
Abstract
Public cooperation with health experts and authorities plays a critical role in curbing the spread of disease during outbreaks such as the COVID-19 pandemic. Through data collected using mixed methods in May and June of 2020, we investigate the influence of information from horizontal and vertical ties on the likelihood that individuals would practice safe and healthy behavior. We look at actions such as staying home, wearing personal protective equipment, and increased handwashing in two northeastern U.S. metro areas. Controlling for factors thought critical in previous studies, our analysis of more than eight hundred survey responses and more than sixty interviews finds that reliance on information from horizontal and vertical ties correlates significantly with behaviors designed to curb the spread of the virus.
At the start of the novel coronavirus pandemic in February and March 2020, individuals in the United States and elsewhere were inundated with public information about the disease now known as COVID-19. A variety of government, media, and civil society sources pushed actions to curb the spread of the virus and “flatten the curve.” Advice included avoiding contact with sick people, staying home when ill, cleaning and disinfecting frequently touched objects and surfaces, and by April, wearing a face mask and maintaining a distance of six feet from others. Staying home and mask-wearing in public play important roles in curbing the virus’s spread (CDC 2020a, 2020b; Soltesz et al. 2020; Trauer et al. 2021). Health communication was critical in this effort, yet when the Centers for Disease Control and Prevention (CDC) began recommending near-universal mask-wearing in public, there was little precedent for understanding how Americans would respond to large-scale health communication efforts (Fisher et al. 2020), especially among less vulnerable groups.
In this study, we examine the effects of information and social ties on healthy behaviors among individuals with high human capital in the early months of the COVID-19 pandemic. Although our sample is not a nationally representative one, its demographic characteristic match 235 counties in the United States where more than seventy-four million North Americans live and that host many of the largest land-grant universities. An original survey having been administered in May and June of 2020 in neighborhoods in Boston and New York City,1 our team collected data on changes in behavior at the individual level along with the information sources these 822 individuals relied on during the first wave of the virus. We also carried out more than sixty face-to-face interviews and doublechecked our results with a nationally representative sample of 5,275 respondents from the U.S. Census Pulse survey (2022).
Controlling for a variety of factors, including age, income, education, gender, political partisanship, employment status, and marital status, we find evidence that contact with and reliance on information from horizontal and vertical ties had a measurable effect on behaviors during the pandemic. Horizontal ties are high trust, frequently contacted connections between friends, extended kin, and family, and also connections with people from different backgrounds through institutions, including workplaces, faith-based organizations, and horizontal associations. Vertical ties involve “respectful and trusting ties to representatives of formal institutions,” which may involve only occasional, single-direction communication (Szreter and Woolcock 2004, 665). In this study, respondents routinely cited reliance on their close networks for information and support while looking to authorities—including mayors, governors, and Dr. Anthony Fauci—for guidance on health practices. Relying on information from vertical and horizontal ties strongly correlated with altered behaviors relating to the adoption of nonpharmaceutical interventions (NPIs), such as wearing personal protective equipment (such as masks and gloves), avoiding public spaces, and handwashing.
This article advances the field in several ways. First, although many studies have sought to understand protective behaviors during the pandemic, they have relied on single types of data, whether qualitative or quantitative (Liu and Mesch 2020; Ozdemir et al. 2022). To move beyond the challenges of any one methodological framework, we use mixed methods to gather both interview and survey data, using large- and small-N samples (Lieberman 2005; King, Keohane, and Verba 1994).
Next, although studies of crises and health communication often focus on vulnerable populations such as the elderly, minority communities, and the disabled (see Vinck et al. 2019), scholars understand less about how higher-income, highly educated Americans respond to such efforts. Such individuals are highly prized by political campaigns (Kurtlzeben 2018), often holding leadership positions in civic and political groups (Askarinam and Hounshell 2022). Further, although individuals in our sample live in two large metro areas in the United States (New York and Boston), they closely mirror the demographics of the 235 U.S. counties that are home to more than 22 percent of the country. Our work complements other ongoing COVID-19 research examining smaller subsets of the overall U.S. population to paint a fuller picture of the outcomes (Burns and Albrecht 2022, this issue; Evans et al. 2022, this issue; Pezzia, Rogg, and Leonard 2022, this issue).
The results of our analysis bring important implications for the study of information and social ties. Horizontal and vertical ties were critical sources of information and behavioral change in the early months of the pandemic. In an era of misinformation (Galvão 2021) and deliberate disinformation, generalized communication strategies are unlikely to have broad impact. More broadly, this work contributes to a long-standing need to better integrate social science perspectives with public health research, underscored by the COVID-19 pandemic (see, for example, Kleinman 2010; Davies and Wenham 2020). When asked about misinformation during the pandemic in a December 2021 interview, former National Institute of Health (NIH) Director Francis Collins lamented, “I wish I had more insights from behavioral social science research on how this has come to pass” (Subbaraman 2021). This research contributes to understanding how Americans receive and act on information presented as part of health education campaigns, adding critical context to an area of work predominantly focused (with good reason) on low- and middle-income countries and vulnerable groups (see Howard et al. 2017; Vinck et al. 2019).
HOW NETWORKS INFLUENCE BEHAVIOR
Much research has underscored that networks influence our behavior: the choices and encouragement of people with whom we interact encourage us to alter our behavior in a process known as social contagion. A field experiment in Minneapolis and Denver showed that voters transmitted their motivation to vote from household member to household member (Nickerson 2008). Contact with advertisements and messages on social media platforms such as Facebook can influence network members to take on more activist behaviors (Kwon, Stefanone, and Barnett 2014). So too health-related behavior can be altered by network members talking about and encouraging activities such as quitting smoking or exercising (Latkin and Knowlton 2015).
