; Kleinman 1997).5 The distribution of pain in society also reflects structural violence that shapes workplaces, neighborhoods, and homes, creating patterns of social suffering (Bourdieu 1999; Farmer 1996).6 Finally, the historical contexts in which we live influence which remedies are available, and whose pain is recognized or silenced (Bendelow 2006; Farmer 2006; Peacock and Patel 2008). This complexity makes pain sociologically revealing because it offers important insights into the social organization of suffering (Farmer 1996; Biedma-Velázquez et al. 2022; Zajacova, Grol-Prokopczyk, and Zimmer 2021b).
As a complex, multifaceted phenomenon, pain offers social scientists an important object of study for advancing connections between social structure, the human body, and experience. Sociologists and social psychologists have long argued that personal experiences such as pain exhibit commonalities in ways that are not reducible to biological universals or radical individuality (for example, Durkheim [1893] 1984; Elias 1939; Goffman 1978). In this framework, our experiences are mediated by our position in social hierarchies, and the educational, health, social, and labor institutions that shape our actions and beliefs over the life course (Bourdieu 1984; Elias 1939; Sewell 1992; Wacquant 2004).
Sociologist Pierre Bourdieu (1984, 1999) extended this line of inquiry by articulating a model of how the objective and subjective manifestations of inequality are intertwined. In his conceptualization, subjectivities (internal experiences) are objectively distributed in ways that reflect and reinforce social divisions from birth (Wacquant and Bourdieu 1992). Institutions validate the experiences and practices of socially advantaged groups, positioning theirs as proper and meritorious, naturalizing inequality in the process (Bourdieu 1984). Class-based ways of thinking, acting, speaking, and perceiving the world provide a form of capital (Bourdieu 2018) that reflects and extends other advantages (Bourdieu 1984) in schools, markets, and hospitals, providing advantages in securing everything from college admission to narcotics (Abramson 2015; Lareau 2003; Shim 2010; Wacquant 2004). Others have added that race, gender, age, and their intersections can function similarly, organizing opportunities, experiences, and access to resources (money, social networks, credentials) in ways that reinforce hierarchies (Tilly 1999) and discount the experiences of socially marginalized groups (Collins 1992).
Examining connections between pain and American society (Bendelow and Williams 1995) in dialogue with such a perspective offers potential insights into inequality (Bourdieu 1984), social suffering (Kleinman, Das, and Lock 1997), and the organization of experience more broadly (Goffman 1972; Collins 1992, 2000). Our examination of the unique AVP data provides a contribution by illustrating multilevel connections between social inequality, Americans’ experiences of pain and the organization of suffering.
METHODOLOGY
This article empirically examines experiences of pain in the contemporary United States, and how these experiences are connected to inequality and stratification.
Research Questions and Expectations
We ask three interrelated research questions:
Q1: How do Americans talk about pain?
Q2: Do pain narratives vary in ways that are connected to patterns of inequality?
Q3: If so, how?
We had three expectations based on prior empirical research and theory.7
E1: Pain will create challenges and disruptions for people across demographic groups.
E2: Narratives of pain will invoke cultural understandings, moral assessments, and structural limitations on coping behaviors.
E3: How people narrate pain will reflect their experiences and understandings, organized by inequalities over the life course.
Data Set
To examine inequalities in the origins and experiences of pain in the contemporary United States, this article draws on data from more than 1,500 in-depth interview transcripts collected as part of the American Voices Project between 2019 and 2021. The AVP aims to connect representative sampling, standardized survey measures (that identify subpopulations), and the depth of qualitative interviews at a scale that is well suited for our purposes.8 Despite the potential upside of a large sample of in-depth interviews, the AVP presents challenges—for example, whether big qualitative data can support epistemically diverse qualitative approaches (Abramson and Gong 2020), whether scope compromises depth (Lareau and Rao 2016), and practically, how to identify, index and analyze narratives without reducing tens of thousands of pages of text to numbers or small subsets of interviews. Our approach to addressing the empirical questions speaks to these methodological challenges.
Analytical Strategy
Our analytical strategy combines traditional qualitative analyses with computational social science (CSS) techniques (that is, computational ethnography). Such a combination offers a useful approach for big qualitative datasets such as AVP (Abramson et al. 2018; Li and Abramson 2024). Computational analyses can help identify and visualize broad patterns in human subject data such as interviewee speech and field observations (Abramson and Dohan 2015). In particular, machine learning provides a toolkit for identifying text around a concept such as pain and can be deployed in a way consistent with iterative qualitative analyses (Li, Dohan, and Abramson 2021). Visualizations help identify broad patterns and situate specific narratives (Abramson et al. 2018).9
A mixed-methods analysis answers our questions more thoroughly than a single-method approach by triangulating findings, providing complementary evidence, and connecting levels of analysis (Abramson et al. 2018; Du Bois 1899; Small 2011). We proceeded in six chronological phases:
pilot reading of a sample of full interviews;
using machine learning to identify segments of interview transcripts on pain;
creating semantic networks to visualize language patterns;
in-depth readings of all text discussing pain, and a subsample of full interviews;
identifying overlapping themes in the networks and narratives; and
repeating to identify similarity and difference within and between categories of respondents.
For step 6, we used individual attributes recorded in the survey questions connected to the AVP interviews to divide respondents into subgroups. We focused on criteria central to prior literature on how inequality shapes experiences of pain (gender identity and educational attainment). These categories were selected because they are analytically important and provided adequate volumes of text for both qualitative and computational analyses.10 This does not suggest that these are taken to be the only, or even the most important, categories; our methods do not allow us to make such a determination but rather to show similarity and difference in categories established to be important in extant works.
ANALYZING INTERVIEWS IN AVP’S BIG QUALITATIVE DATA
One of the first challenges in analyzing a large-scale, multipurpose qualitative dataset is identifying textual data relevant to new research questions (Li, Dohan, and Abramson 2021). Computational social scientists often begin by searching the text with a predefined dictionary (a list of keywords, including synonyms for the construct of interest). However, even when the literature guides the selection of keywords, researchers’ existing dictionaries may miss novel or nuanced ways in which people talk about a concept of interest (such as pain). Although this may be framed as an advantage for some approaches, qualitative research often seeks to make sense of this type of variation (Abramson and Gong 2020). To address this challenge, we cast a wide net and used human review to minimize the exclusion of relevant text on initial passes and the inclusion of irrelevant text subsequently (Li, Dohan, and Abramson 2021; Sánchez-Jankowski 2002).
We used Word2Vec in Python (a programming language used in CSS) to inductively identify words that respondents use to talk about pain. Word2Vec is a class of unsupervised machine learning models that can be trained on large corpora of text to obtain high-dimensional vector representations of words in a vector space where words that are used in the same contexts or analogically are clustered together (Mikolov, Chen, et al. 2013). Sociologists have taken advantage of Word2Vec to map semantic similarities and analogies among words in a variety of sociolinguistic contexts (Arseniev-Koehler et al. 2022; Arseniev-Koehler and Foster 2020; Garg et al. 2018; Kozlowski, Taddy, and Evans 2019; Stoltz and Taylor 2021). By quantifying this relational structure of meaning, Word2Vec’s word embedding models are able to inductively discover not just text that contains the word pain, but also other words people use when they talk about pain, and which traditional dictionary-based methods struggle to detect.
We trained Word2Vec models on all respondents’ speech, excluding interviewers and other nonspeech information, and inductively identified the twenty seed words that were most synonymous, analogical, or closely related to the word pain in this particular dataset.11 We then used these seed words to extract the paragraphs in which respondents talked about pain and pain-related experiences. We obtained 5,852 paragraphs that potentially contained pain narratives and used this reduced dataset as the basis for our computational analysis.
Thematic Networks
Another challenge in analyzing a large amount of text is that respondents talk about concepts of interest at multiple levels and in a variety of contexts. This maps on to a challenge in sociological theory, where scholars of culture argue that it is necessary to look both at articulated narratives and underlying language patterns connected to how we filter. Theories of culture have noted that people often filter experience through cognitive schema or habitus (D’Andrade 1992; Leschziner and Brett 2021), but articulate understandings as narratives and justifications (Vaisey 2009). In connecting these, Margaret Frye notes, “People make sense of the world by consciously deploying collective narratives… . Collective narratives put flesh around the bones of cultural schemas [more basic symbolic structures], specifying symbolic events or character traits that elucidate schematic associations between attributes and outcomes” (2017, 948).
Our empirical approach aims to use computational analyses of natural language, and qualitative analyses of narratives, to connect these levels of culture. In our analysis, networks represent core language patterns and building blocks that help support and situate themes in respondents’ narratives. These networks provide a useful starting point for subsequent qualitative analysis aimed at identifying and interpreting cultural schemas.
We used semantic network analysis to detect and model thematic structures. Topic models are also popular tools for exploring themes in large-scale qualitative datasets. However, topic models provided limited insights for our specific project in pilot analyses, perhaps because of their reliance on high-frequency words and vulnerability to stop words. Instead of relying on the frequency of single words, semantic network analysis allowed us to examine the co-occurrence of word pairs: how often and how rarely two words are used in the same context to describe pain-related experiences. From the semantic network view of a narrative, words appear as nodes. Words frequently used together will be connected by an edge weighted by the frequency of co-occurrence; words that are not used together will appear unconnected. The contrast between the presence and absence of edges helps us identify clusters—sets of words that are densely connected to each other, but relatively disconnected from other words—pointing to distinct thematic structures underlying narratives. By explicitly modeling not only the high-frequency but also the low-frequency word pairs, semantic networks are well suited to robust analyses alongside the linguistic noise of interview transcripts. Sociologists have used word co-occurrence networks to explore the thematic structure of other forms of text in wide-ranging inquiries (Carley 1994; Rule, Cointet, and Bearman 2015; Hoffman et al. 2018; Basov 2020; Basov, de Nooy, and Nenko 2021; Padgett et al. 2020).
