
Abstract
Using National Vital Statistics Birth and Fetal Death Data from 1995 to 2020 linked to county-level information on wildfires, we use variation in wildfire timing to examine how effects of wildfire exposure on infant health vary by maternal education. Results indicate that wildfire exposure increases the likelihood of low birth weight and fetal death, but effects vary by both trimester and maternal education. Mediation analyses suggest the variation by maternal education reflects selective survival and unequal sensitivity, rather than differential parental response to wildfires. In addition, mediation analyses suggest that maternal behaviors explain a greater share of the relationship between wildfire exposure and infant health than air quality. Wildfires may therefore reduce infant health through stress.
Prenatal wildfire exposure is associated with poorer infant health (see Amjad et al. 2021 for a review; Jayachandran 2009; Requia et al. 2022), but less is known about why. The association could reflect air quality, stress, or selective exposure to wildfires. Mixed evidence in existing research could reflect a number of limitations, including bias due to sample exclusions and confounding (Amjad et al. 2021), as well as potential heterogeneous effects by maternal socioeconomic status (SES) (Cozzani, Triventi, and Bernardi 2022).
Wildfires are increasing in frequency and intensity in the United States (Dennison et al. 2014; Halofsky, Peterson, and Harvey 2020). The increasing prevalence of wildfires in more areas of the United States makes understanding their health and inequality implications urgent and relevant for a growing swathe of the country. We contribute to existing research by, first, examining wildfires throughout the United States from 1995 to 2020 to include a more representative sample than studies that limit analysis to one location or time period; second, including births from the full distribution of health outcomes to avoid potential exclusion bias (Amjad et al. 2021); third, examining heterogeneous effects by maternal SES and conducting mediation analyses to understand mechanisms; and, fourth, examining effects on fetal death to explicitly examine selective survival.
We use National Vital Statistic Birth Data for 1995 through 2020 linked to county-level wildfire and air quality data to examine how the relationship between wildfire exposure and infant health varies by maternal education—a key SES indicator that is consistently associated with infant health. We examine several potential mediators, including prenatal care and health behaviors, to help understand that variation. We address two research questions: Does the relationship between prenatal wildfire exposure and infant health vary by maternal education? Do prenatal care or health behaviors explain variation by maternal education?
Baseline infant health and access to care could vary by local risk of wildfires, which would bias naïve estimates of the relationship between wildfire exposure and infant health. We use two strategies to address this concern. First, we use fixed-effects models to adjust for stable differences in infant health between counties and national changes in infant health over time. Second, we use geocoded wildfire data and take advantage of variation in their timing to estimate causal effects of wildfire exposure on infant health.
To preview our results and consistent with existing work, wildfire exposure during pregnancy is related to poorer infant health. Using variation in wildfire timing within counties, we find that effects of wildfire exposure vary by both trimester and maternal education, with more negative effects among low-SES mothers exposed during the second trimester. These results hold under a series of sensitivity analyses, including controlling for air quality and seasonality of births and assuming all pregnancies last nine months. Estimated effects on fetal death and mediation analyses suggest that the variation by maternal education could partly reflect selective survival and unequal sensitivity, rather than differential parental response to wildfires.
BACKGROUND
Exposure to environmental toxins, including air pollution and wildfires, has negative implications for health at every life stage through multiple and compounding effects on the immune, neurological, and endocrine systems (Torche, Fletcher, and Brand 2024, this issue; Crinnion 2000; Sexton et al. 1992). Exposure to environmental toxins or insults are particularly harmful during early life and even during pregnancy (Conley and Bennett 2000; Goosby 2013; Haas 2008; Palloni 2006; Pizzorno and Murray 2020). For example, lead exposure during childhood has been linked to cognitive impairment and lower test scores in adolescence and adulthood (Aizer et al. 2018; Bellinger et al. 1991; Mazumdar et al. 2011). Flood exposure among rural, school-age children in India is related to lower math and reading skills (Khalid et al. 2024, this issue). Similarly, exposure to famine in utero has been linked to chronic health problems, including obesity, cardiovascular problems, and cognitive functioning later in life (de Rooji et al. 2010; Roseboom, de Rooji, and Painter 2006; Schulz 2010).
Exposure to environmental shocks has negative implications for infant health through multiple pathways and the effects can vary depending on the timing of exposure during pregnancy. For example, exposure to an earthquake during gestation reduced infant health through maternal stress, but only among those exposed during the first trimester of pregnancy (Torche 2011). Exposure to iron mining residues due to a collapsed dam during the third trimester reduced infant birth weight and increased infant mortality (Carrillo et al. 2020).
Air pollution is one potential mechanism (Currie, Neidell, and Schmieder 2009; Ritz et al. 2007, 2000; Liu et al. 2003; Maisonet et al. 2001; Rogers et al. 2000; Ritz and Yu 1999; Lee et al. 2003). In addition to air pollution, wildfires could also influence infant health through other mechanisms, such as maternal stress, pregnancy complications, and disrupted prenatal care, family, and work routines. Wildfires increase the risk of maternal PTSD-like symptoms and maternal stress over family separation, childcare, and strained spousal relationships (Verstraeten et al. 2021; Bremault-Phillips et al. 2020). Maternal stress is also related to pregnancy complications, such as hypertensive disorders, and may cause premature delivery (Currie and Rossin-Slater 2013; Oni et al. 2015). Finally, wildfires can limit pregnant women’s physical mobility and disrupt their routines, roles, and occupational schedules (Pike et al. 2022).
