
Abstract
Early-life conditions are associated with mortality in men, but not studied to the same extent in women. We add new evidence by studying a cohort of women born between 1916 and 1931 and followed for mortality between 1986 and 2013. Our sample from Iowa includes a significant number of rural women, from both farms and small towns. The long-term effects of growing up in a rural area were mixed: farmers’ daughters lived longer than women growing up off-farm in rural areas. Daughters of farm laborers and skilled or semi-skilled trades workers fared worst, when considering early-life socioeconomic status. We also find evidence that migrating to small-town Iowa was associated with lower life expectancy after age fifty-five. Considering social class and farm-nonfarm status is important for understanding the health of rural America.
A substantial body of research in the social and medical sciences has now established that stress and economic deprivation in early life can have long-lasting effects on individual health and well-being. Thus the roots of contemporary health conditions in adults, and differences between groups in health status and life expectancy, can be partly traced to adverse experiences in early life. A wide range of interrelated childhood influences can bear on later-life health and mortality, including early-life health itself, and children’s social and economic environment (Elo and Preston 1992; Haas 2007; Hayward and Gorman 2004; Kauhanen et al. 2006). Poor health in childhood has been shown to be associated with poorer health in adulthood in different cohorts in both the United States and Britain (Blackwell, Hayward, and Crimmins 2001; Haas 2008; Kuh and Wadsworth 1993; Wadsworth and Kuh 1997). In turn, health status in both childhood and adulthood is influenced by current and past socioeconomic status (Cohen et al. 2010).
Much of the literature on the effects of early-life circumstances on later-life health and mortality has focused on the experiences of cohorts born since World War II and either followed prospectively or asked retrospectively about their early-life circumstances (Brandt, Deindl, and Hank 2012; Montez and Hayward 2011). Although these cohorts include both men and women, by definition they are relatively young, having only reached their seventies at the time of writing. Representative population samples begun since World War II are likely to have relatively small numbers of rural residents. By the census definition of urban, 57 percent of the country was living in an urban area in 1950 (Boustan, Bunten, and Hearey 2018). Research on earlier cohorts, born between the 1890s and 1940 and more likely to include people growing up in rural America, has relied on prospective long-term follow-up of pioneering early twentieth-century studies (such as the Harvard, Oakland, and Fels growth studies) and linkage between early-life census records and later-life health and mortality outcomes (Aizer et al. 2016; Ferrie and Rolf 2011).
Thus studies of life-course health processes over the long term have somewhat neglected people with rural origins. Moreover, studies of early twentieth century cohorts have underrepresented women. Again, practical considerations of sample or variable availability are a significant reason for this oversight. Women are difficult, but not impossible, to trace over time due to the nearly universal practice of changing surname on marriage (Ruggles, Fitch, and Roberts 2018). Although this is common in Western societies, the practical implications for record linkage are exacerbated in the United States by the diffusion of marriage recording across county government. In countries with centralized marriage registration at the national (such as Britain and New Zealand) or first subnational level (such as Australian states and Canadian provinces) tracing women across the life course is easier. It is clear from the literature that the influence of early-life conditions on adult health and mortality differs across time and social context (Currie and Vogl 2013; Galobardes, Lynch, and Davey Smith 2008, 2004). It is less clear whether the effects differ across the sexes (Power, Hyppönen, and Davey Smith 2005) and what the impact of different residential origins are.
We address a key gap in the literature by examining early-life circumstances and late adult mortality in a group of American women born between 1916 and 1930 and followed in the Iowa Women’s Health Study since 1986. This is an earlier cohort than previously considered in studies of women’s early-life conditions. Women in this cohort had a significantly different fertility and labor-market profile in their adult lives than surrounding cohorts. This cohort represents the mothers of children born during the baby boom. Yet they are also a cohort that reentered the labor force in significant numbers after childbearing, in contrast to earlier generations of American women. Considering for the moment only national migration trends, this cohort also saw significant movement from rural childhoods to urban (or suburban) adult lives. We find that growing up or moving to a farm was associated with better health outcomes, and that for women of any residential origins in childhood moving to a city or large town was associated with better health in later life. Across several dimensions of social status and health, we observe that living in nonfarm rural areas in earlier or later life is associated with worse outcomes and lower social status. To be specific, these women are living off-farm in towns with a population of under 2,500. Given this and the generally positive findings for farm residents at any point in the life course, we conclude that understanding what it means to grow up and live in rural America is heavily conditioned by social class and occupational opportunities. The finding in our cohort of a mortality difference for women living in nonfarm rural areas in later life is suggestive of important changes in the opportunities and challenges of rural areas that have emerged in recent decades.
BACKGROUND
A full life-course perspective is important for understanding and addressing rural health disparities. The “rural mortality penalty” in the United States dates only to the 1980s (Cosby et al. 2019) and is not uniform across regions (James, Cossman, and Wolf 2018)—higher disparities exist in the South—or across age groups, given that excess rural mortality is concentrated in working-age populations (Elo et al. 2019). Because the rural mortality penalty is relatively recent, many Americans adults in both urban and rural areas grew up in an era when infectious disease and environmental hazards from industrial activity meant an urban mortality penalty. Through the mid-twentieth century, improvements in public health reversed these differences (Haines 2001). In the same period, substantial rural-to-urban migration in the United States continued, more than three-quarters of the country living in urban areas since the 1970s. Yet in cohorts born before World War II, rural origins were common. The long-term impact of growing up in rural or urban settings has, however, often been addressed by classifying residence at a single point in time, such as birth or a single point in childhood. Rural mortality patterns today reflect a long-term process of migration and compositional change. Understanding why older (sixty-five-plus) rural residents have not experienced the same health disparities as those of working age over the past thirty years can inform policies to improve health for the next generation of older rural Americans.