Once we obtained a baseline network, we visualized its core structure to identify and interpret the distinct thematic contexts in which pain was discussed. Because the resulting thematic network was large and dense, we pruned the network to preserve the robust thematic structure while enabling readability. Our goal was to show enough context words in a thematic cluster for it to be meaningful while revealing boundaries between distinct thematic clusters and highlighting relationships between them. Although this optimization process was qualitative and iterative, we tested a wide range of pruning hyperparameters to determine the extent to which different specifications of the network affected the results.
A third challenge in analyzing large-scale qualitative data is that the distribution of narratives often does not correspond to the distribution of demographic groups. For example, consistent with existing literature (Bendelow 1993), we found that those identifying as women talked more about pain and pain-related experiences than men. We also observed unbalanced distributions of narratives across racial-ethnic groups, educational levels, income levels, and geographic locations. Although quantitative variables in an unbalanced sample can be easily reweighted to approach distributions in the population, narratives cannot. Focusing only on the core structure of a given size controls for unbalanced distributions to a certain extent; we also use semantic network analysis to contextualize qualitative analysis.
Stop Words and Sensitivity Tests
Stopwords present a challenge to the intelligibility of semantic networks. These are words such as the, a, by, for, and and, which are so common in English that they carry little semantic information relative to the noise they add to the model. Although Word2Vec models typically do not require the removal of stopwords, given the large amount of filler words in oral language, we focus our attention on only nouns, verbs, and adjectives, and manually remove some specifically functional words used by transcribers such as inaudible and personalname. Personalname, which refers to the redacted name of a person, is relevant. However, in practice these names co-occurred with role words daughter, husband, doctor, or referenced the interviewer. Therefore, for our networks, we removed personalname from node visualization, but retained the role words. We also excluded the word ass as a stopword because there are mentions of the colloquial phrase “pain in the ass,” which is analytically distinct from talking about pain as physical or mental suffering. We consider this a reasonable trade-off, given our aims, it reflects the interview context and is not fully natural language based on unprompted conversations. Furthermore, a subset of interviews were conducted in languages other than English and then translated. Even though the translations likely capture information on the core concepts needed for our analyses, some valences may have been lost.
In sensitivity tests, we found including all words in the Word2Vec model did not significantly change which words are identified by the model as synonyms or closely related to pain. We also included highly frequent bigrams—phrases that consist of two consecutive words, such as mental health, medical bill, and heart attack—but none of these bigrams is frequent enough to appear in the network. We used pain and twenty other words that Word2Vec identifies as most similar to pain as seed words to generate a corpus of text in which Americans are talking about pain. We then extracted co-occurring word pairs from a twenty-word context of each occurrence of any of the seed words in all interviewee speeches. Using a six-word or full-sentence context did not fundamentally alter the structure of networks. To optimize interpretability without losing information on core semantic structures, we pruned the network by keeping the top 0.1 percent of the most frequent word pairs and the top fifty most central words by node betweenness. These thresholds reflect the interpretive aspects of CSS analyses completed alongside our in-depth reading of the text. In other words, they are not purely mechanical by design, mirroring an iterative and interpretive logic. Further, rigidly mechanistic approaches pose a different risk in itself for interpreting computational models (Chang et al. 2009) and producing ecologically valid accounts more broadly (Cicourel 1982). Notably, verbal patterns are consistent with our model, visual configurations, and our interpretative analysis of the text (subsequently reproduced in reanalysis by another team).
To construct subnetworks, we subset the text based on respondent demographic characteristics including education level and gender identity. As noted, these groups were selected because of both analytical importance and practical limitations around weighting text and subsetting data unbalanced in size between groups.
Narrative Analysis
Our qualitative analysis is grounded in a contemporary iterative approach that examines themes both deductively, based on prior work and expectations, and inductively, based on emerging patterns (Abramson and Sánchez-Jankowski 2020; Deterding and Waters 2021; Lichtenstein and Rucks-Ahidiana 2023). After aggregating relevant paragraphs in Python, we also used the query function in NVIVO, a contemporary computer-assisted qualitative data analysis program, to cross-tabulate narratives.12 Central to our analysis, our in-depth reading focused on identifying similarities and differences in individual and group narratives as comparative qualitative logic rather than a basis for statistical generalizations (Abramson and Gong 2020). Connecting narrative sets and weights for population estimates was not feasible for this study.
To identify qualitative themes, we used paragraphs as the unit of analysis, exporting paragraphs in which the word pain appeared from NVIVO into text documents to limit performance bottlenecks experienced on the AVP server. Paragraph-level analysis is common in qualitative analyses, particularly computer-assisted qualitative data analysis, and can provide important context while limiting false positives, as in using full interviews, or false negatives, as in words or sentences alone, in identifying thematic patterns (Li, Dohan, and Abramson 2021). This produced approximately 1,429 pages of text across groups. The exported text was organized by respondent so we could read all paragraphs in which the word pain was used for each respondent. This allowed us to see when and how pain was discussed throughout each interview.
Given the quantity of text associated with the number of interviews we analyzed, as well as the range of topics and issues covered by the interviews, we could not holistically read all transcripts in which respondents spoke about pain. However, at the outset of the project we performed a holistic reading of more than twenty random complete transcripts to familiarize ourselves with the flow of the interview questions and themes. In performing our qualitative analysis, where necessary for interpretation we moved back and forth between reading the extracted paragraphs of text and complete transcripts. For instance, when the text was unclear or particularly relevant, we would go back to read more of the interview in NVIVO. For each group, we read all text until new themes related to our research questions no longer appeared, and then kept with our focus on pain due to time limitations and data set size. After reading through, writing memos, and identifying representative or otherwise key quotes for all groups, we triangulated the findings by comparing the patterns of similarity and difference identified through our in-depth narrative reading with those evident in the networks.
Both our network visualizations and narrative analysis played key roles in answering our research questions. The networks help reveal broad patterns and the narratives provide core illustrations of how people discuss their experiences of pain. The themes identified in our narrative reading shape our interpretation of the networks that might otherwise be more vulnerable to misinterpretation (Cicourel 1982); the networks help situate quotations in a broader text sample (Abramson et al. 2018; Abramson and Sánchez-Jankowski 2020). Together, the approaches connect pain narratives at the level of both basic language patterns and elaborated accounts, which reveals multifaceted connections between inequality and pain. Core computational and qualitative findings were independently substantiated as part of the qualitative verification project AVP workshop, coordinated by Robey, Karcher, and Elman at Syracuse University.
RESULTS
Table 1 presents the number of interviews that include pain narratives in the AVP data by simplified gender and education categories.
File and Group Reference Frequencies for Qualitative Analysis
The table reveals that discussions of pain are widespread across groups.13 Our analyses of content demonstrate that pain is connected to concrete everyday challenges in respondent narratives (E1); that narratives often involve discussions of morality, meaning, and distinction (E2); and that differences by demographic group reflect divergent experiences around disparate medical treatment, identity threats, and how complex traumas create pain (E3).
We begin by examining general patterns before moving on to analyses by education and gender. We focus on education as an aspect that links social advantages, health behavior, and narrative justifications, such as cultural (health) capital (Bourdieu 1984; Lareau 2003; Shim 2010). We then turn to gender as an organizing category that often shapes experiences with pain and how pain is treated or perceived (Barker 2005; Bendelow 1993; Kempner 2014).
Mapping Discussions of Pain in the AVP
Figure 1 presents a semantic network that visualizes the structure of language use across 5852 interview segments discussing pain-related experiences. Each node represents a word situated in the context of other words that appear in pain narratives. The size of the node is proportional to the betweenness centrality of the word in the text segment—the degree to which the coherence of the narrative depends on this particular word. A tie that connects two nodes represents a correlation between a pair of words. Density of ties is proportional to the strength of the correlation between words and themes. Themes are distinguished by their distance from each other. Words were identified computationally, as described above, but color coding reflects a holistic interpretation based on network patterns and in-depth readings of text, which gives us greater confidence that they are not artifacts of computational methods. For instance, the green cluster containing words such as surgery, knee, bone, neck, and walk references discussions about managing a damaged body, which is both a source of pain and practical challenges observed in both networks and narratives. The clusters are identifiable by grayscale shading, but the full color version is available online (https://www.rsfjournal.org/content/10/5/34).

Baseline Semantic Network of Pain Discussions in AVP Data
Source: Authors’ tabulation.
The key themes in figure 1 include medical management (red), coping strategies (orange), broken bodies (green), everyday experiences or feelings (blue), and relational support (purple). This reflects that when asked about their health problems, AVP respondents discussed how pain is felt and experienced in relation to their everyday lives (feelings); how relationships with other people such as family and friends can offer physical, logistical, and emotional support, but might also become a source of tension (relationships); how pain is connected to physical trauma (broken body); everyday coping strategies; and pain’s connection to physicians and medical treatments (medical management). These patterns show the core language people use to connect pain to experiences, and in which contexts.
Unpacking Pain Narratives: Pain and Everyday Life
Our narrative analysis reaffirms extant survey data showing pain is prevalent and significant for many Americans (Yong, Mullins, and Bhattacharyya 2022). Even narrow searches for mentions of the word pain reveal frequent and wide-reaching discussions of pain in the AVP data. A comment by Juan Carlos illustrates how these discussions often reflect the extent to which pain is part of everyday experience. In discussing what an average day looks like for him, Juan Carlos, who is identified as an Hispanic man working in a low-income job, said, “For me, a typical day is waking up, trying to shake off the lower back pain, it’s constant… . I’m feeling it right now.” In addition to its omnipresence, pain was reported to constrain the kinds of activities people can engage in on a given day. Over time, this limits the lives people are able to lead and shapes how they present themselves in social settings (see also Abramson 2015; Charmaz 2002).
AVP respondents reported that pain, especially chronic pain, influenced their thinking about themselves and their social identity. In a clear example of this broader pattern, Dan, a young college-educated white man, said, “The biggest issue was how I had been feeling within the past year was the fact that I was not able to continue the same lifestyle that I like or want because of my injury and the amount of pain that I was in. That had a big frustration on who I am as a person, who I’ve seemed to become.” Like many, Dan reaffirms how pain becomes an organizing aspect of life and identity.