Poor infant health has long-term consequences, resulting in higher risk of disability, mortality, and poor health later in life as well as lower educational and labor-market outcomes (de Jong et al. 2012; Swamy, Ostbye, and Skjaerven 2008; Aizer et al. 2018; Bellinger et al. 1991; Mazumdar et al. 2011; Baranowska-Rataj et al. 2022). Poor infant health, including low weight births, are also expensive, with one underweight hospital birth costing approximately $24,000 more than a normal weight birth (America’s Health Rankings 2021). Exposure to wildfires and other air pollution is increasing, making it important to understand how to mitigate their effects on infant health.
Variation in Environmental Effects on Infant Health
The effects of environmental insults on infant health can vary depending on factors other than timing of exposure, particularly parental socioeconomic status. Socioeconomic status could alter the effects of environmental insults through variation in exposure, sensitivity, survival, or parental responses (Cozzani, Triventi, and Bernardi 2022).
Effects could be larger among low-SES infants if mothers are exposed to more wildfires or poorer air quality because of the proximity, duration, or intensity of wildfires. People with fewer resources are exposed to more air pollution than higher-SES populations at home and at work (Tessum et al. 2021, 2019; Ferguson et al. 2020; Hajat, Hsia, and O’Neill 2015). However, exposure to wildfires may be more equal because wildfires occur in areas where those across the SES distribution are likely to live, including suburban and rural areas. We assess exposure rates by SES in our sample and find relatively similar exposure rates (see tables A.3 and A.4 in the online appendix).1
When exposure is equal, negative effects of wildfire exposure may still be stronger among low-SES infants because of higher sensitivity or lower resilience among low-SES mothers. For example, low-SES mothers may have more severe pre-existing conditions and risk factors, including exposure to chronic stress, that increase the likelihood of negative health outcomes from stress or poor air quality (Torche 2018; Martins et al. 2004; Turner and Avison 2003; Prescott et al. 2003; Chen, Krewski, and Dales 2001; Jerrett et al. 2004; Phelan and Link 2005). Alternatively, exposure to higher air pollution or stress could have more detrimental effects among higher-SES mothers because of lower resilience or higher sensitivity from limited earlier exposure (Genereux et al. 2008; Feder, Nestler, and Charney 2009; Cagney et al. 2016).
Low-SES mothers have fewer resources available to avoid wildfires, avoid poor air quality days, access health care to prevent and address health concerns, and reduce stress through healthy coping mechanisms (Link and Phelan 1995; Phelan and Link 2005; Torche 2018; Elo 2009). This perspective suggests that those with higher SES have a flexible set of resources—money, knowledge, time—that they leverage to maintain better health as the policy and environmental context change (Torche, Fletcher, and Brand 2024, this issue; Link and Phelan 1995). In the case of wildfires, effects could be larger among low-SES mothers if they are less able to access prenatal care or stay indoors on unhealthy days (House et al. 1990; House 2002; Lieberson 1985; Link and Phelan 1995; Preston and Taubman 1994; Zeng, Gu, and Land 2007).
Exposure to environmental insults, including wildfires, could increase the chances of fetal death, resulting in the survival of healthier and more robust infants. If wildfires increase fetal death, then their negative effects on infant health would be underestimated when examining only live births because the resulting births are healthier (Bharadwaj et al. 2013). Selective survival could help explain varying effects by SES if wildfires have different effects by both maternal SES and the timing of exposure. For example, environmental insults could increase the likelihood of fetal death early in pregnancy for low-SES births, leaving healthier low-SES fetuses relative to high-SES fetuses. This form of selective survival would predict negative health effects of early exposure for low-SES pregnancies, followed by weaker effects of later exposure among low-SES pregnancies. Because high-SES pregnancies are less selected, selective survival would predict more negative health effects of late-pregnancy exposure among high-SES births. Because most studies examine live births, little research has directly examined selective survival as a potential explanation for varying effects of environmental insults (Cozzani, Triventi, and Bernardi 2022).
Wildfires vary in their timing and location. The increasing prevalence of wildfires in more areas of the United States makes understanding their health implications urgent and relevant for a growing swathe of the country (Dennison et al. 2014; Halofsky, Peterson, and Harvey 2020). As wildfires occur in more areas throughout the country, it is becoming difficult for women across the SES distribution to avoid them entirely. We use variation in wildfire timing to estimate effects of wildfire exposure on infant health. We build on work by Marco Cozzani, Moris Triventi, and Fabrizio Bernardi (2022) and Florencia Torche and Andres Villarreal (2014) by explicitly examining mechanisms, including selective survival, to understand variation in effects of environmental insults by maternal SES. Based on this review, we pose two hypotheses:
Hypothesis 1: Wildfire exposure has negative effects on infant health outcomes.