These networks can include a pair of actors, or dyads, where information is directed from one actor, the source, to another, the target, but is not necessarily reciprocated (Yang, Keller, and Zheng 2017). Elements of these social networks, such as the information, influence, social credentials, or reinforcement provide individuals with resources that can be mobilized for action or gain (Coleman 1988; Lin 2001), which Nan Lin defines as social capital, or “the resources embedded in social networks accessed and used by actors for actions” (2001, 25). These networks can remain open and dispersed, allowing for bridges and weak ties to emerge and still facilitate information or influence, or dense and closed, giving greater leverage to realize the gains of social capital (Granovetter 1973; Lin 2001).
Research on social capital categorizes social ties into horizontal and vertical ones (Woolcock 2002); these function in different ways and lead to varied outcomes during shocks and crises. Close horizontal ties can facilitate physical, emotional, and financial support during an event (Hurlbert, Haines, and Beggs 2000). Tightly knit horizontal ties often between friends or family, for example, help would-be evacuees and affected individuals make critical, often life-saving choices about departure and return. A study of more than 1.5 million social media users before and during Hurricanes Harvey, Irma, and Maria demonstrated that broader and more diverse networks motivated people to evacuate from low-lying areas (Metaxa-Kakavouli, Maas, and Aldrich 2018). Communities with stronger horizontal social ties bring back more evacuees after shocks as well (Aldrich 2012).
Beyond horizontal ties, vertical ties to decision-makers also matter in shocks. Although more than fifty coastal towns and villages were devastated by Japan’s tsunami of March 2011, only one community—a city with a connection to well-resourced decision-makers in Tokyo—received central government funds for expensive reconstruction projects (Aldrich 2019). One-way vertical ties (individual trust in government officials), have also been shown to matter in disasters; in the 2014 Ebola outbreak in West Africa, for example, individuals expressing distrust in local officials were less likely to adopt preventive behaviors (Vinck et al. 2019). How these horizontal and vertical ties influenced health behaviors early in the pandemic remains an open question.
METHODS AND DATA
This study undertakes both quantitative and qualitative analyses to understand the associations between reliance on information from horizontal and vertical ties and behavioral change during the COVID-19 pandemic. We draw on an original dataset (N = 822) from a survey (Aldrich et al. 2020) conducted in May and June of 2020 in the Boston and New York City metro areas, including zip codes 02127, 02132, 02135, 10304, 10301, 11223, 11224. We recruited individuals by mail and social media, purchasing contact information from Valassis. Participants recruited by mail received a personalized letter of invitation with a paper survey and a prepaid return envelope. Those recruited by social media were recruited on Facebook with Facebook ads in our select zip codes and were invited to complete a survey identical to the paper survey via the Qualtrics survey platform.
Quantitative surveys captured respondents across a broad range of demographic characteristics—gender, age, income, education, and social capital—but the average respondent was a White, highly educated woman. Table 1 displays the demographic distribution of our sample. These findings are consistent with what we know of social science survey participants, especially in web-based surveys. Previous work on the racial, gender, and socioeconomic characteristics participation rates have found that non-Hispanic Whites and Asians are more likely than Black participants to participate in surveys, higher levels of education are associated with survey completion (Jang and Vorderstrasse 2019; Reinikainen et al. 2018), and women are more likely than men to participate in self-administered surveys (Mulder and de Bruijne 2019).
Descriptive Statistics of the Control Variables for the Large-N, Quantitative Analysis
Social scientists typically seek to capture large, representative samples and use statistical techniques such as weighting to reproportion their sample to look like the broader population should they fail (D’Exelle 2014). Yet epidemiologists and social scientists alike acknowledge the value of nonrepresentativeness in causal investigation (Rothman, Gallacher, and Hatch 2013). We build on the work of other articles in this issue that have looked at specific demographic groups such as vulnerable older adults (Pezzia and Leonard 2022, this issue), Native Americans (Evans et al. 2022, this issue), and residents of small towns (Burns and Albrecht 2022, this issue). We apply post-stratification weights only to gender, leaving our nationally nonrepresentative sample to match 235 counties in the United States with similar attributes, home to more than seventy-four million Americans. To calculate our matching counties, we selected U.S. counties that exceed the 2021 Census Bureau national averages of median household income ( > $64,994), percentage White alone, not Hispanic or Latino ( > 60.1 percent), and percentage bachelor’s degree or higher ( > 32.9 percent). The 235 counties matching these demographics include a number of large metro areas (for a complete list and map of matching counties, see figure A.1 and table A.4 in the online appendix at https://www.rsfjournal.org/content/8/8/32/tab-supplemental). We confine our conclusions about behaviors to individuals with higher levels of human capital and to residents in urban and suburban communities whose votes are coveted and whose behaviors are scrutinized during elections (Kurtzleben 2018). Finally, we used a nationally representative dataset of 5,275 respondents from the 2022 U.S. Census Pulse surveys to double-check our results.
We carried out follow-up semi-structured interviews with a subset of survey participants in June and July 2020 (n = 62) to add depth and causal process to our quantitative results. Interview participants were recruited via positive responses to a survey question about their willingness to participate in a follow-up interview. All interviews were conducted via Zoom by a team of two researchers, using an instrument designed to further probe responses to each segment of the survey instrument. Interviews were transcribed by Amazon Web Services’ Transcribe service for analysis. Table 2 displays the demographic distribution of our interviewees.