Many AVP respondents described seeking medical care, where they approached health-care providers who facilitated surgeries, prescribed painkillers, or ruled out these treatments. Others sought alternative treatments such as marijuana, alcohol, exercise, and mindfulness or meditation to dull pain either in lieu of or alongside medical management. The coping strategies people deployed shaped their schedules (medical engagement is time-consuming), molded their sense of self (pain can limit activities), and influenced their relationships. This is seen most clearly in management strategies that involve the persistent use of narcotic pain medication or other often-stigmatized strategies, which were invoked alongside discussions of challenging life trajectories.
Challenging Life Trajectories, Narcotics, and Stigma
How respondents framed the use of narcotic pain medications was revealing. One comment by Jim, a middle-aged white man who had attended some college but did not have a college degree, illustrates how respondents connected life challenges, pain coping strategies, and negative outcomes as part of a challenging life trajectory narrative. For Jim, the use of narcotic fentanyl to manage chronic pain developed into addiction and added to other challenges in his marriage and life. When asked how he had come to live at his current address, Jim connected his trajectory to pain and addiction, which contributed to separation from his wife:
[my ex-wife] who I was going to grow old and fat with. I got old and fat, but not with her. We just, it just went off the rails. I have chronic pain, had it since the 90s. So, I spent over a decade on fentanyl. Toward the end I was getting tired of it simply because with the narcotic aspect, you can see, you know, where addiction could start to play a factor… we got to the point where we were, she said, I love you, but I can’t live with you anymore.
The issue for Jim was not that pain or addiction was the sole cause of his troubles. Instead, his story illustrates a trajectory in which chronic pain intersects with broader challenges, adaptations (taking narcotics), complications (addiction), and ultimately further disruption.
Given the stigma associated with the use of opioids, discussions of strategies involving the use of pain medications often invoked distinctions between so-called abusers and those who were able to avoid medication or use it in a way that limits harmful physical effects (such as bodily damage) or social effects (such as stigma, threats to identity). People who admitted to using narcotic pain medications often emphasized their efforts to minimize negative effects while further emphasizing that their use is legitimate and limited. As Shonda, an older black woman, told the interviewer, “if I’m having back pain that day or something, and it’s too excruciating, I go get me some pain pills and I’ll take them for that particular day. But for every day taking pain pills, uh-uh. I’m not fixing to do it. I’m not fixing to kill my kidneys and my other organs taking stuff. I’m not a pill taker. I don’t like taking pills. Never have, and I never will. If I don’t have to take it, I’m not taking it.”
Leanne, a middle-aged white woman, likened persistent use of opioids to heroin. When asked by her AVP interviewer whether she ever coped by relying on prescriptions, pain medications, marijuana, or other substances, Leanne replied, “Never taken any of it in my life, pain medication when I had C sections, obviously, but see all these people getting addicted to heroin and, yeah, no thank you.”
Even those who used other sometimes stigmatized strategies, such as marijuana, were careful to separate themselves from the specter of opioid abuse. For example, a college-educated black man named Marcellus noted, “One of the problems that I’ve had, I’ve smoked marijuana. One thing I don’t do is take pain pills because I’ve saw what it does to a lot of people that I’ve known.” In this statement, Marcellus draws a boundary between his choice of coping mechanism, which he sees as a potential problem, and the even more dangerous strategy of using prescription pain medication. A key finding was that respondents from all backgrounds described pain management in terms of physical concerns but also as a moral event, with implications for identity and distinction (Abramson 2015; Werner, Isaksen, and Malterud 2004).
Mapping Discussions of Pain in the AVP: Educational Differences
We now turn to how differences in social advantages manifest in our sample. Our qualitative and semantic network analyses revealed that although pain affected daily life for Americans of all backgrounds, pain and resources for responding to it reflect broader inequities. We begin by analyzing subnarrative networks to explore the correlations between social position, educational attainment, and narrative structure. Figures 2 and 3 present a comparison of pain narratives between respondents with a four-year college degree, and those who do not have a college degree.14 Once again, color and shading indicate the leading theme in each of the clusters, and node sizes indicate the centrality or relative importance of a specific word in the overall narrative.

Semantic Network of Pain Discussions in AVP Data by Education, Four-Year College Degree or Higher
Source: Authors’ tabulation.

Semantic Network of Pain Discussions in AVP Data by Education, No Four-Year College Degree
Source: Authors’ tabulation.
Overall, the subnetwork of respondents with four-year or advanced college degrees showed a more centralized structure around the medical management of pain. This suggests, as we would expect, skill in elaborating medicalized narratives. Discussions on medicalization are prominent even when discussing coping with pain outside of the hospital and clinical settings. For example, medication, surgery, insurance, and doctor are among the most central words used by highly educated respondents. Opioids are less central in these narratives and are routinized as part of everyday coping (as an orange node).
In contrast, among those without four-year degrees medical terms are dispersed across themes such as coping strategies (orange), experience or feeling (blue), and broken bodies (green). This mirrors discussions of pragmatic and often more dispersed strategies central in the narratives of respondents. For instance, opioids and doctors are grouped alongside nonmedical coping strategies (orange), and surgery is connected to physical breakdown (green) in a way that differs from those with higher levels of education. Second, the connection between illness and relationships (purple) is pronounced in the networks and connected to language about disease, mirroring our qualitative analysis showing that how pain affected roles was a concern and challenge for respondents.
Our qualitative analysis confirms and further articulates this division between medicalization and coping as a central organizing theme in Americans’ experiences of pain, as well as the differential effect on social roles, which resurfaces in our discussion of gender.
Unpacking Pain Narratives: Origins, Capital and Contestation
In-depth qualitative analysis by education revealed variations in the origins and experiences of pain, as well as the cultural narratives used to describe it. Respondents with less education often referred to medical providers, conditions, and treatments in general terms. For example, respondents used descriptions such as “my bones hurt” rather than medical terms (for example, “arthritis”). In a representative example, Elisa, a low-income woman who had not completed high school, spoke about experiences with sciatic nerve pain by saying, “They said it’s the largest nerve people have on the left side of the body, and sometimes it becomes swollen, and when it’s swollen, that’s when you have very strong pain. But they said there isn’t any medication for that.” In contrast, Americans with at least a bachelor’s degree often used precise medical terminology. They described medical providers in specific terms, referring to their gastroenterologist or orthopedist, and explained their own experiences using terms such as angioplasty, ablation, and endoscopy. This reflects a domain-specific form of cultural capital that people may draw on to understand, explain, and justify their experiences in ways that reinforce social advantages or disadvantages. It is also a form of language validated through interactions with providers and institutions from whom they seek care or resources for coping (Shim 2010; Abramson 2015).
Respondent narratives also revealed differences in the espoused causes and nature of pain itself. Dental pain was a major theme for all except for those with a bachelor’s degree or higher. This likely reflects disparities in oral health and the fact that dental insurance is often a “luxury” item in American health care. On the other hand, discussions of injuries from travel and vacations mostly appeared in the narratives of people with college degrees. Trauma and violence, aspects of precarity to which those in lower socioeconomic groups are disproportionately exposed, were particularly pronounced in the narratives of those with less than a high school education. Those without a high school degree shared stories about contending with the unequally distributed risk of experiencing pain because of assault, abuse, losing a family member to murder, or spending time in prison.
Divergent positions and life experiences mapped onto the ways respondents drew distinctions between legitimate and illegitimate narcotic use. For example, Isaac, a middle-aged white man with a college degree, explained it this way:
When you say, “use pain medication,” the only pain medication she [subject’s spouse] ever uses is anything that’s prescribed by a physician… . What my wife probably should be getting to help her cope with her chronic [disease], she’s not getting. And the big reason for that is because of what society has done with the term pain medication. To me, it’s all been caused by people cheating the system. People getting prescriptions, selling on the pavements and getting it in the open market. And, of course, consequently, we have an epidemic, and that’s how it started, anyway. Now, it’s we have an epidemic and everybody is so closely scrutinized, including physicians.
In this statement, Isaac connects perceived social problems (limited opportunities for pain management and perceived cheating of the system), his view of the moral failings of individuals (who take advantage), and a perceived innocent’s suffering (Isaac’s wife) to construct a narrative of blame and victimization. Isaac draws on classic tropes of deservingness and legitimation that are widespread in American ideology and policy and employed by institutional actors as well as members of the public (Patterson 2000; Anderson 1999; Foster et al. 2023; Mohr and Duquenne 1997; Sánchez-Jankowski 2008; Wacquant 2022).
By contrast, those with less than a college education spoke openly with interviewers about struggles, addiction, violence, and complexities within their families and communities. Like peers with higher levels of education, their narratives often involved “boundary work” (Lamont 2000) to draw distinctions around which avenues of pain relief were legitimate. However, their accounts focused on direct examples of complexities rather than hypotheticals. For example, an older white man named Tom answered a question about whether he had ever used marijuana or prescription pills to cope with pain, saying, “Don’t like drugs, hate them. I’ve seen what it had done to our mother. The only drugs I take is this, my prescription. And I need to take, I don’t take anything that I’m not supposed to take. And even with the pain meds I have, it says, every four hours or when needed. I make sure I stretch it out to that four hours, and sometimes longer because I don’t want to get dependent on that.” He explains why his behavior is in accordance with the ideals of methodical sobriety. This finding follows research showing how people use their responses to health challenges to draw distinctions and present their own strategies as honorable in light of what they see as the most (or only) respectable solution to a challenge (Abramson 2015).