Hypothesis 2: The negative health effects of wildfire exposure are larger for less-educated mothers.
METHODS
Mothers with more resources, including education and health knowledge, are more likely to live in counties with higher-quality air and less pollution (House et al. 1990; House 2002; Lieberson 1985). Rates of prenatal exposure to wildfires are relatively similar by SES (see tables A.3 and A.4), but baseline differences in local air quality, health-care access, or other resources could bias naïve estimates of the relationship between wildfire exposure and infant health. To address such differences, we limit the main analyses to counties with a Class G wildfire (those that burned at least five thousand acres), taking advantage of variation in the timing of wildfires and the timing of exposure relative to conception. We use fixed-effects models to adjust for stable differences in infant health between counties and geocoded wildfire data to test whether infant health changes with wildfire exposure within the same county.
Data
National Vital Statistics System (NVSS) birth data provide administrative infant health and prenatal care information for each live birth in the United States and include information on maternal education and county of residence. We use restricted NVSS data, which include maternal county of residence. We take a 10 percent random sample of singleton births, with information about infant health and maternal characteristics, born each year from 1995 to 2020. We limit analyses to singleton births because multiple births (such as twins or triplets) are not randomly distributed by maternal education and have lower measures of infant health.
NVSS fetal death data provide information about fetal deaths (pregnancies that did not result in a live birth, also called stillbirths or miscarriages) in the United States, which we use to examine potential selective survival. Fetal death data include information about maternal education and county of residence in the restricted data, but do not include induced terminations of pregnancy (abortions) and in most states do not include deaths early in pregnancy (before twenty weeks of gestation or less than 350 grams). We use all singleton fetal deaths and, because we take a 10 percent random sample of live births but not of deaths, we assign a weight of ten to each sampled birth observation and a weight of one to each death observation for analyses examining fetal death. Maternal education is not available between 2007 and 2013, so analyses examining fetal death include those from 1995 to 2006 and from 2014 to 2020.
We link individual NVSS birth and fetal death data to county-level data on air quality and wildfire timing and severity using county Federal Information Processing System (FIPS) codes for maternal county of residence. Air Quality Index (AQI) data provide annual county-level data on air quality from the U.S. Environmental Protection Agency (EPA) for 1995 through 2020 (EPA 2021). AQI values are based on daily information recorded from monitors throughout the United States. In the time period we examine, EPA provides AQI data for approximately half (47 percent) of U.S. counties. These monitors record particulates and toxic gases or matter in the air. The EPA reports annual county-level air quality statistics, including 90th percentile and maximum AQI and the number of unhealthy days in a county during the year. Higher AQI values indicate higher pollution and lower quality air. According to the EPA, AQI values between 0 and 50 are good and those above 50 are unhealthy to varying degrees.
Wildfire data are from Monitoring Trends in Burn Severity (MTBS 2022), which is conducted by the U.S. Geological Survey Center for Earth Resources Observation and Science and the USDA Forest Service Geospatial Technology and Applications Center. MTBS data provide information about the location, timing, and burn severity of large fires throughout the United States, including fires that burn at least five hundred or one thousand acres in the eastern and western United States, respectively. Wildfire locations are geocoded using ArcGIS Pro, spatially joined to the county in which they began, and linked to NVSS and EPA data using county FIP codes. To focus on the most severe wildfire in each county-year, we include wildfires that burned the largest number of acres in each county-year from 1995 to 2020. We further focus our analyses on Class G fires that burn at least five thousand acres. This results in a sample of 2,890 large wildfires across county-years from thirty-seven states, with multiple wildfires in counties over time (only 237 counties had one wildfire over the period examined). To allow event study analyses, we link wildfire data to the 10 percent random sample of singleton births in the same county in the year before, the year of, and the year after the wildfire, yielding a sample of 1,389,357 births. Figure A.1 shows the distribution of wildfire severity by month and by year. These figures show increasing severity over years as measured by the number of acres burned and percent of county acres burned. Wildfires that started in September are the most severe, potentially because they occur in the dry period following summer.
Measures
Primary dependent variables are based on NVSS birth and fetal death data and measured as low birth weight (less than 2,500 grams) and fetal death. The low birth weight threshold identifies infants at high risk for poor health in childhood and later life (Conley et al. 2003; Johnson and Schoeni 2011; Institute of Medicine 2003). Fetal death (also called stillbirth or miscarriage) allows explicit examination of selective survival and is an indicator for whether the observation is a live birth (in the NVSS birth data) or did not result in a live birth (in the fetal death data). Fetal death and low birth weight are not mutually exclusive and approximately 81 percent of fetal deaths are also low birth weight. Sensitivity analyses examine preterm birth (less than thirty-seven weeks), birth weight (grams), gestational length (weeks), and intrauterine growth restriction (under the 10th percentile of birth weight for gestational age) to examine continuous outcome measures and to allow for downward trends in birth weight over time (Oken et al. 2003). Gestational length is based on last missed period before 2014 and obstetric estimate since 2014.