Descriptive Statistics of Small-N, Qualitative Analysis
We analyzed the data from our qualitative interviews with a reflexive thematic analysis (Richards 2021), which includes the following five steps: collect the data, code the data, categorize the data, create themes, and interpret themes. We trained a team of three graduate students to code text segments in interview transcriptions that demonstrated both reliance on information from social ties and the subsequent behavioral change. With each segment, the graduate students coded the presence of reliance on information from social ties and the subsequent behavior change. We then categorized the data into the nature of the source of information. We then created themes generated deductively from the social capital literature, which signify horizontal and vertical ties.
Our study includes three dependent variables: avoidance of public spaces to minimize viral transmission, use of personal protective equipment, and increased frequency of handwashing (see table 3). These three behaviors were routinely promoted as effective and protective behaviors to curb the spread of COVID-19 throughout the pandemic. Individuals were asked, “Please indicate any changes in your behavior due to COVID-19 or related stay in place orders.” Responses to “Avoided going to public places,” “Started using personal protective equipment (such as masks and gloves),” and “Increased frequency of handwashing” were coded 1 if the individual reported the behavior and 0 if the individual did not (see table 3).
Descriptive Statistics of Dependent Variables for the Large-N Quantitative Analysis
Emergent themes we observed from the interviews, such as that with Gabrielle, demonstrate respondents came to trust authorities even if their only connections came from one-way, media interactions: “Such as Dr Anthony Fauci, I learned the science behind the pandemic. I learned, um, I watched as the science evolved and we became more aware of what it was and what it meant.”
Meghan similarly talked about building trust through broadcasts from an elected figure: “And I would add that the other place I did go for information was Governor Cuomo. So I would listen to his daily conferences. . . . Well this is gonna sound really hokey but I felt like he was being honest because he was saying how bad it was.”
Further, when asked about vertical ties to local elected officials, informants responded as follows:
Yeah, so I probably once a week watch Mayor Walsh’s or Charlie Baker’s press conferences to the Boston.com link to get direct information from them. . . . Um, yeah, I think, and also just trying to make good decisions from my family about you know, what’s safe, what kind but parts of the reopening do I want to participate in what don’t I want to do? And so on. (Beth)
Yeah. So it was daily briefings with Cuomo. It was like the highlight of my day. I just felt they were very realistic and factual based. So I appreciated that without all the speculation and rhetoric from other sources. . . . His daily updates were informative. They were fact based and they were science based, so I appreciated that. The CDC and WHO I Googled and went on the CDC website a lot, especially concerning the baby and using masks and, you know, just general information like that. And then, um I know me and my friends were talking once a day and they said something that says what’s good. . . . Well, we stay in the house a lot. Um, wearing a mask—I’ve become much more conscious of washing my hands than I had been previously. I washed them, but not like I do now. Um, I carry hand sanitizer. Now, any time I go anywhere, I come from there, I put it on my hands before I get in my car. (Gigi)
These vertical ties match the definition of linking social capital, which involves “respectful and trusting ties to representatives of formal institutions” (Szreter and Woolcock 2004, 665). These connections capture aspects of political participation, including political efficacy and political trust (Poortinga 2012, 288).
Horizontal ties capture the high trust, frequently contacted connections involving friends, extended kin, and family (Adler and Kwon 2002). This form of social capital often results in homophily—high levels of demographic, attitudinal, racial, and linguistic similarity—in these networks (Mouw 2006). These thick connections inform life-saving decisions when neighbors knock on doors before a fire spreads out of control or rescue family and friends nearby who are trapped beneath the rubble of collapsed homes (Aldrich 2012). In our interviews, when asked to explain the information they relied on to get through the coronavirus outbreak, individuals routinely cited the importance of these ties: “Originally in the beginning, I was looking at all the news and it just got very overwhelming. And there were a lot of sources that didn’t feel very reliable. So eventually I just started asking my closest friends who were really following experts to sort of guide me on like, Okay, what are the new policy things? What are the changes? How much worse has it gotten? Because I just couldn’t take it. And I knew that my friends were really looking at reliable news sources. (Christina)”
Horizontal ties also include ties that connect people from different backgrounds through institutions, including workplaces, faith-based organizations, and horizontal associations. Early research on “thin” or “weak” ties indicated their tremendous power in helping young job searchers find work through their extended networks (Granovetter 1973). Even a small, neighborhood-based childcare center can provide users and their families with critical information and assistance (Small 2009). For example, in our interviews, individuals cited the importance of these ties to practicing their faith in the pandemic:
One thing I would say is that our rabbi was very strict about everything, and it made us feel very supported as, like the community that, like he took [COVID] seriously and also meant that like when he decided to start doing services again. So he made it very safe so that I felt comfortable that my husband could go back to a synagogue and pray there like, for example, like he had it outdoors. And everyone has to stand six feet apart. And everyone has to wear a mask and, you know, like otherwise like, I feel like he couldn’t have gone back in the community if he hadn’t taken it seriously. (Candice)
To understand the associations between reliance on information from horizontal and vertical ties and the practice of prescribed safe and healthy behavior during the pandemic, we used an iterated principal factor analysis to categorize the sources of information individuals relied upon based on the themes from interviews we conducted and on survey responses to the following question: “Which of the following sources have you relied on for information during the COVID-19 outbreak?” (for the full qualitative script and quantitative survey questions, see the online appendix).