Pain Is Part of the Job
The narratives we analyzed also revealed connections between pain and workforce parti-cipation in ways that varied by education and reflect other aspects of social class such as occupation and income. For respondents with college degrees, computer-related injuries or work stress were often identified as the causes of pain. As a young college-educated black man named Phil noted, “one thing I will say is that I’ve experienced more lower back pain, which is due to constantly sitting down and working on the computer. To counteract that, I try to do those walks as much as possible to loosen up my back, but that’s really it, you know, nothing crazy.” For those with less education, occupational injuries tended to be associated with manual labor jobs and were often compounded over time. For instance, in explaining how she came to be on disability, Gloria, a woman who had worked in a manual occupation and did not have a high school degree, said this:
Now, when I worked in [organization], I left there in the mid-90s. I left because I got a back injury and the judge gave me disability in my back… . I went to [place], worked there… . This ladder fell … and hit me on my shoulder. Well, I’m not knowing that it had damaged some bone and, hell, I just kept working. And every now and then I would get this pain, but I wouldn’t pay it no mind. But when I went to [organization], the kind of work we was doing, dusting … and pulling trash, I started having this terrible pain. And I end up getting surgery on my shoulder.
After recounting the story, Gloria explained to the interviewer that it took six years for disability payments to begin. During that time, she had to continue working to stay afloat. Being able to stop laboring to address this issue was an untenable luxury.
The coping strategies of those with less education were often shaped by occupational precarity and the need to endure pain for survival. Juan Carlos, a low-income respondent who does not have a high school degree, was representative in saying,
When it first started happening to me, I ignored it [the pain] for over a year to tell you the truth. I ignored it for a year because I had to work. I had to make my money. I had bills I had to pay. I didn’t have time to be sick and so, I noticed like my [redacted] leg started hurting and it kept hurting until one day [it] was like four days later after the pain started, I reached out for something and I just felt a rip in my leg, but I guess the muscle or tendon or something ripped and it was painful then I chilled, relaxed.
For Juan Carlos and others in his position, pain is common but often not practically actionable until the body itself is broken by labor. In labor generally, and manual occupations in particular, pain was framed as part of the job. This was reflected in how respondents from lower socioeconomic strata matter-of-factly framed pain as just a part of life, work, and identity.
Respondents with higher education levels expressed less matter-of-factness and more contestation. Their narratives also emphasized efficacy in encounters with medical providers. In recounting an interaction with a doctor, Fred shared,
I said, “No, you’re not putting a needle in my back, we’re not doing none of that.” I’ve seen people get that done and they crippled now, so no, I’m not interested.” He said, “All right, then we can put you on pain pills,” so I said, “Okay. All right, give me the pain pills, but give me some education along with it because I don’t want to get hooked on these things,” because I know a lot of people that went from them pills to dope.
Fred’s comment invokes a perennial distinction between those who are credible and those who are part of a dubious moral category subject to addiction. Fred also likely leveraged his cultural health capital in navigating a health-care system beset by inequalities.
Gender and Pain
Like education, gender was a significant source of variation in how respondents experienced and made sense of pain. The accounts of female interviewees posited that women’s experiences of pain are often not taken seriously, and that the health conditions that disproportionately affect them are trivialized (see also Barker 2005; Kempner 2014). At the same time, both men and women suggested that women have more capacity to endure pain (Bendelow 1993). Similarly, both believed that men were generally more actively discouraged from expressing pain (see also Bendelow 1993; Jaworska and Ryan 2018). Further, AVP narratives highlighted that men often experience chronic pain as a threat to their status and identity (see also Courtenay 2000; Charmaz 1994). Respondents often drew connections between pain and sacrifice, albeit in ways that reflected gendered norms.
Mapping Gender and Pain Narratives
Figures 4 and 5 present semantic networks by respondent gender. The thematic structure of gender subnetworks is interesting in two ways. First, men’s accounts of pain are heavily bifurcated between talking about pain as part of everyday life and social relationships (in purple), and talking about pain as a medical diagnosis (in red). By contrast, women’s accounts of pain use a broader, decentralized network. Second, men often pinpoint specific locations in their body as the source of pain (neck, arm, knee, leg, foot, and bone), whereas women describe pain as being more generalized.

Semantic Network of Pain Discussions in AVP Data by Gender Identity, Male
Source: Authors’ tabulation.

Semantic Network of Pain Discussions in AVP Data by Gender Identity, Female
Source: Authors’ tabulation.
These gendered differences are connected to narratives of disparities, which mirror scholarly accounts of the historical barriers women face in getting medical professionals to believe their suffering is real and legitimate. Our qualitative analysis supports the hypothesis that women might have turned to individual coping strategies as a result of their struggles to establish credibility in interactions with health-care providers, as well as with family and colleagues, which they connected to the belief that their pain and suffering were not taken seriously.
Unpacking Pain Narratives: Unequal Treatment, Sacrifice, and Identity
Women’s accounts highlighted their perceptions of being dismissed and mis- or inadequately treated for pain and health issues. Eleanor, a retired white woman, provided a poignant illustration related to a health problem affecting women:
I’ve had female problems and it’s like I would call, they [providers] would say, okay, go get this over the counter, try this and I try that and it wouldn’t go away. So then call back and say, “Oh no, don’t use that one. Use this one, go get this one.” So, I’d run back out to the store and get the other medication and try that a couple of days later it’s not getting better… . It was like, this is ridiculous. I’m in pain here. I need to do something I need to be looked at. It needs to be examined.
Eleanor’s account emphasizes that she felt that medical providers did not take her pain seriously (Barker 2005; Kempner 2014). This reflects the challenge women have in establishing credibility with medical providers and being seen as trustworthy narrators of their experience (Schäfer et al. 2016; Wright 2018). These feelings of being dismissed and improperly cared for were pervasive in women’s narratives and crossed racial as well as educational categories.
Pain, Caregiving and Sacrifice
Our narrative analysis also revealed the ways in which pain and pain management are framed as axes of distinction but in ways that reflect gendered expectations and ideologies (Kempner 2006). For example, caregiving responsibilities, prioritization of family, and associated self-sacrifice frequently came up in women’s discussions of pain management. For example, Imani, a young black woman with a high school degree, explained that she sacrificed effectively managing her own pain to support her partner:
So it’s like, well, you can get it you can get twenty pills right now, even though he needs like 120. So I’ll skip my medications because his [chronic disease] and he’s had it for quite some time. And you can see the deterioration that has happened [across] the months and years. So the way I looked at it, he needs his medication more than I do, so I’ll only get the one I need for swelling or inflammation, so it’ll kind of help with the pain, it’ll make it bearable, but I’ll be able to actually at least function, I want to make sure he has his pain pills, and he has what he needs for his blood, everything.
The narratives highlighted a variety of ways in which women made sacrifices to care for loved ones in their social networks, as clearly articulated here. This suggests one way women’s disproportionate burden as “family health managers” (Melander 2023; Ranji and Salganicoff 2014; Reczek and Umberson 2012; Reczek, Gebhardt-Kram, and Umberson 2018; Reczek et al. 2020) and gendered logics affecting the experience of pain (Melander 2023) may be linked.
Women’s comments about pushing through discomfort connected to caregiving obligations and sacrificing for family. As Cristina said, “It hurts because sometimes I feel bad and I do things so that everyone will feel fine. And maybe they recognize it but they won’t tell me. So that makes me upset. It upsets me because I’m making a sacrifice, I’m feeling bad, and I’m not doing my stuff.” Cristina’s comment reflects feelings of being unappreciated and yet unable to change the dynamics or step away from the taken-for-granted responsibilities and identity of being a primary caregiver for a household.
Gendered expectations around caregiving also came up in stories about pain interfering with women’s ability to keep up with housework (see also Paxman 2021). Whereas men in their stories often focused on paid employment, women spoke about pain in terms of how it limited their ability to cook, clean, and go grocery shopping—as part of a second shift of unpaid household labor (Hochschild and Machung 2012). Melanie, a middle-aged white woman with a college degree, related, “Sometimes I am just in such pain or I’m in bed and so I can’t do things like make dinner or go get groceries or the normal sort of care giving things and that my husband and my son who lived with me have to take on that responsibility and take care of me as well when I’m in those sorts of—when I’m having those days or those periods.” This concern was generally absent from men’s accounts, as were discussions about caregiving responsibilities.
Masculine Ideals and Identity Threats
In contrast to women’s accounts of caregiving and sacrifice, men’s narratives emphasized toughness and conquering pain. For example, Jorge spoke about how he dealt with a painful injury saying, “No, no, that doesn’t get in the way for me at all. I mean, even yesterday I just tie[d] up my arm and bring a ton of concrete to the dump yard and use just one arm to get rid of it… . Even though I have a broken bone I just tie it up and go anyways and just try to reduce the pain. I don’t know. Pain is not going to slow me down, sickness is not going to slow me down, Coronavirus doesn’t scare me.” Ignoring pain was narrated as a means by which honor and male identity could be reasserted (see also Robinson et al. 2001). In another example, Peter remarked, “You know, I said, I’ve felt neck pain and back pain for twenty years. I said, I just don’t say anything about it. I take ibuprofen and I move on.” Extended periods of pain also seemed to be experienced as a threat to men’s identity and sense of self (Charmaz 1994) in a way that did not clearly manifest in women’s narratives. This is evident in Dan’s lament, that chronic pain shaped “who I’ve seemed to become.”
Avoidance of help-seeking was another common theme in men’s narratives (Keogh 2015). Men generally did not provide any explanation as to why they would not seek medical help when experiencing acute or chronic pain. Gustavo illustrated this by recounting how he responded to an injury and its consequences. He explained, “I did not go to the hospital. I treat it [shoulder injury] myself at the house. I remember I was skinny because I could not sleep due to the pain. No matter how I position myself at night the shoulder hurt. It hurt in every way I moved it so I lost my job.” Gustavo is a middle-aged Hispanic man who was working in a low-wage job at the time of his AVP interview. His decision to forgo medical care is stated matter-of-factly, demonstrating another way in which gendered expectations of self-reliance and stoicism are normalized and idealized. As Edward, an older white man, added, “I don’t go whine around for every ache and pain. It’s part of living and [living], is part of dying.”