The primary independent variables are indicators for wildfire exposure during the first, second, or third trimester. Exposure timing is measured based on wildfire start date and county, maternal county of residence, and estimated conception date, calculated as birth date minus gestational length. First trimester exposure is coded 1 if a wildfire started in the mother’s county of residence during the first three months of gestation and 0 otherwise. Second trimester exposure indicates whether a wildfire started during months four through six of gestation, and third trimester exposure indicates whether a wildfire started after six months of gestation and before birth. Date of conception is measured with error, but measuring wildfire exposure by counting backward from birth date is biased due to variation in gestational length (Currie and Rossin-Slater 2013). Premature births could be inaccurately coded as exposed when calculating wildfire exposure based on birth date. We calculate conception month since wildfire ignition date to compare infant health over time relative to the wildfire.
Wildfire severity is measured as the number of acres burned and the percent of acres burned in the county. Main analyses are limited to Class G wildfires that burn at least five thousand acres. Sensitivity analyses examine effects of more severe wildfires that burn more than the median percent of county acres (2 percent) or at least ten thousand acres. The data do not include duration or containment date, but duration would be measured with error even with this information because wildfires can continue burning after they are fully contained (Thompson et al. 2017; Reimer, Thompson, and Povak 2019). The average wildfire duration in western U.S. forest areas is fifty-two days (Westerling 2016, 7), but average duration is likely longer for the fires in our study, because we examine the most severe Class G fire in each county and year.
We measure socioeconomic status using maternal education. NVSS birth data do not include a measure of family income. Maternal education provides a measure of socioeconomic status that strongly predicts health (Elo 2009; Harding, Morris, and Hughes 2015; Montez et al. 2019). We stratify the sample and examine birth outcomes separately by maternal education level: less than a high school degree, high school degree, some college, and at least a four-year college degree. Controls include maternal race-ethnicity (mutually exclusive categories for Black, American Indian, Asian, Latina, or White), maternal age, marital status, and whether the infant is male.
Potential mechanisms for the relationship between infant health and wildfires include prenatal care, maternal health behaviors, and air quality. We measure prenatal care using indicators for receipt of any prenatal care, receipt of care in the first trimester, and number of prenatal visits. Measures of maternal health behavior include indicators for smoking during pregnancy, number of daily cigarettes during pregnancy, and weight gain during pregnancy. These measures are not available in all years; we examine multiple measures to check for consistency across potential mechanisms and to allow for potential variation in health-care needs and behaviors. AQI is the air quality measure used by the Environmental Protection Agency and ranges from 0 to 500, with higher values indicating higher air pollution (EPA 2021). We use county-year maximum AQI, 90th percentile AQI, and the number of unhealthy days to measure exposure to poor air quality in each year for each county. These measures are logged to reduce skewness.
Analyses
We follow previous research and use an event study design to compare birth outcomes for those exposed to a wildfire during gestation with those born shortly before or conceived shortly after the wildfire in the same area (Holstius et al. 2012). We improve on existing work in three ways. First, we examine wildfires throughout the United States between 1995 and 2020 to include a more representative sample than studies that limit analysis to one location or time period. Second, we include births from the full distribution of health outcomes rather than exclude births below a certain weight or gestational length (a common limitation identified in a review by Amjad et al. 2021). Third, we examine effects on fetal death to explicitly examine selective survival. Including fetal deaths provides a more complete distribution of infant health outcomes by including pregnancies that did not result in a live birth and allows us to examine whether varying effects by maternal education reflect unequal chances of survival.
We limit analyses to counties with a wildfire because mothers and infants in those counties could differ from those in other counties on baseline health conditions and ability to respond to environmental insults. In each county-year with a wildfire, we limit analyses to births conceived twenty-one months before to twelve months after the wildfire start date. This sample includes births likely exposed during gestation (conceived approximately zero to nine months before the wildfire start date), as well as those conceived another twelve months before and twelve months after the wildfire start date. Equation 1 predicts individual infant health (i) in each birth year (t) and birth month (m), in each county of maternal residence (j), with wildfire exposure, fixed effects for birth month, year, and county, and controls (Xijtm) for individual characteristics (sex of the infant, parental marital status, maternal age and race/ethnicity, and estimated conception date). County fixed effects account for stable county differences in infant health, and month and year fixed effects address nationwide changes in infant health over time. Robust standard errors adjust for county clustering in all models.

The coefficients of interest (β1, β2, and β3) estimate the relationship between wildfire exposure and timing and the likelihood of low birth weight (LBW). We stratify the sample to fit models separately for each level of maternal education and then compare coefficients by maternal education.
Estimates rely on within-county variation in exposure across birth cohorts and within-cohort variation in exposure across counties. We fit models with and without controls and add controls for time-varying county-level characteristics (unemployment rate, poverty rate, median income) to account for local economic changes that could influence infant health.