The variables in our factor analysis loaded on two key factors: reliance on information from horizontal and reliance on information from vertical ties (see table 4). Information received and relied on from friends, neighbors, family, coworkers or colleagues, and community organizations and groups (such as church, temple, mosque, neighborhood groups) were categorized as reliance on information from horizontal ties.
Results from a Factor Analysis of Sources of Information Relied on During COVID-19
Information from local elected officials, local government agencies, state elected officials, state agencies, federal government leaders, CDC, NIH, and the World Health Organization (WHO) were categorized as vertical ties, consisting of trust in or relationships between people separated by levels of power and authority (Szreter and Woolcock 2004). These ties provide information and resources that are often unavailable locally. In our interviews, individuals routinely cited reliance on the CDC, the NIH, Governors Baker and Cuomo, and Fauci:
Well, they’re trusted institutions, they’re institutions that I associate strongly with making decisions and issuing information based on science, not based on politics or the political moment that they would actually assess the risks and tell us. . . . There [was] a lot of uncertainty early on . . . the role of masks and how important masks were. So I relied heavily on those institutions to evaluate the science. . . . I trusted the CDC and NIH to actually evaluate [all of the claims made by researchers] publishing in not yet peer-reviewed pieces and tell us what we actually should and should not take away from them. (Christopher)
The CDC and the NIH I think provided many guidelines for what you should be doing? Whether it’s wearing mask or social distancing or, you know, touching surfaces or how to clean things on. I relied on them personally, but also for my job [with] Zipcar. . . . relied on a lot of both local and federal and state regulations to figure out how we could safely . . . support our employees and our members. (Emmie)
Work on vaccine hesitancy (Khubchandani et al. 2021) and responses to health recommendations during COVID-19 (Grossman et al. 2020) identifies factors correlated with accepting and acting on new information. Building on this literature, we controlled for demographic characteristics (see table 2), including age (O’Malley, Kerner, and Johnson 1999), income (O’Malley, Kerner, and Johnson 1999), education (Khubchandani et al. 2021), gender (Burke 2001; Carpenter et al. 2011; O’Malley, Kerner, and Johnson 1999), and political party affiliation (Malka, Krosnick, and Langer 2009; Grossman et al. 2020; Khubchandani et al. 2021; Barrios and Hochberg 2020; Gadarian, Goodman, and Pepinsky 2021; Allcott et al. 2020; Clinton et al. 2021).
ANALYTICAL STRATEGY
For our quantitative analysis, we use logistic regression models to test the reliance individuals had on vertical and horizontal ties and our three dichotomous dependent variables: avoidance of public spaces, use of personal protective equipment, and increased frequency of handwashing. We structure additional regression models, including ordinary least squares, Poisson, and negative binomial regression models to ensure the results we uncovered in our logistic regression were not artifacts of model choice. All three of the models have heteroskedasticity–robust standard errors, and multicollinearity tests indicated low levels of collinearity between the variables in our models. The variance inflation factor for the models was less than 3.79, which is well below the accepted threshold (Salmerón Gómez et al. 2016). Further, to correct for oversampling of women in our study, we applied a post-stratification weight to our models based on the gender distribution reported by the Census Bureau.
RESULTS
The results of our statistical analyses are organized by three behaviors designed to curb the spread of the virus promoted by the CDC: avoiding public places, using personal protective equipment, and practicing frequent handwashing.
Staying Home and Avoiding Public Places
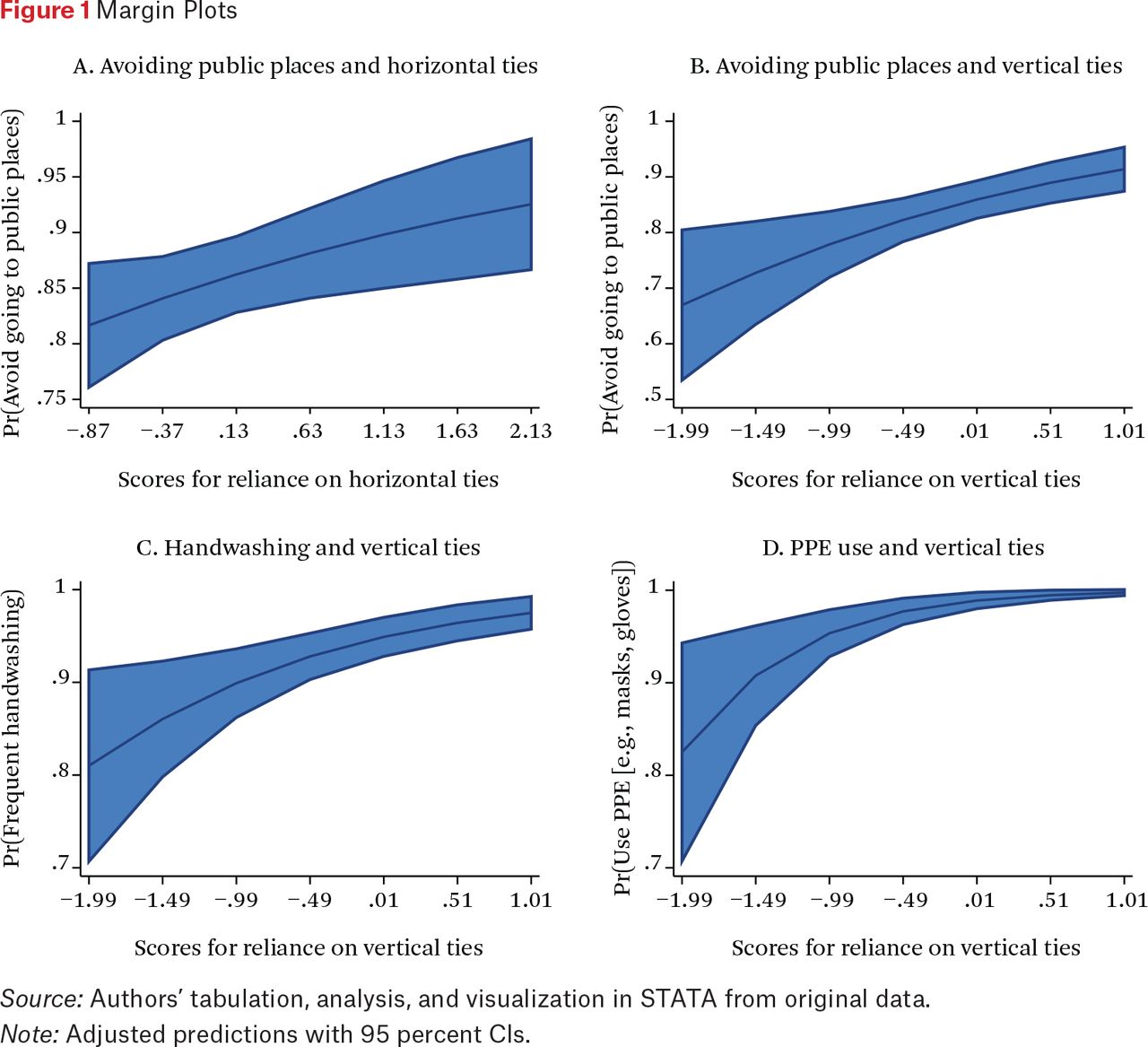