Intersecting Precarity
Some accounts of pain connected to intersecting vulnerabilities such as class, race, gender, and age (Newman 2004; Collins 2002); sometimes as part of a challenging life trajectory narrative. For instance, a low-income Hispanic woman named Mariana shared the following account, connecting pain, childbirth, and institutional treatment: “I felt that it was coming out and a nurse was passing by, and I said to her. ‘Oh, excuse me, I need to be checked because I feel that I am relieving.’ And she says, ‘I’m telling a nurse now.’ ‘Oh, please, I feel it. What’s more, check me out, please check on me.’ I am so shameful and that day I was telling her that.” This echoes generations of research showing how poor experiences with health-care providers, concerns about disempowerment, and disparate treatment are a fact of life for Americans from the lower classes, women, and people of color.
Although the general patterns discussed in this article are consistent over the years of data collection, the challenges of the COVID era revealed hard choices and vulnerability. Joaquin, a Hispanic man with some college education, described how COVID-19 exacerbated the downstream effects of policy, the necessity of work, and the costs of illness:
And so pretty much I’m paying all this money for health care, which is mandatory by the way, especially in my state, I’m paying this for nothing, because I can’t even see my fucking doctor excuse my French, so I’m working in pain. And then my boss, I tell him, hey, I have to take one day off my foot is swollen. And legitimately he asked me have you seen the doctor, in order for me to get short-term disability or short-term leave, which I also need insurance for through my job, you have to see a doctor and be given a referral, and I can’t even see a doctor because the health care right now is down because of the limited quantities of space that they have. I’m kind of fucked over because of the pandemic I’m in a position where I’m just hurting myself, especially being an essential worker, it’s just hurting me. Unfortunately, I just have to live with it for now, I guess.
This statement, like many of the others, illustrates how pain narratives reveal complex inequalities shaping the social organization of suffering, revealed and exacerbated by the stressors of the pandemic.
DISCUSSION
Our findings are consistent with expectations that pain creates challenges and disruptions for Americans from varied backgrounds, that pain narratives invoke moral assessments of different response strategies, and that the content of narratives vary by gender and education in ways that reveal divergent experiences and challenges. Triangulating extant findings through a multimethod analysis is an important goal of this article (as well as open qualitative social science). Our findings also offer broader contributions to social scientific explanations that connect inequality to experience, research methodology, and social policy.
American Inequality and the Social Organization of Suffering
Our findings show how respondents’ pain narratives reveal similarities, differences, and inequities that organize experiences of pain and suffering.
First, our analysis shows various ways pain affects the lives of respondents. Their accounts reveal how both chronic and acute pain shaped workplace possibilities, interpersonal relationships, and respondents’ understanding of their roles and identities. Pain entered discussion as a practical dilemma that often required a response to resume activity patterns, which typically involved medical engagement or other strategies for numbing. In the wake of the opioid crisis, the use of narcotic painkillers was particularly charged, and framed in moral terms. This was part of a broader set of distinctions respondents made between legitimate and illegitimate, honorable, and stigmatized ways of managing pain. Concerns about the implications of being ill, unable to bear pain, using narcotics, or what outward appearance of suffering signified, were described as (or feared for the potential to become) anchoring aspects of social identity.15 Pain took on a widely acknowledged moral valence.
Second, our analyses show how aspects of social stratification and inequality in America— including gender and education (which we compare directly) and race and class (which emerge in narratives)— were associated with differences in narratives describing the origin and consequences of pain. Patterns revealed in networks and in-depth narratives reveal how subjective experiences, including complex phenomena like pain, can be objectively distributed in ways that map on to broader circumstances (such as economic precarity or disparate medical treatment) in ways that organize social suffering. AVP narratives highlight unequal challenges, treatment, resources, and beliefs about what it means to be in pain.
Available coping strategies reflected different constraints in life circumstances, but discussions of morality and distinction were seen across groups. Some responses were framed or recognized as admirable (such as working through pain, methodical sobriety), whereas others were framed as a marker of stigma (such as taking narcotic painkillers, letting pain become part of identity). Further, the social position of the person experiencing pain—often related to race, class, gender—was commonly connected in in accounts of whether pain was seen as legitimate by medical providers and others.
AVP pain narratives also offer insights into how inequality affects the origins of pain. Narratives highlighted how the risks of violence, workplace injury, stress, and the intersecting vulnerabilities of illness and material deprivation accumulated in ways that could radically alter life chances. This was most prominent in the narratives of women, especially those from marginalized groups, who described how pain reflects and exacerbates the burden of navigating work, caregiving, and medicine. These accounts referred to disparate medical and nonmedical resources as well as challenges in having concerns about pain taken seriously in medical settings. Perceptions of gendered mistreatment and dismissal were found across education levels.
Our analyses support earlier findings regarding the significance of gendered experiences of pain in several ways, including the challenges women report in establishing credibility in medical settings as well as the convergent challenges of managing pain and care work. When framing pain as distinction, people from varied backgrounds emphasized that persevering through pain and maintaining sobriety is admirable and honorable. However, women’s narratives focused on prioritizing others’ care over managing own’s own pain for the good of families, whereas men’s accounts emphasized bearing pain as a form of adversity, a test to be born silently with social stigma and identity at stake.
Table 2 provides a brief summary of some key themes identified in our network and narrative analyses that show broader patterns within and across groups.
Themes Related to Origins and Experiences of Pain
These findings support a key assertion of social scientific theories: challenges grounded in the body, including pain, are deeply intertwined with social inequalities. Inequalities shape not just the likelihood of circumstances that cause physical pain but how pain is understood and managed. The strategies that people ultimately deploy to manage pain, whether taking narcotic painkillers or toughing-it-out through suffering, distinguish or stigmatize them in the eyes of other people and societal institutions. However, this challenge is not faced in a level-playing field. Unequal opportunities in work, family, and medical institutions can reinforce racial, socioeconomic, and gender disparities. The narratives of the people interviewed in the AVP often evidenced a recognition of how both the origins of pain and their opportunities for navigating it reflected social inequalities even as these inequalities shaped their responses.
As a whole, these findings suggest that objective inequalities shape experiences of pain, while different ways of managing pain can create additional suffering, marginalization, stigma, or distinction (Abramson 2015; Bendelow 1993; Bourdieu 1984, 1999; Shim 2010). Differential vulnerabilities appear to be exacerbated by historical phenomena such as the fallout of the opioid crisis (Smirnova 2023).
Methodological Innovations and Limitations
Our analyses show how combining qualitative analyses with computational mapping of patterns can help reveal connections important to studies like ours, and which might otherwise be missed. A computational ethnography approach enabled us to situate narratives that reveal social mechanisms connecting inequality and pain against the backdrop of broader patterns in the AVP data. The process of doing so may offer insights for future analyses of large qualitative data sets (Abramson et al. 2018; Li and Abramson 2024). The analytical strategy section describes our procedures as well as the set of methodological techniques we used to effectively subset and classify text, combine computational pattern recognition with in-depth reading, and generate network visualizations. The appendix situates this approach along with other research paradigms.16
These study has several limitations. First, although the AVP data fit our questions, they were not generated prospectively for our project, which may limit the depth of pain narratives. Direct questions about acute pain, chronic pain, or social suffering will be useful for future work. Second, we used broad categories for our networks to address issues of complexity and data volume. This is because attempts to examine education-by-gender interactions, or map language by racial-ethnic identification, produced sparse corpi of text data. Although we discuss nuances that manifested in our qualitative analyses throughout and note that we do not reduce findings to network categories, increased data will allow more comparisons to be conducted with confidence.17 Third, it was difficult to assess interviewer effects or site-specific sources of bias at the time of writing. Fourth, the nature of the secure data sandbox and confidentiality limited our ability to generate interactive linked visuals or provide additional depth about respondents, which would be ideal in this genre of work. Nonetheless, we are confident that our findings reveal important aspects of social inequality and health and offer methodological resources for future work.
Policy Implications
Our findings reveal general patterns that show how American pain reflects inequalities. This is an important topic for policy, because it is another point of evidence showing the unequal burden of social suffering borne by vulnerable groups and the implications for health systems (Kleinman, Das, and Lock 1997; Farmer 1996). Social scientific examinations such as this article offer an avenue to understand broader patterns and can help identify ways policy might address inequities. For instance, our findings support the argument that policy needs to look at the unequal effects of not just the expansion of opioids (Mullins, Gilligan, and Bhattacharyya 2022) but also how their criminalization and stigmatization disproportionately exacerbate challenges with pain and life chances (Smirnova 2023). Our findings show that validation of pain in medical encounters is important to Americans, and yet people (particularly women) often feel ignored or delegitimized (Toye et. al 2021). Our analyses reveal examples where persistent pain exacerbates social vulnerabilities when unmanaged, but many forms of management are stigmatized and precarious (Anderson, Green, and Payne 2009; Mullins, Yong, and Bhattacharyya 2022; Janevic et al. 2017). Further, our work suggests that narratives remain an important source of data for health policy and that large-scale qualitative studies are valuable in this regard (Dohan et al. 2016). Analyses of what American voices have to say about pain in particular have implications for expanding equitable and just health policy at the level of government, clinics, and workplaces in the United States.
METHODOLOGICAL APPENDIX
Our approach to analyzing the AVP data is only one possible approach to qualitative and mixed-methods comparison. A key point of value for studies like the AVP is the potential for multiple uses for researchers from varied backgrounds and approaches. Rather than present our work as the only reasonable solution, we have always begun with the observation that qualitative social science has a rich and laudable history of multiple paradigms (Abramson and Gong 2020) and even though a large-scale data source such as the AVP maps on to our arguments for the utility of scaled qualitative studies, such work need not be seen as an a priori replacement to more traditional qualitative inquiry (Abramson and Dohan 2015).
Epistemic Position and Logic
Given perennial debates about the role and utility of qualitative methods, it is important to situate our work to both be reflexive about our use of methods and avoid issues of misspecification. Qualitative approaches have included diverse scientific and humanist traditions in post–World War II social science, sometimes leading to assiduous debates about what makes research qualitative, as well as heated debates about the role of interviews and field research in an era of big data (Small 2021). Our work proceeds in accordance with the broad principles of methodological pluralism, which suggest that multiple modes of inquiry can aid in producing a fuller understanding of the phenomena of sociological and policy importance, even under the umbrella of qualitative methods (Abramson and Gong 2020; Lamont and Swidler 2014).