When predicting indicators for low birth weight and fetal death, positive coefficients for wildfire exposure would be consistent with hypothesis 1, suggesting more negative health outcomes from wildfire exposure. We test for significant differences between wildfire exposure coefficients by maternal education using z tests (Clogg et al. 1995). For example, to test for different effects of first trimester exposure by education, we calculate z statistics  , where β<HS indicates the estimated effect of first trimester exposure among births to mothers with less than high school and βBA indicates the estimated effect of first trimester exposure among births to mothers with at least a bachelor’s degree. If these z statistics are positive and statistically significant, they would support hypothesis 2, that negative health effects of wildfire exposure are larger for less-educated mothers.
, where β<HS indicates the estimated effect of first trimester exposure among births to mothers with less than high school and βBA indicates the estimated effect of first trimester exposure among births to mothers with at least a bachelor’s degree. If these z statistics are positive and statistically significant, they would support hypothesis 2, that negative health effects of wildfire exposure are larger for less-educated mothers.
We repeat analyses controlling for air quality, wildfire severity (acres burned), and county economic characteristics to address potential unequal exposure and varying contexts. Because higher SES women are more likely to plan births at certain times of the year (Buckles and Hungerman 2013; Torche and Corvalan 2010), we calculate six- and twelve-month periodicity measures (following Torche and Corvalan 2010) and repeat analyses when controlling for these seasonality measures. Finally, as women with longer pregnancies have a higher chance to be exposed to wildfires (Currie and Rossin-Slater 2013), we repeat the analyses when assuming a nine-month gestation period for all births.
RESULTS
Table A.1 provides descriptive statistics for the 10 percent random sample of singleton births from 1995 to 2020. According to the CDC, rates of low birth weight and preterm birth in 2020 were 7 percent and 8 percent for singleton births (Osterman et al. 2022, 7). In our random sample including earlier years, low birth weight and preterm birth rates were comparable, at 6 percent and 10 percent, respectively. Consistent with previous studies (Rauscher 2020; Rauscher and Rangel 2020; Aizer and Currie 2014), mothers with higher levels of education give birth to healthier infants, on average. For example, rates of low birth weight are 6 percent among mothers with less than a high school degree, but 4 percent among mothers with at least a bachelor’s degree.
Table 1 presents estimates of the effects of wildfire exposure on infant health among all births in the sample, specifically, births in counties with Class G wildfires that burned at least five thousand acres, conceived twenty-one months before to twelve months after the wildfire start date. Estimates indicate that infants who are exposed to a wildfire in their second or third trimester are about 0.2 percent more likely to be low birth weight than those born to mothers in the same county but conceived earlier or later relative to the wildfire. With approximately 3.6 million births per year in the United States and about 4 percent exposed to a wildfire in their second or third trimester, this slight increase in the rate would amount to about 288 additional LBW infants. Each underweight hospital birth costs approximately $24,000 more than a normal weight birth, resulting in an estimated annual cost of nearly $7 million (America’s Health Rankings 2021).
Estimated Relationship Between Wildfire Exposure and Infant Health
Exposure in the third trimester increases the likelihood of preterm birth by 0.2 percent and fetal death by 0.04 percent. Results in table 1 are thus consistent with hypothesis 1 and suggest negative infant health effects of wildfire exposure, especially exposure late in pregnancy. These estimates hold when controlling for seasonality and air quality, suggesting that effects are not driven by air quality or selective birth timing alone. Effects on fetal death suggest selective survival could underestimate effects in naïve analyses examining only live births.