In our first model (table A.1), our results indicate that individuals in our study who relied on information from their horizontal and vertical ties were more likely to indicate avoiding public places in May and June of 2020. A one-unit increase in reliance on information from horizontal ties results in a 1.407 (p < .05) increase in the odds of an individual avoiding public places. A one-unit increase in reliance on information from vertical ties results in a 1.736 (p < .01) increase in the odds of an individual avoiding public places. Further, holding all other variables at their mean, post-estimation predictive margins reveal that (figure 1a, figure 1b) the probability of avoiding going to public places goes from 82 percent to 93 percent from the lowest to highest measures of relying upon horizontal ties, and from 67 percent to 91 percent from the lowest to highest measures of relying on vertical ties. Gender, race, and employment status were also significant variables in this model. Women were more likely than men in the reference group to report avoiding public places (1.671, p < .1). Non-White individuals were less likely than White individuals in the reference group to report avoiding public places (–0.565, p < .1). Further, individuals unable to work were more likely than individuals employed full time in the reference group to indicate avoiding public places (9.443, p < .01).

Margin Plots
Source: Authors’ tabulation, analysis, and visualization in STATA from original data.
Note: Adjusted predictions with 95 percent Cls.
Using Personal Protective Equipment
In our third and final model (table A.3), our results indicate that individuals in our study who relied on information from vertical ties were more likely to report increased handwashing in May and June of 2020. A one-unit increase in relying on vertical ties resulted in a 2.089 (p < .05) increase in the odds of an individual increasing the frequency of handwashing. Holding all other variables at their mean, predictive margins indicate (figure 1d) that the probability of increased handwashing went from 81 percent to 97 percent from the highest and lowest measures of relying on vertical ties. Age, income, education, and marital status were also predictors of handwashing. Those who were seventy-five years old and older (21.53, p < .05), reported incomes of between $60,001 and $80,000 (3.207, p < .1) and between $100,001 and $120,000 (13.17, p < .01), and had some college, no degree (4.633, p < .1) were more likely than those in their respective reference groups to report handwashing. Widowed individuals (0.0715, p < .05) were less likely than those who were single or never married to report increased handwashing.
Increased Handwashing
In our second model (table A.2), our results indicate that individuals in our study who relied on information from vertical ties were more likely to report the use of personal protective equipment (PPE), such as masks or gloves, in May and June of 2020. A one-unit increase in reliance on vertical ties results in a 4.352 (p < .01) increase in the odds of an individual using PPE. Holding all other variables at their mean, predictive margins indicate (figure 1c) that the probability of wearing a mask, for example, went from 83 percent to 99.7 percent from the highest and lowest measures of reliance on vertical ties. Other factors, including income, education, employment status, and marital status were statistically significant predictors of PPE use. Those who reported an income of between $40,001 and $60,000 (7.827, p < .01), between $60,001 and $80,000 (5.094, p < .05), between $100,001 and $120,000 (25.65, p < .05), and more than $120,001 (8.024, p < .01) were more likely to report using PPE relative to those who reported an income of less than $40,000. Those who were retired or not looking for work (–0.223, p < .1) were less likely to report using PPE relative to those employed full time in the reference group. Further, those who were married (–0.435, p < .1) were less likely to report using PPE relative to those who were single or never married in the reference group.
DISCUSSION
Much has been made of the role of political party identification in determining behavior during the COVID-19 pandemic (Grossman et al. 2020; Khubchandani et al. 2021; Barrios and Hochberg 2020; Gadarian, Goodman, and Pepinsky 2021; Allcott et al. 2020; Clinton et al. 2021). For example, newspaper articles and blogs alike have emphasized that Republicans seem less likely to take on mask-wearing or engage in physical distancing and the other preventive measures endorsed by health agencies. However, in our models consisting of primarily Independents and Democrats to accurately characterize the partisanship of the geographies we sampled, we did not find party affiliation to be a significant predictor. Instead, our research pushes us to look beyond simple party affiliation to the role of social networks—horizontal and vertical ties—that influenced healthy and safe behavior during the COVID-19 pandemic.