Our research was conducted in accordance with the principles of contemporary realism, and aims to identify patterns that can be seen by other researchers’ qualitative, quantitative, and mixed-methods projects. A core advantage of qualitative methods in the realist paradigm is the ability to examine phenomena with a level of depth that cannot be captured using other approaches (Sánchez-Jankowski and Abramson 2020). We also recognize that critical, humanist, constructionist, and exploratory approaches are used in qualitative inquiry in fields such as anthropology and sociology, with goals such as critiquing society or generating ideas for survey research, and have made important contributions in this regard (but see also Burawoy 1998; Clifford and Marcus 1986; Glaser and Strauss 1967; Collins 2000, 2002). Although these approaches have yielded important insights and correctives, the benchmark we apply to our qualitative works is the ability to reliably capture patterns and processes that are important and might be obscured or hidden using other approaches. This is particularly valuable in examinations linking social inequalities, response strategies, and beliefs, where our goal is to provide scholarly insights that can also inform evidence-based policies.
A core limitation of qualitative inquiry in the conventional scientific tradition has always been related to scale and sampling limitations that impede the ability to generalize in a probabilistic way (Abramson and Sánchez-Jankowski 2020; Small 2009). Related issues include the absence of tools to make sense of large volumes of qualitative data without quantitative or computational reductionism (Abramson and Dohan 2015); the difficulty of managing complex human subjects data for open science (Murphy, Jerolmack, and Smith 2021; Freese 2007); the unequal resources for conducting qualitative research at scale (Abramson and Dohan 2015; Bernstein and Dohan 2020); the historical paucity of analytical approaches for linking broad patterns and nuanced mechanisms empirically (Abramson and Sánchez-Jankowski 2020; Li, Dohan, and Abramson 2021); the lack of clarity about what qualitative researchers of different traditions aim to do in their comparative analysis (Abramson and Gong 2020); and the general contestation and often combativeness of the qualitative field. However, many of us remain drawn to these methods because they reveal important aspects of the world—how people think about, experience, and navigate the contours of American inequality—with a precision and sensitivity to context that has to date not been captured in surveys, analyses of administrative data, historical methods, found data, or experiments. In engaging with these matters, our article also endeavors to show that the methodological challenges are not insurmountable, and qualitative research might pursue multiple modes of response, as part of a productive and respectful dialogue as seen in this double issue.
We have argued that at least some of the technical challenges of “big (qualitative) data” are becoming more manageable in the computational era, given that technology allows both scaled inquiry and possibilities for data processing that go beyond the traditional possibilities of computer-assisted qualitative data analysis (for example, Dohan and Sánchez-Jankowski 1998). To this end, in this article we deployed techniques from computational social science while articulating tools that may have utility for others who share analytical aims (but see also Abramson and Dohan 2015; Abramson et al. 2018; Li, Dohan, and Abramson 2021; Li and Abramson 2024). Yet, without thoughtful deployment, technical complexity does not in itself advance social inquiry, and for our part we have tried to explain our decisions and trade-offs throughout this work.
We are grateful that the American Voices Project has provided a generative locale for deploying some of these methods in alignment with the goals of building an open qualitative social science. We hope this initiative will continue to produce not only useful empirical findings but thoughtful methodological dialogue.
Computational Information and Replication
Text preprocessing, word embeddings, and semantic network analysis are implemented in Python 3.9.5 using “gensim==4.2.0”, “matplotlib==3.4.2”, “networkx==2.5.1”, “nltk==3.6.2”, “pandas==1.2.5”, and “spacy==3.0.6”.
The network visualizations were created in R 4.2.3 using “ggplot2 (3.4.0)”, “igraph (1.3.5)”, “ggraph (2.1.0)”, “dplyr (1.1.0)”, “RColorBrewer (1.1-3)” packages.
For replication code, please contact the authors directly to facilitate sharing in accordance with American Voice Project protocols.
FOOTNOTES
↵1. This article examines physical pain in a broad sense, including both chronic and acute variants. In a prospective study design, examining chronic pain (pain that lasts more than three months) has the advantage of being a condition in and of itself, whereas acute pain is more likely a symptom (possibly fleeting) of something else (Siddall 2013; Zajacova 2021a). Acute pain is more difficult to sample. Because the AVP does not select on people with pain, examining narratives of both chronic and acute pain allows us to cast a broad net to uncover potential commonalities that might be missed by a narrower focus, including connections to inequality that may be obscured by a priori boundaries that may not reflect experiences (Cicourel 1982). Acknowledgment is also growing of important similarities, including that both classes of pain can catalyze neuronal remodeling, that experiences of both are informed by individual beliefs and attitudes (Carr and Goudas 1999), and that chronic as well as acute pain co-occur with other forms of suffering such as anxiety and depression (for example, De La Rosa et al. 2023; Carr et al. 2005). More broadly, this follows our goal of using the case of pain to understand connections between inequality, experience, and suffering (Bourdieu 1984; Kleinman, Das, and Lock 1997).
↵2. The reported prevalence of both acute and chronic pain has increased over the last twenty years in the United States (Zajacova, Grol-Prokopczyk, and Zimmer 2021a). Estimates indicate one in fourteen American adults experience “high impact” chronic pain, which means their life and work activities are limited for substantial periods of time most days or everyday, and many experience intermittent pain (Dowell et al. 2022; Yong, Mullins, and Bhattacharyya 2022). This has implications for socioeconomic institutions as well as social suffering. By the early 2010s, chronic pain was estimated to cost between $560 and $635 billion in direct medical costs, lost productivity, and disability (Gaskin and Richard 2012). By 2019, estimates posit an annual loss of $79.9 billion in lost wages and an impact on GDP of $216 billion (Yong, Mullins, and Bhattacharyya 2022). Chronic pain is one of the most common reasons American adults seek medical care (Lara-Milan 2021; Schappert and Burt 2006). Some suggest the costs associated with pain exceed those of other leading conditions (Gaskin and Richard 2012).
↵3. The presence of chronic pain is treated as a condition unto itself; epidemiological estimates suggest that this kind of pain affects approximately one in five adults in the United States or approximately fifty million people (Yong, Mullins, and Bhattacharyya 2022). Chronic pain can exacerbate depression, anxiety, and everyday challenges, resulting in tremendous human suffering that extends beyond physical discomfort, expenses, and broader economic costs (IsHak et al. 2018; De La Rosa et al. 2023; Sampson et al. 2015; Siler, Borneman, and Ferrell 2019).
↵4. Over the last decade, an ongoing epidemic of opioid use emerged against this backdrop. A number of scholars argue that some or much of this epidemic was driven by multiple factors, rather than just pharmaceutical entrepreneurship and opportunism. These include the increasing prevalence of chronic pain (Zajacova, Grol-Prokopczyk, and Zimmer 2021a, 2021b), the stress of declining economic opportunities (Case and Deaton 2020), disparities in addiction and addiction treatment (Hansen, Netherland, and Herzberg 2023), the medicalization of suffering and the subsequent criminalization of coping strategies (Smirnova 2023), and a patchwork market-based health-care system that enabled pharmaceutical entrepreneurship to market addictive pain medications (Currie and Schwandt 2021). Increases in opioid prescriptions for pain were accompanied by opioid related substance use disorders as well as deaths (Phillips, Ford, and Bonnie 2017). The opioid epidemic has led to scores of deaths, suffering, a moral panic (Mendoza, Rivera, and Hansen 2019), and increasing criminalization and surveillance (Sue 2019) that have been particularly devastating to vulnerable populations (Bridges 2020) and make management of pain more fraught for the most vulnerable.
↵5. Suffering refers to broader experiences of distress and hardship, continuing beyond how people categorize physical pain. Social suffering includes both individual and collective aspects of pain, which offers an empirical entrée to the topic (Farmer 1996; Bourdieu 1999; Siler, Borneman, and Ferrell 2019).
↵6. Reports of levels of pain have been empirically connected to both demographic shifts and social stratification. One group, older adults, form a growing proportion of the population, report high rates of pain, and describe how pain is important to their lives in ethnographic research (Abramson 2015; Domenichiello and Ramsden 2019). Americans with less than a high school degree are the most likely subgroup to report experiencing severe pain that effects their life, work, and family most days (Mullins, Yong, and Bhattacharyya 2022). Other demographics that disproportionately suffer from sustained periods of pain include nonwhites, women (Mullins, Yong, and Bhattacharyya 2022; Bartley and Fillingim 2013), poor and working-class individuals (Jay et al. 2019; Mullins, Yong, and Bhattacharyya 2022).
↵7. We use the term expectations rather than hypotheses given conventions for discussing qualitative data, but these propositions are consistent with the concept of a hypothesis in the broader sense of expected outcomes, which can be evaluated in non-arbitrary ways. The necessary caveat is that regardless of language, all such inquiry is bound by human and technical limits, so our analysis speaks to the plausibility of these expectations rather than providing definitive confirmation or falsification. This maps on to a broadly fallibilist approach to human inquiry with affinities to the Bayesian approaches, computational social science, and an iterative approach to realist inquiry that underpins our work (see Abramson and Sánchez-Jankowski 2020; Sánchez-Jankowski and Abramson 2020).
↵8. The data set is described at length in the introduction to this volume (Edin et al. 2024, this issue).
↵9. Although this approach has its origins in goals of “scaling up” qualitative methods to support large comparative qualitative projects and reveal patterns, it has parallels with CSS approaches that scale down big data to examine qualitative narratives alongside patterns (DiMaggio 2015; Nelson et al. 2021; Lichtenstein and Rucks-Ahidiana 2023; Breiger 2015; Sauder, Shi, and Lynn 2024, this issue; Zilberstein et al. 2024, this issue; Chu and Lee 2024, this issue).