Variation by Maternal Education
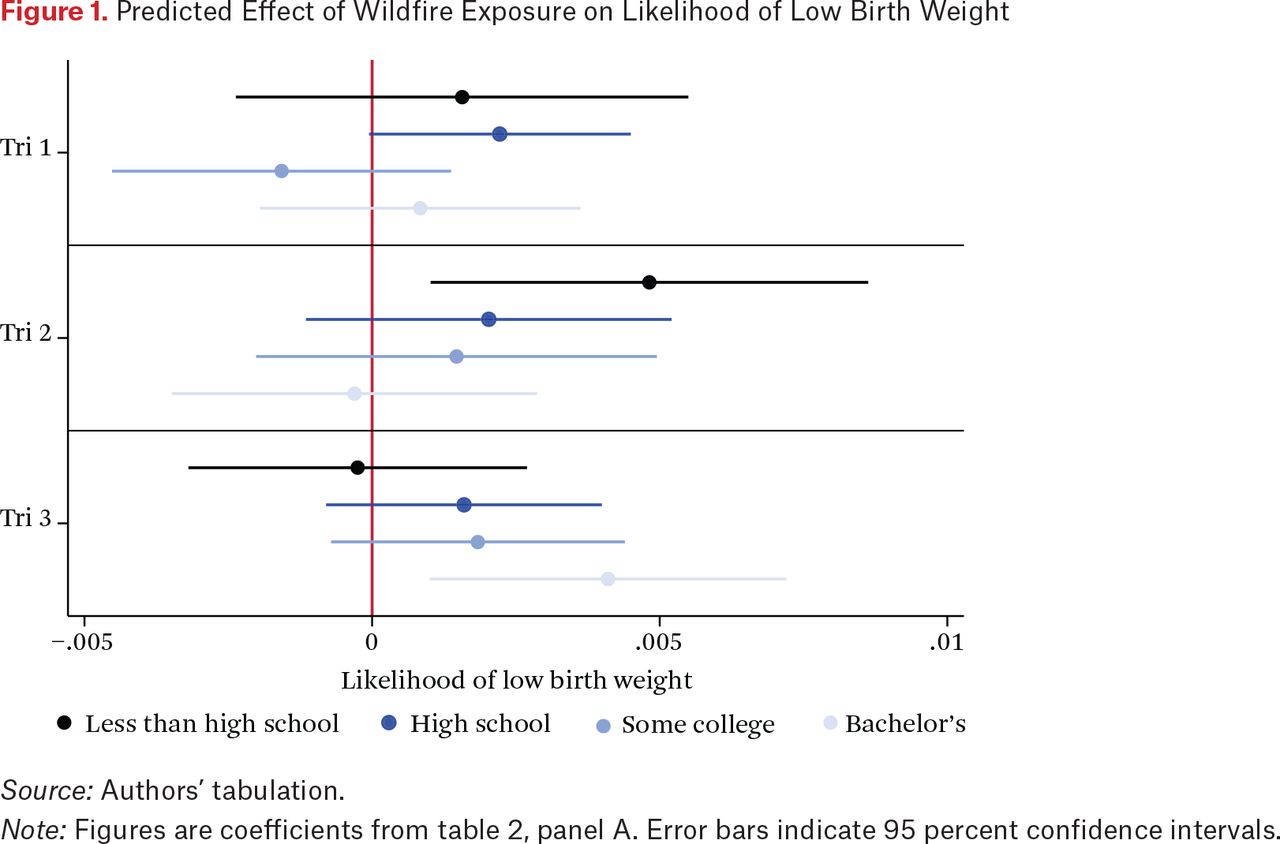
Table 2, panel A presents estimates predicting the likelihood of low birth weight separately by maternal education. Among births to mothers with less than a high school degree, wildfire exposure during the second trimester consistently increases the chances of low birth weight by about 0.5 percent. However, exposure during the third trimester has no effect for mother with less than high school. In contrast, exposure during the third trimester consistently increases the likelihood of low birth weight by 0.4 percent among mothers with a bachelor’s degree. Coefficients among mothers with less than high school and a bachelor’s degree are significantly different for both second and third trimester exposure. The unequal impact of wildfire severity on likelihood of low birth weight by maternal education is shown in figure 1. These results hold when controlling for seasonality or air quality and when including fetal deaths (pregnancies that did not result in a live birth). Estimates predicting the likelihood of preterm birth are shown in table A.5.
Relationship Between Wildfire Exposure and Infant Health by Maternal Education

Predicted Effect of Wildfire Exposure on Likelihood of Low Birth Weight
Source: Authors’ tabulation.
Note: Figures are coefficients from table 2, panel A. Error bars indicate 95 percent confidence intervals.
These estimates are small and births to mothers with less than high school account for only about 10 percent of annual births in the United States. Based on estimated effects of exposure in the first and second trimesters (0.16 percent + 0.48 percent = 0.64 percent), and average exposure in our sample (5 percent among those with less than high school in first and second trimesters), wildfires are estimated to increase the number of underweight births just to mothers with less than high school by about 117 (3,664,292 births in 2021 × 0.10 proportion less than high school × 0.05 × 0.0064 = 117). If each underweight birth costs an additional $24,000 (America’s Health Rankings 2021), even this relatively small increase would represent nearly $3 million in annual hospital costs. Births to mothers with a bachelor’s degree make up nearly a quarter of births and based on estimates of third trimester exposure (0.4 percent), wildfires are estimated to increase the number of underweight births to mothers with a bachelor’s degree by about 110 (3,664,292 births in 2021 × 0.25 proportion bachelor’s degree x 0.03 × 0.004 = 110), resulting in about $2.5 million in annual hospital costs.
Table 2, panel B presents estimates predicting the likelihood of fetal death separately by maternal education. Estimates (shown in figure 2) suggest that wildfire exposure in the third trimester increases the likelihood of fetal death by about 0.03 percent to 0.04 percent at all levels of maternal education. Exposure during the second trimester increases the likelihood of fetal death, but only among mothers with less than high school and these estimates are not significant. Estimates are consistent when controlling for seasonality and air quality.

Predicted Effect of Wildfire Exposure on Likelihood of Fetal Death
Source: Authors’ tabulation.
Note: Figures show coefficients from table 2, panel B. Error bars indicate 95 percent confidence intervals.
Longer pregnancies have a higher chance wildfire exposure (Currie and Rossin-Slater 2013), so analyses assuming nine-month gestation for all births are analytically valuable when predicting fetal death. When assuming nine-month gestation, second trimester wildfire exposure increases the likelihood of fetal death significantly more among mothers with less than high school than those with a high school degree.
Overall, results examining variation in effects of wildfire exposure are generally consistent with hypothesis 2 for second trimester exposure and suggest wildfires reduce infant health more among mothers with low levels of education. However, third trimester exposure has more negative infant health effects among mothers with higher levels of education. Varying effects of wildfire exposure by timing and maternal education are consistent with the selective survival explanation for unequal effects of environmental insults by SES.