Our findings indicate vertical ties with entities of power, or the reliance individuals had on mayors, governors, and government leaders such as Dr. Fauci, was a statistically significant variable in all three of our models. These findings confirm that the information from these sources of power and prestige was associated with a higher probability that survey participants would report staying home during the pandemic, using PPE, and increasing the frequency of handwashing. In the case of PPE use, vertical ties were associated with the near-universal use of facemasks or gloves during the early months of the pandemic. In terms of staying home, horizontal ties were also important.
Our qualitative findings (discussed in the following section) from sixty-two one-on-one interviews suggest that reliance on horizontal ties, in particular, played a role, for example, in getting to and from work in a way that avoided the public. In our follow-up interviews of survey participants, individuals further confirm these findings. Direct quotes are reported in the participants’ own language; respondent names have been changed to pseudonyms to protect their identity.
Staying Home and Avoiding Public Places
Many interview participants noted the importance of drawing on close horizontal ties not just for information but also for assistance in staying home in the early months of the pandemic. This resonates with findings from previous disasters, finding that individuals make important decisions about whether to stay home or evacuate during crises, and if they evacuate, whether to return (Aldrich 2012; Metaxa-Kakavouli, Maas, and Aldrich 2018), as well as previous findings on adherence to physical distancing during COVID-19 (Petherick et al. 2021). Similarly, our interviews show how individuals relied on horizontal ties to grapple with more quotidian questions—such as whether to avoid non-essential errands or take public transportation to work.
Now, my thing was with my family, I work outside. So they were always telling me [to] make sure I stay away from people. Um, if somebody approaches me, make sure I had my mask on that my sister made for me. (Katy)
The majority of people in my neighborhood . . . followed the rules. Everyone in my building was all of a sudden working from home, everyone wearing a mask when they go outside. My neighborhood, my community, groups that I’m part of totally flipped from in-person engagement to online, and so totally changing how we socialize and meet and work. . . . And so we’ve created new programs that do that, to engage people from home. (Abbie)
My roommate is back to work. He works in construction. And instead of having him take the train, I drive him back and forth to work almost every day when I can, just to avoid that. Our entire lives, my husband and I are very much go, go, go. . . . We were doing all the grocery orders, the Amazon Prime (now), or Whole Foods delivery. And then my husband really wanted to go grocery shopping. So we finally let up on that, but we certainly [are not shopping like in] the past. You would need something, and you would just run to the grocery store. Now we are really trying to minimize those trips. (Adel)
Although horizontal ties played important roles in facilitating preventive behavior in regard to staying home, some participants reported another side of this story: divergent attitudes and behaviors in regard to avoiding public places drove some interview participants apart from individuals they previously considered close ties.
I do think that people’s true colors have come out, from what they’re posting [on social media] or if they’re wearing a mask or if they’re going out to eat five times a week. . . . it’s just, you know, I’m realizing very quickly that I’m surrounded by a lot of people I’m similar to, but at the same time, you thought you knew somebody and you’re like, “oh, no, no, no.” We are not watching the same news sources, we are not politically aligned. (Abbie)
Beyond this, vertical ties were also key sources of information for messages about every individual preventive behavior examined in our study, including mask-wearing, staying home, and avoiding public places. Yet some participants also reported mixed messaging regarding mask-wearing had detrimental effects on trust in elected officials and institutions, at the federal level in particular. In some cases, mixed messaging from the federal government was cited as a reason for relying more on local elected officials, whom they saw as more trustworthy and reliable. In addition, when prompted by the interviewer, after stating they relied primarily on local elected officials, to explain why, some participants noted that they felt stronger resonance with messages from elected officials highlighting the potential for adoption of preventive behaviors to protect others.
Because when I listened to the governor and the mayor speak, they were much more aggressive about protecting the community than what was coming out from national leaders. And by that time . . . it seemed long past due because by that point it was really getting around. I think our first case in Boston was in January and that was publicized. So we were walking around for two more months between January and mid-March before it really reached crisis level, and whenever they would talk about it in their news conferences, they were taking a much more serious approach to, you know, this is the only way we can stop this. (Meghan)
And I would add that the other place I did go for information was Governor Cuomo. So I would listen to his daily conferences. . . . [Interviewer prompt to expand on this, and why she relied on him as a resource] Well this is gonna sound really hokey but I felt like he was being honest because he was saying how bad it was. And I think the other thing that kept coming through to me with his conferences was [that] we don’t have a cure yet. We really don’t have a treatment yet. But what we can do for each other is, you know, I hate to use the word flatten the curve, but you know, he would describe what it was like in emergency rooms and that his point was, if we can just keep it to the point where what is coming to our medical facilities is manageable, [that] will be helping all of us. And so to me, that message really resonated. (Meghan)
Increased Handwashing
Participants tended to rely on information from vertical ties to non-elected federal officials—and Dr. Anthony Fauci, in particular—for messaging on handwashing. For example, one participant (Mitchell) attributed their information on “wearing a mask, washing your hands, and those kind[s] of prevention strategies” to the CDC. Even when participants did not remember the exact source of recommended interventions, once they had internalized a behavior change, they sometimes attributed it to a trusted expert source, such as Dr. Fauci.