↵10. Even with oversampling, racial-ethnic group focused analyses, which also map on well to literatures we engage with, created challenges for modeling networks due to sub-sample size limitations. We also recognize simplified operationalizations of education and gender do violence to the complexity of the underlying concepts, but some compression was necessary to allow comparability given limits on the methodological and technical tools available to us at the time of writing. We address this by using these categorizations not as definitive individual attributes, but as a broad basis allowing some aggregate comparison between qualitative sets or corpi of text. Narratives were not reduced to these criteria, and relevant quotes that did not fit neatly into categorizations were evaluated separately insofar as they relate to our broader research questions.
↵11. Seed words include ibuprofen, herniate, oxycodone, hydrocodone, discomfort, painkiller, morphine, stimulator, curvature, anesthetic, oxycontin, sciatica, spine, sciatic, cedar, inflammatory, ache, vertebra, spinal, and cortisone, with a cosine similarity to pain ranging from 0.444 to 0.353. As we describe later, we compressed pain medication into opioid and non-opioid varieties using a medical dictionary list. It is possible that there are some false positives, but these were weeded out manually for qualitative analysis as discussed in (Li, Dohan, and Abramson 2021).
↵12. This was not ideal because technical issues were associated with the data set size and we had no direct way to link with more advanced language models. This, as well as the weeding out of false positives, accounts for some of the numeric divergences in set sizes. Other CAQDA software became available later in the project, but much of our qualitative analysis was already completed, and no current off-the-shelf software provides an ideal solution.
↵13. Interviews with missing data on these core measures were excluded from analysis for this article. Although numbers show variation in the percentage of respondents mentioning pain by gender identity (for example, 81 percent identifying as female versus 74 percent identifying as male), our focus here is demonstrating that discussion of pain occur at high rates across groups, to allowing a comparison of how pain is discussed. In our analysis of interview content, we further specify the number of interview segments (a paragraph of uninterrupted response by the respondent in an interview) for our computational analyses. In the context of our focus on narrative structure and content, the raw number of segments methodologically demonstrates adequate scope for modeling rather than substantively measuring variation in verbosity by gender or education. However, because we are modeling within groups of interviews using methodologies focused on word position within categories of respondent, the observed differences focus on connections unlikely to be fundamentally changed given differences found in research. As noted, for qualitative analyses, our findings rely on a broader human reading of interviews and relevant text.