Sensitivity Analyses
Results are consistent when conducting multiple sensitivity analyses. We repeat analyses with and without controlling for time-varying county characteristics (unemployment rate, poverty rate, median income) and with and without including controls for parental characteristics (maternal race, age, marital status). We repeat analyses when excluding births in counties with only one wildfire and results are consistent. Results are also consistent when limiting analyses to counties with a severe wildfire (above the median percent of county acres burned). Estimates controlling for seasonality measures and when assuming a nine-month gestation period for all births yield consistent results.
We include the full range of infant health outcomes to avoid selective exclusion concerns in existing research identified by Sana Amjad and her colleagues (2021). However, because some states do not report fetal death data for births below 350 grams or twenty weeks of gestation, we repeat analyses excluding births below these values and find consistent results.
After a wildfire, the same forest can burn again even in the following year, depending on climate conditions and plant adaptation to fires (Harvey, Donato, and Turner 2016; Coop et al. 2020). However, wildfires in an area that recently burned may be less severe or disruptive. To account for repeat fires in the same area, we conduct two additional sets of analyses examining only the largest wildfire in each county within three years or within five years. Results in some models are smaller but in the same direction when examining births around these more severe wildfires. We also estimate the relationship between wildfire exposure and infant health when including all counties, even those without a wildfire, and find consistent results.
Mediation Analyses
Heterogeneous effects of wildfires by maternal education raise questions about mechanisms that could explain the varying results. Table 3, panel A presents the coefficients from models predicting the effect of wildfire exposure on multiple potential mechanisms. Estimates suggest that wildfires increase tobacco use and reduce prenatal care and weight gain among mothers at each level of education. For example, estimates predicting receipt of any prenatal care suggest that women are about 9 to 12 percent less likely to receive prenatal care when exposed to a wildfire. Similar estimates by SES are not consistent with unequal parental response to wildfire exposure. Based on measures of prenatal care, tobacco use, and weight gain, maternal response to wildfire exposure is similar by maternal education.
Mediation Analyses
Table 3, panel B presents estimates of the percentage of the total effect of wildfire exposure on low birth weight that is mediated by the potential mechanisms examined, using medeff in Stata (Hicks and Tingley 2011). Estimates are shown separately by maternal education as an exploratory step to understand varying effects of wildfires. The largest mediation estimates are for the number of prenatal visits and tobacco use, and variation offers suggestive evidence that their mediating role differed by maternal education. Specifically, estimates suggest wildfire exposure in the second and third trimesters may have reduced infant health among less-educated mothers in part by reducing prenatal visits and increasing tobacco use. In contrast, these maternal behaviors mediated smaller fractions of the effect of wildfire exposure for more-educated mothers.
Mediation estimates suggest county air quality may also mediate a small part of the effect of prenatal wildfire exposure on infant health. Air quality is measured using the annual county maximum AQI score, which is not ideal because it does not vary by individual birth within each county-year. Using county-year measures, mediation estimates suggest air quality could explain up to 2 percent of the effects of wildfire exposure on infant health.
At the same time, our mediation estimates suggest that wildfires affect infant health through mechanisms other than air quality. Wildfires are disruptive events, influencing multiple aspects of life, including transportation to work and prenatal care, destruction of capital, and stress (Wang et al. 2021; Davis et al. 2014; Kuligowski 2017). Individual-level air quality measures could yield higher mediation estimates, but relatively large estimates for prenatal visits, tobacco use, and weight gain suggest that other mechanisms are involved. For example, wildfires may influence infant health by disrupting transportation to prenatal care, destroying family homes, and increasing stress (Wang et al. 2021; Davis et al. 2014; Kuligowski 2017).
These mediation estimates should be interpreted with caution because they rely on the strong assumption of sequential ignorability (Imai et al. 2011), which is often violated. Table 3, panel C shows the correlation between error terms from the models predicting each mediator and the outcome measure required to make each mediation estimate zero. Mediation estimates are predicted to become zero at relatively low levels of correlation between error terms in models predicting the outcome and the mediator, suggesting estimates are sensitive to potential violation of the sequential ignorability assumption. Mediation estimates for prenatal visits and daily cigarettes are the least sensitive to potential violation, consistent with the evidence that prenatal care and tobacco use are key mechanisms for the relationship between wildfire exposure and infant health.
CONCLUSION
Based on more than 1.3 million birth records between 1995 and 2020, estimates suggest that exposure to a wildfire in the county where the mother resides during pregnancy reduces infant health. The relationship between wildfire exposure and infant health, however, varies by maternal education and by the timing of exposure. Wildfire exposure during the second trimester reduces infant health more among mothers with low levels of education, but exposure during the third trimester reduces infant health more among mothers with at least a bachelor’s degree. For example, among births exposed during the second trimester, wildfire exposure increased the likelihood of low birth weight by 0.5 percent for mothers with less than high school, but had no effect on those with a bachelor’s degree. In contrast, among births exposed during the third trimester, wildfire exposure increased the likelihood of low birth weight by 0.4 percent for mothers with a bachelor’s degree, but had no effect for mothers with less than high school. These results hold in multiple sensitivity analyses.