You’re gonna go to the national elected officials, right? Not anything from local elected officials but for the fact that they encouraged, you know, or demanded we follow what Fauci was recommending. [Interviewer: Was there anything specific you learned from Dr. Fauci that you didn’t learn elsewhere?] Well, you know, I’m assuming he was one of the first ones to say wash your hands. Wash your hands. Wash your hands. Wear a mask. Stay away. Stay home. Wash your hands, wash your hands, buy sanitizer, make sanitizer, get sanitizer. No matter how you get it, wipe down your house. Wipe down things other people touch. Wipe it down, wipe down, wipe down, and wash your hands. (Natasha)
Using Personal Protective Equipment
Finally, vertical ties were key sources of information for messages about the importance of mask-wearing and avoiding public places, as participants noted:
Governor Baker, because he’s the Massachusetts governor. I think he’s done a terrific job, but I wanted to keep track of each step along the way. In the beginning, because the outbreak had been in New York, where my daughter and my grandchildren live. I had been watching that Governor Cuomo, who also did a fantastic job. I did watch Mr. Trump for about six weeks, and at that point I decided that I really wasn’t getting accurate information from him. (Alexa)
Well, I think collectively all of them as the push to wear a mask was more strongly pushed on, by the case was made that you should wear it we embraced that fully. That was not a problem. Uh, the social distancing part of it. We embraced fully. That was not a problem. The stay at home portion of it on how you act when you go out. Not a problem. We listened to what was suggested. (Natasha)
Broadly, findings demonstrating an association between information from vertical ties and the adoption of preventive behaviors echo earlier findings regarding network effects on the adoption of health behavior (Latkin and Knowlton 2015). In doing so, they offer a more granular view of the way variation in types of social ties affects information individuals choose to rely on in crises.
THEORETICAL AND POLICY IMPLICATIONS
Our findings resonate strongly with those of other investigations that have used nuanced categorization of social capital to illuminate the role of horizontal and vertical social capital (Fraser and Aldrich 2021; Hawkins and Maurer 2010; Kyne and Aldrich 2020; Page-Tan 2020, 2021; Poortinga 2012). Research envisioning social capital in a single dimension fails to advance our understanding of how vertical, horizontal, inclusive, and exclusive ties can operate differently from one another. Furthermore, our inclusion of one-way ties expands on previous definitions of vertical social capital, facilitating valuable overlap with previous work on the role of trust in outbreak response (Vinck et al. 2019).
We find that information from trusted entities with political and administrative power shared a strong association with recommended behavior to protect individuals from contracting and spreading the novel coronavirus. Further, staying home or avoiding public places was correlated with information—and often assistance—from close, tightly knit horizontal ties. For example, one interviewee drove her roommate to and from a construction job every day to protect him from commuting via public transit. By measuring and testing these various ties, we can better understand and leverage these social ties in crises and emergencies. In sum, this research speaks to the importance of avoiding monolithic measurements of networks and trust, which would miss the differential effects of the different horizontal and vertical ties.
Further, our findings hold implications for previous work on outbreaks showing negative effects of misinformation on institutional trust and adopting preventive behaviors (Daszak et al. 2021; Vinck et al. 2019). Although we find information from trusted entities of power (vertical social capital) strongly associated with the adoption of preventive behaviors, information from federally elected officials (namely, former President Trump) known to be frequent sources of misinformation was not a significant factor in our analysis (see Kessler 2021). Some interview participants discuss the loss of trust in federally elected officials and federal institutions due to misinformation and mixed messages, resonating with findings from research during previous outbreaks (Vinck et al. 2019). Yet precedent is limited for large-scale health communication campaigns during outbreaks in the United States today (Fisher et al. 2020). Our findings complement initial studies focused on vulnerable communities (Pezzia, Rogg, and Leonard 2022, this issue; Evans et al. 2022, this issue; Burns and Albrecht 2022, this issue), reinforcing the importance of horizontal and vertical ties among a large, constituent group constituting one-fifth of the country. This underscores the need for further research to understand the dynamics of health communication, misinformation, and institutional trust in the U.S. context during the COVID-19 pandemic.
These findings have implications for policymakers both preparing for and responding to future outbreaks and other prolonged crises. Our research suggests that policies focused on disseminating information through community-level influencers and leaders—whether in faith-based organizations, civil society organizations, or schools—may have beneficial effects because these individuals’ beliefs and behavior can serve as a bellwether for others in their networks. Our findings furthermore reinforce the importance of horizontal ties in facilitating decisions regarding movement and travel during crises. When it comes to decisions about whether and how to avoid public spaces during an outbreak, the presence of close horizontal ties may mean the difference between getting a ride or taking public transit and between wearing a mask or going out unprotected. Therefore, policies facilitating the development of close ties within community and neighborhood networks—such as the development of community centers and funding for neighborhood-based civic groups—may lay the groundwork for the uptake of safe behaviors during future outbreaks by providing individuals with necessary social support structures.
Limitations and Research Agenda
As true of all social science studies, our research comes with limitations. Our respondents are not a representative sample of the U.S. population, but instead an oversampling of high-income, highly educated people in New York and Boston. Whereas social scientists typically seek massive samples to better generalize about the behaviors of larger populations, we build on research recognizing the importance of a focus on a smaller subdemographic (Burns and Albrecht 2022, this issue; Evans et al. 2022, this issue; Pezzia, Rogg, and Leonard 2022, this issue). This demographic tends to participate more often in civil society organizations as leaders (Keohane 2020) and serve as important swing voters in elections (Kurtzleben 2018). A consequence of this high human capital demographic is that our respondents tend to belong to civically engaged groups, unlike others who may engage in antidemocratic, intolerant, or high-risk behavior (Van Deth and Zmerli 2010). Whereas our sample focused on metropolitan areas, the demographic features of our respondents matched with some seventy-four million Americans who live in 235 counties across the nation.