↵14. Our justifications and methodological reasons for compressing categories are discussed in the methods section. We recognize that these categories do not capture all important variation, but provide a starting point for analytical comparisons, presented alongside our more detailed qualitative analyses. In this case, the strategy provides adequate set size for comparisons of language patterms, maps on to a key component of class and cultural health capital (Shim 2010), and has been documented as an important source of distinction for both individuals and institutions. This also mirrors key variation that emerged inductively in our qualitative analysis.
↵15. Subjects may hide pain because its underlying condition (such as aging or disease) can be seen as discreditable—speaking negatively to a person’s identity (Goffman 1963)—but not immediately visible and “discrediting.” Others might see being direct about pain as candid, admirable, or efficacious depending on whom they are interacting with. Empirical research demonstrates that both communities and medical contexts shape responses to pain, with the latter historically and contemporarily involved in dismissal or mistreatment of pain among minoritized populations (Biedma-Velazquez et al. 2022; Morales and Yong 2021; Hoffman et al. 2016).
↵16. The combination of semantic networks and qualitative analyses of narratives were complementary for connecting general language patterns across groups (represented as semantic networks) and the narratives shared by our subjects (represented as qualitative narratives). Conceptually, the networks can be thought of as a visual representation of language structures and basic themes (for example, medical engagement), and in-depth narratives show how respondents draw connections (for example, women’s pain is ignored by doctors). Our use of interpretive coding (Abramson and Dohan 2015) provides a link between these levels, and is key to triangulating patterns across levels of data.
↵17. We are also aware of the danger of essentializing racial, gender, and SES cultures, as well as the potential for aggregation errors, which added to our concern about drawing generalizations where the data were sparse.
- © 2024 Russell Sage Foundation. Abramson, Corey M., Zhuofan Li, Tara Prendergast, and Martín Sánchez-Jankowski. 2024. “Inequality in the Origins and Experiences of Pain: What ‘Big (Qualitative) Data’ Reveal About Social Suffering in the United States.” RSF: The Russell Sage Foundation Journal of the Social Sciences 10(5): 34–65. https://doi.org/10.7758/RSF.2024.10.5.02. Please direct all correspondence to: Corey M. Abramson, at corey.abramson{at}rice.edu, Department of Sociology, MS-28 Rice University, P.O. Box 1892, Houston, TX 77005.
Open Access Policy: RSF: The Russell Sage Foundation Journal of the Social Sciences is an open access journal. This article is published under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.
REFERENCES
In this issue





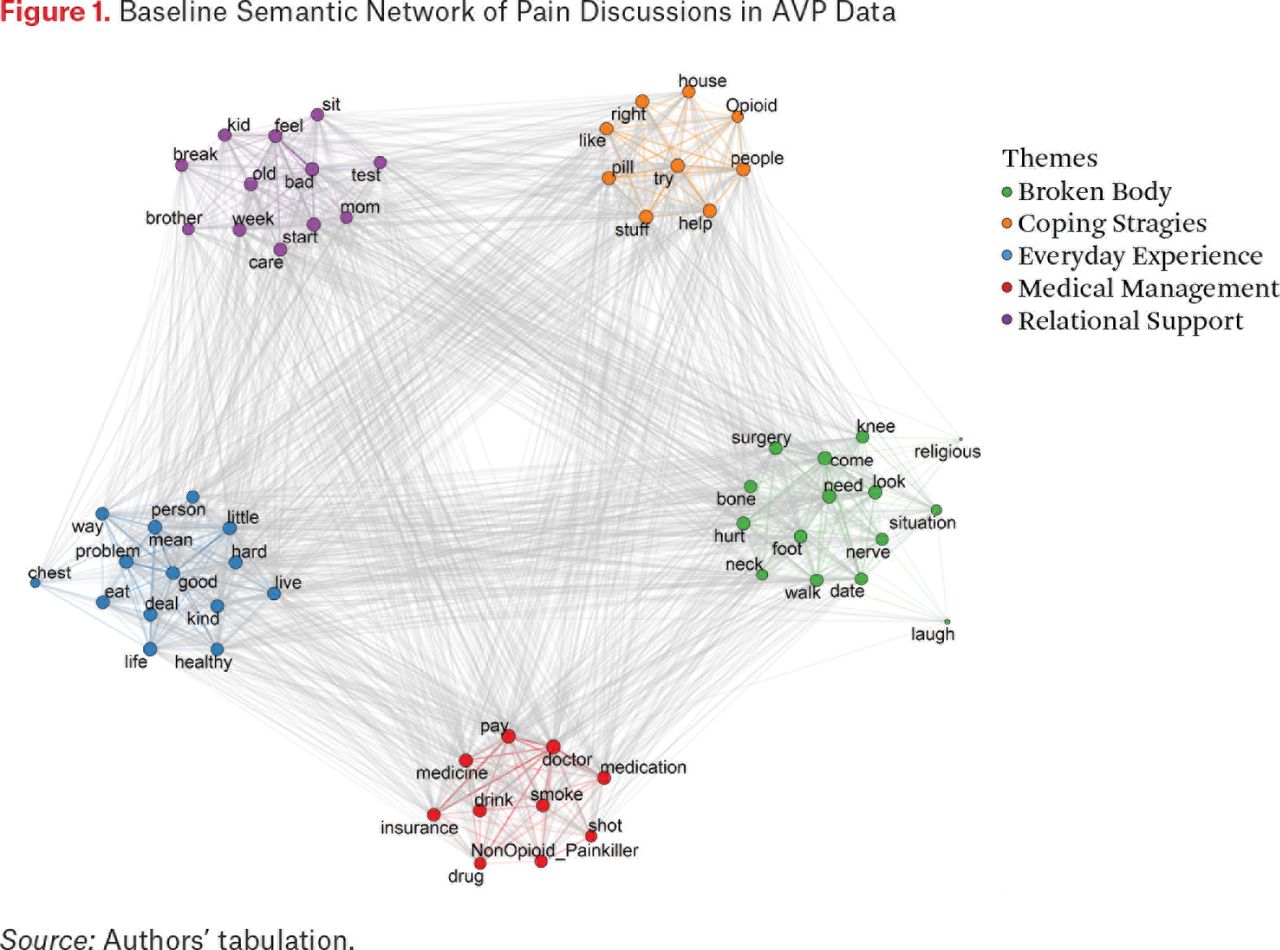{kind=link}
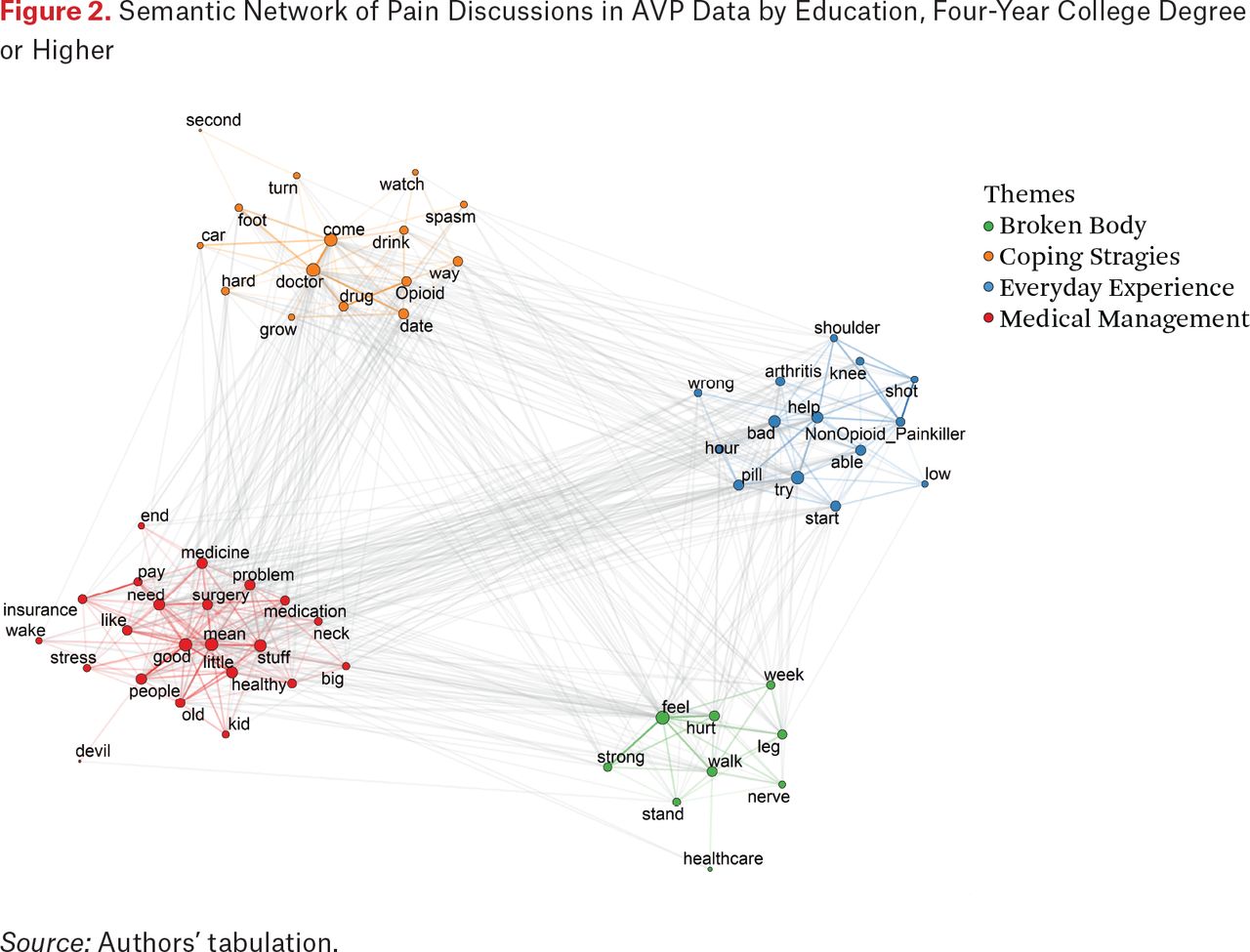{kind=link}
{kind=link}
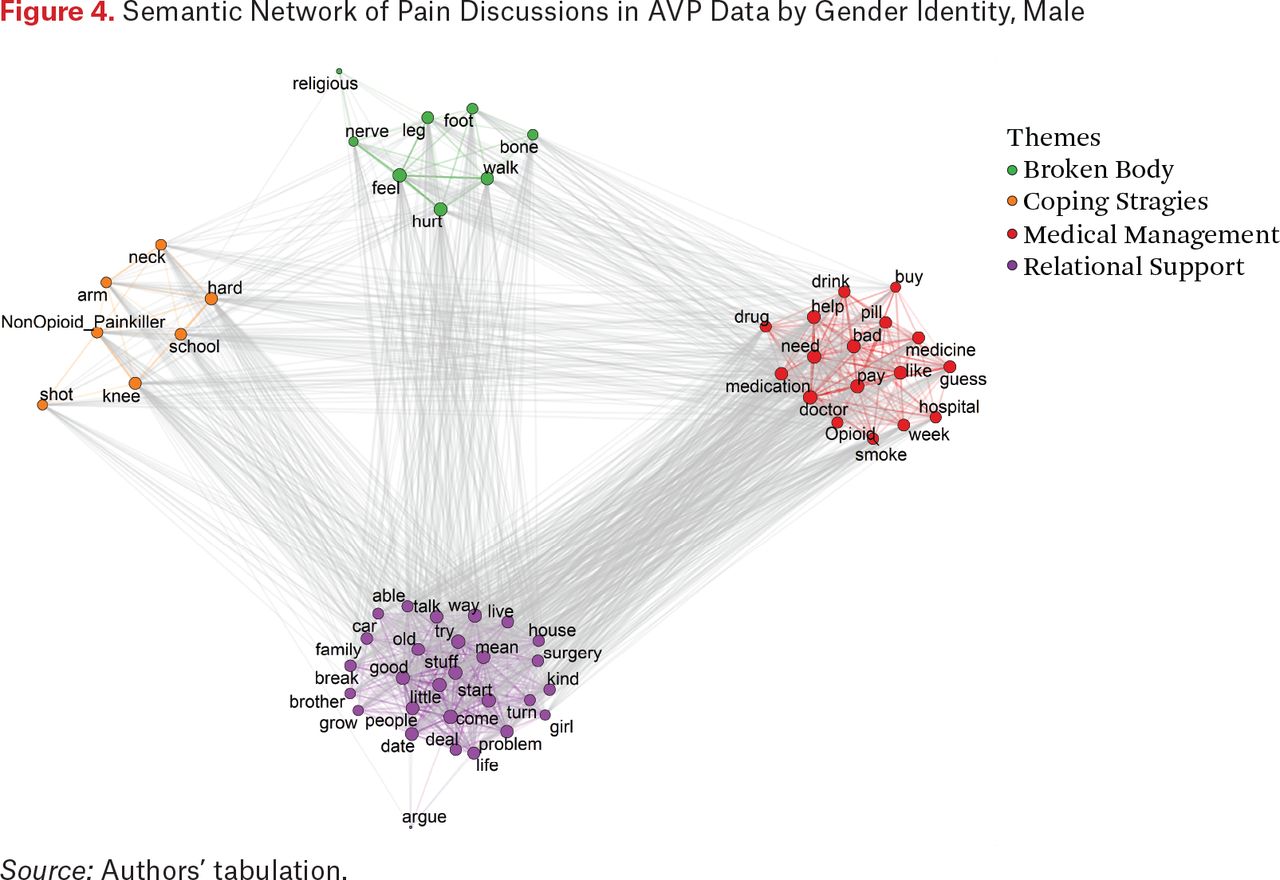{kind=link}
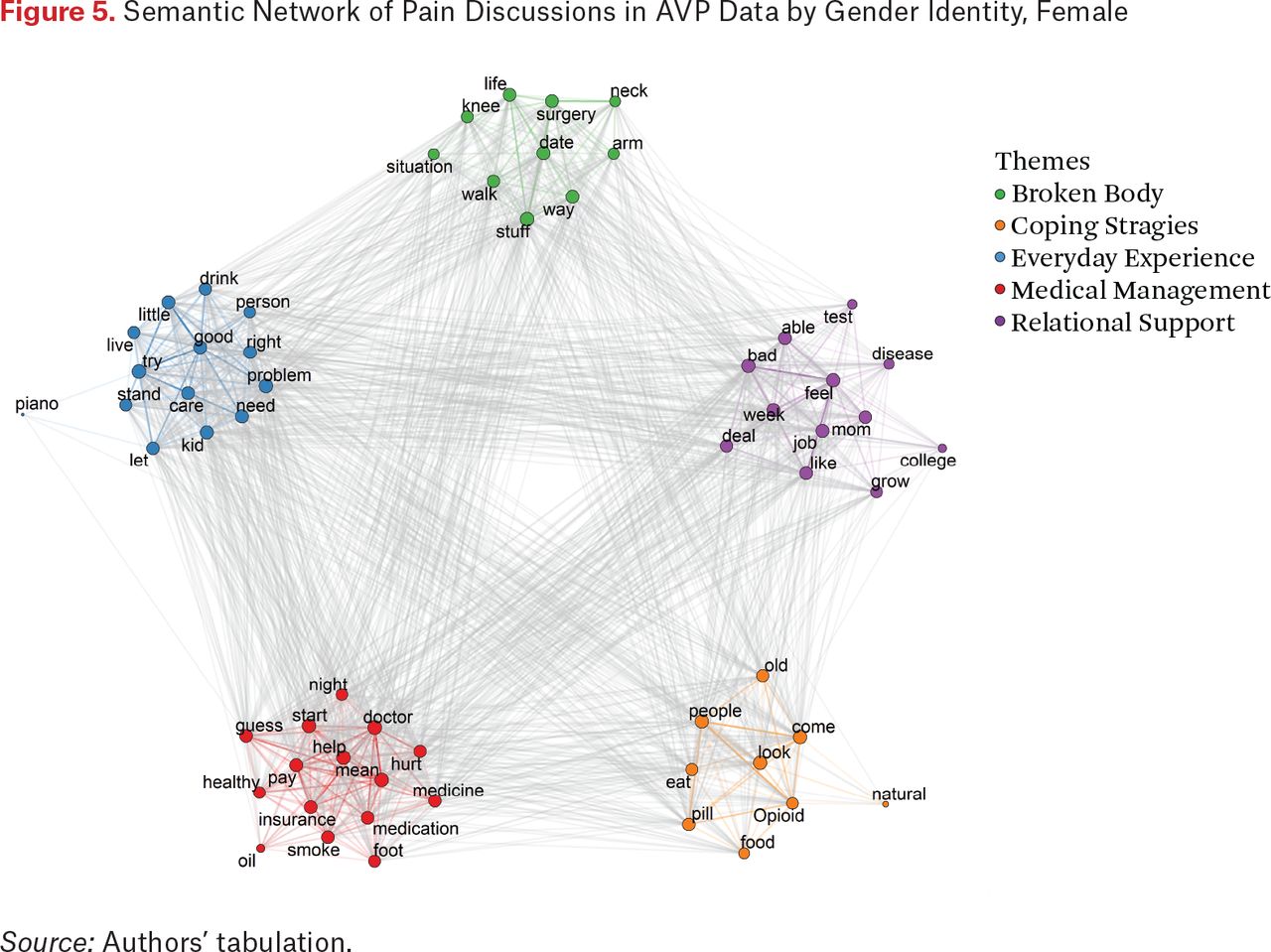{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.