The effects of wildfire exposure on infant health are small. However, even small effects on the likelihood of low birth weight have substantial long-term consequences for life chances, resulting in higher risk of disability, mortality, and poor health later in life, as well as lower educational and labor-market outcomes (de Jong et al. 2012; Swamy, Ostbye, and Skjaerven 2008; Aizer et al. 2018; Bellinger et al. 1991; Mazumdar et al. 2011; Baranowska-Rataj et al. 2022). In addition, even small effects on infant health are costly for society. Wildfire exposure is estimated to increase the number of underweight births by about 288 births per year, amounting to nearly $7 million in added annual hospital costs. As wildfire frequency and severity increase (Dennison et al. 2014; Halofsky, Peterson, and Harvey 2020), these estimates suggest the importance of mitigating their effects.
In a novel step, we examine fetal death data to understand variation by maternal education and to explicitly examine selective survival. We find that wildfire exposure slightly increases the likelihood of fetal death, particularly in the third trimester. In some models, second trimester wildfire exposure increases the likelihood of fetal death significantly more among mothers with less than high school than among those with a high school degree. The variation in likelihood of fetal death is consistent with selective survival and suggests that wildfire exposure earlier in pregnancy reduces the chances of fetal survival more among mothers with fewer resources. By the third trimester, fetuses carried by less-educated mothers are more highly selected and less sensitive to further environmental insults. In contrast, fetuses carried by more-educated mothers are more likely to survive wildfire exposure earlier in pregnancy, suggesting they are less selected and may be more sensitive to later environmental insults.
In addition to selective survival, mediation analyses suggest the variation by maternal education could partly reflect varying importance of prenatal care and tobacco use. Wildfire exposure reduces prenatal care and increases tobacco use at all levels of maternal education. But those maternal behaviors explain a higher fraction of the relationship between wildfire exposure and infant health outcomes for mothers with less than high school than those with a bachelor’s degree. These results are not consistent with unequal parental response and are consistent with differential sensitivity to wildfires. Despite similar exposure and similar changes in prenatal care and tobacco use, wildfire exposure can still have more negative effects on low-SES infants due to higher baseline risk factors, such as exposure to chronic stress, that can increase the likelihood of negative health outcomes from additional stress or poor air quality during a wildfire (Torche 2018; Martins et al. 2004).
Mediation analyses suggest prenatal care, tobacco use, and weight gain account for a larger fraction of the relationship between wildfire exposure and infant health than county air quality. Mediation analyses are sensitive to potential violation of the sequential ignorability assumption, but estimates predicting infant health are also similar with or without controlling for county air quality. Taken together, these findings suggest that wildfires may harm infant health more through stress and maternal behaviors than air quality. Stress could help explain the negative health implications for mothers with both low and high education levels, consistent with evidence of the substantial economic and disruptive effects of wildfires (Wang et al. 2021; Currie and Rossin-Slater 2013). The NVSS birth data do not include economic or stress measures and the fetal death data do not include all pregnancies that do not result in a live birth. Future research examining those measures or more complete pregnancy data would provide additional evidence about mechanisms and help explain variation by maternal education.
Overall, results provide additional evidence of the negative effects of wildfires when including a more complete sample of births and when explicitly examining selective survival. Detrimental effects of wildfires on infant health indicate their long-term implications for health and well-being in the next generation. Poor infant health has economic and health costs for individuals and society (de Jong et al. 2012; Swamy, Ostbye, and Skjaerven 2008; Aizer et al. 2018; Bellinger et al. 1991; Mazumdar et al. 2011; America’s Health Rankings 2021) and growing wildfire exposure is likely to increase those costs. Furthermore, our results suggest that the negative health implications of wildfires are stronger among infants born to mothers with low levels of education, increasing the likelihood of fetal death and low birth weight early in pregnancy. Mediation analyses suggest the variation by maternal education reflects selective survival and unequal sensitivity, rather than differential parental response to wildfires. In addition to reducing wildfire exposure, mitigation and response efforts should work to reduce the burdens wildfires pose for pregnant women with low levels of education.
FOOTNOTES
↵1. Online appendix material can be found at https://www.rsfjournal.org/content/10/1/255/tab-supplemental.
- © 2024 Russell Sage Foundation. Rauscher, Emily, and Xinyan Cao. 2024. “Unequal Effects of Wildfire Exposure on Infant Health by Maternal Education, 1995–2020.” RSF: The Russell Sage Foundation Journal of the Social Sciences 10(1): 255–74. DOI: 10.7758/RSF.2024.10.1.11. The authors are grateful for feedback from colleagues at the Russell Sage Foundation, reviewers, and journal editors. This research was supported by the Population Studies and Training Center at Brown University, which receives funding from the NIH (P2C HD041020). Direct correspondence to: Emily Rauscher, at emily_rauscher{at}brown.edu, Brown University Box 1916, Providence, RI 02912, United States.
Open Access Policy: RSF: The Russell Sage Foundation Journal of the Social Sciences is an open access journal. This article is published under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.
REFERENCES
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.