To confirm the broader results of our sample and the possibility of generalizing our results, we conducted an additional analysis of data from the U.S. Census Bureau (2022) Household Pulse Survey, a dataset that better represents the nation. Although the Pulse survey did not capture horizontal and vertical as deeply, it did capture government trust and behavioral change during the pandemic. We performed a weighted logistic regression of individuals who had not yet received the COVID-19 vaccine. Among them, we see the odds of eating indoors at restaurants during the pandemic are predicted to be 0.670 times less (p < .001) among those who trusted government officials, versus those who indicated they did not trust the government (for details, see table A.4). These findings from an external dataset further confirm the importance of relying on linking ties in a pandemic for information, a key finding in our study, and a finding in a study of government trust and compliance with mask-wearing and social distancing guidelines (Suhay et al. 2022, this issue).
A second limitation is that we did not explicitly ask our respondents about their parental status, a factor that may affect sources of information and trust in those sources (Modestino et al. 2021). However, we did collect data on school administrators as a source of information and this factor was not statistically significant in our models. A third challenge is that our surveyed population—and the 230+ counties with similar demographics—strongly lean Democratic (almost all matched counties voted for Biden rather than Trump, for example). The vertical ties we see to authorities like Governor Cuomo and Dr. Fauci likely correlate with reinforcement from partisan media sources and their own horizontal networks. Thus we cannot make inferences about Republican individuals in red-leaning areas where partisan media sees these authorities as untrustworthy.
Future research, then, should seek to include survey questions about participant parental status and better include a broader set of partisan respondents to ensure broader generalizability across the broader U.S. population.
CONCLUSION
The COVID-19 pandemic called for public health communication efforts of a scope and scale unprecedented in the United States today (Fisher et al. 2020), in that Americans were inundated with information about the importance of nonpharmaceutical interventions—such as staying home and avoiding public places, wearing PPE, and handwashing—to curb the spread of disease. Our research demonstrates the importance of social networks—information embedded in horizontal and vertical social capital—to individual adoption of safe behaviors. Associations between vertical social capital and adoption of all three preventive behaviors we study, alongside an association between close horizontal ties and avoiding public places during the early months of the pandemic, further underscore the importance of using nuanced categorizations of social capital, as opposed to treating social capital as a monolith (see also Fraser and Aldrich 2021; Hawkins and Maurer 2010; Kyne and Aldrich 2020; Page-Tan 2020, 2021; Poortinga 2012).
These findings represent an early step in unpacking the complex dynamics of social and civic networks as information sources for health communication in the United States during COVID-19. Interpretation of our findings is limited by the nature of our sample, which is limited to two northeastern U.S. metro areas, namely, Boston and New York. Survey participants were disproportionately White, upper-middle-class, and politically liberal, mirroring a suburban population subset of seventy-four million people to add critical context to studies of health communication typically (and rightfully) focused on vulnerable groups. In highlighting weaknesses in the U.S. health-care system—including inexperience with mass health communication efforts—the pandemic underscores the need to understand how such efforts are received across broad swaths of the population, including privileged groups historically facing fewer obstacles in access to health care. Future studies should examine the extent to which these findings hold among samples more demographically representative of the U.S. population. Further, panel data are needed to capture variation and trends over the course of a prolonged crisis. To address this, our research group conducted follow-up studies in February 2021 and February 2022.
Developing a more nuanced understanding of the role civic networks play in information-sharing during prolonged crises has important implications for policymakers and communities. This applies to both preventive initiatives—such as incentivizing the development of horizontal ties within neighborhoods and communities—as well as crisis response efforts—including targeting health communication to reach key stakeholders within community networks. Further, these findings contribute to integrating social science approaches with public health research to better inform policy in future crises (see Subbaraman 2021). Given that our societies are certain to face shocks in the future, sophisticated, social capital, and social-infrastructure-based responses will better help us build resilience to these shocks.
FOOTNOTES
↵1. The majority of respondents are from Boston, Brighton, Brookline, Brooklyn, Cambridge, Chelsea, Dedham, Dorchester, Newton Center, Roslindale, Staten Island, or West Roxbury.
- © 2022 Russell Sage Foundation. Page-Tan, Courtney, Summer Marion, and Daniel P. Aldrich. 2022. “Information Trust Falls: The Role of Social Networks and Information During the COVID-19 Pandemic Among Suburbanites.” RSF: The Russell Sage Foundation Journal of the Social Sciences 8(8): 32–51. DOI: 10.7758/RSF.2022 .8.8.02. We acknowledge the financial support from the Natural Hazards Center via its Quick Response Grant, the Natural Hazards Center through its CONVERGE COVID-19 leadership grant, the Northeastern University College of Social Science and Humanities Research Development Initiative, and the Natural Hazards Center via a Quick Response Grant for Changing Political and Economic Landscapes: The Role of Civic Networks and Information Sources During the COVID-19 Pandemic. Further, we thank our research assistant Simran Kaur for her assistance in conducting one-on-one interviews, and Cameryn Martin, Melinda Medina, and Clara Moreno for their research assistance. Direct correspondence to: Courtney Page-Tan, at courtneypagetan{at}gmail.com, Embry-Riddle Aeronautical University, 1 Aerospace Boulevard, Daytona Beach, FL 32114, United States.
Open Access Policy: RSF: The Russell Sage Foundation Journal of the Social Sciences is an open access journal. This article is published under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.
REFERENCES
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.