Estimating the impact of birth to early-adult experiences on later health is challenging. At a minimum, it requires data on thousands of individuals at two time points. Because large cohort studies were not initiated until after World War II, understanding the early lives of people born before 1940 requires a different approach. One approach is to ask retrospective questions about early life. Such an approach has been used fruitfully by the Health and Retirement Survey, the Panel Study of Income Dynamics, and the National Longitudinal Survey of Older Men (Havari and Mazzonna 2015; Hayward and Gorman 2004; Smith 2009). Retrospective questions have two significant limitations: they can only be asked of surviving cohort members, and they are dependent on memory, which often falters with age (Brown 2014). An alternative is linking multiple sources across time. In early life, these sources could be a census, health survey, or institutional roster with health information. In later life, they could include health surveys, medical records, or death records.
STUDY CONTEXT
We take advantage of an epidemiological study conducted since the 1980s. The Iowa Women’s Health Study (IWHS) is a prospective study of 41,836 women age fifty-five through sixty-nine at baseline in 1986 and followed until 2014. The sampling frame was the 1985 Iowa driver’s license list; because driving was near universal in the United States in the second half of the twentieth century, a driver’s license registry provided an efficient and representative listing of adults for population samples.
Iowa in the Early Twentieth Century
The members of the Iowa Women’s Health Study were born between 1916 and 1931. Neither the drivers’ license registry nor the baseline questionnaire asked women where they were born. However, from census samples for 1980 and 1990 for the state of Iowa, we can describe the target population: women born between 1916 and 1931 and living in Iowa. More than 90 percent of the cohort eligible to be included in the IWHS were born in Iowa (85 percent) or the six surrounding states. Using the 1920 Census as a gauge, the population of Iowa was less urban (defined as incorporated areas with more than 2,500 persons) than the United States as a whole and fewer people lived in large cities (see table 1). However, its rural residents were much more likely to live in incorporated places than their counterparts in rural areas outside Iowa. Indeed, nearly the same fraction of Iowans lived in incorporated places as in the country as a whole. The Iowa landscape at the time was dotted with hundreds of small towns, and its population density actually exceeded that of the nation’s. Nearly 10 percent of Iowa’s population was foreign born. Emigrants from Germany made up the largest single share, not much lower than the nation as a whole. However, like most of the Upper Midwest before the Great Migration, Iowa had significantly fewer African American residents at the time. In 1920, the dominant industry in the state was agriculture, whereas male employment was more evenly split between manufacturing and agriculture in the rest of the country.
Key Demographic Characteristics of Iowa and the United States in 1920
Despite being more rural, Iowa (along with several other prairie states) was at the forefront of the “high school movement,” the rapid spread of taxpayer-funded secondary schools in the early twentieth century. The expansion of the American high school in the nation’s heartland was in part explained by the fact that the wealth in these states was tied to land, a source more easily taxed than more mobile forms of capital, and in part by the more even distribution of wealth in the region. The relative racial and ethnic homogeneity of the Upper Midwest, the dominance of the Protestant faith, and the preponderance of small towns were also factors that facilitated the spread of high school attendance (Goldin and Katz 1999). Using unique data collected by the state of Iowa in a 1915 state census, the economists Claudia Goldin and Lawrence Katz (2000, 790) estimate that the average years of schooling completed by an Iowa child was at a level that would not be “equaled in the entire United States until about 1940.” In other words, Iowa was a generation ahead of the nation. As a result of the earlier expansion of high school education, Iowa had more high school graduates than the nation as a whole did in 1940, and still leads the nation in the percentage of students graduating, more than 91 percent relative to the national average of 85 percent.1
Goldin and Katz (1999) speculate that the same economic and social features that facilitated the spread of secondary education may also have contributed to greater stocks of local social capital in Iowa and the states like it. Iowa’s higher-than-average turnout rate in the 1920 presidential election, its participation in the Liberty Bond drives of World War I, as well as reported Red Cross membership rates in 1918 are consistent with that interpretation (table 1).2 Iowa still is a leading state on contemporary measures of social capital (Hawes, Rocha, and Meier 2013; Rupasingha, Goetz, and Freshwater 2006), though it has not been immune to the changes that have led to a decline in social capital across the nation (Besser 2009).
Iowa in the 1980s
Members of the IWHS completed their baseline interviews in 1986, a time of severe economic stress in the nation’s heartland rivaling the severity of the Great Depression. In the 1970s, federal policymakers encouraged farmers to plant “fencerow to fencerow” to take advantage of steep rises in the price of agricultural commodities occasioned by surging international demand for U.S. farm exports in China, Russia, and other parts of the world. American farmers invested heavily in both land and equipment to expand production, investments made possible by the cheap credit offered by the nation’s lenders. As a result, the debt that farmers carried on their balance sheets ballooned, rising nearly 80 percent from 1970 to 1980. Land values rose even more than agricultural prices, drawing in speculators that bet on continued good times, further pushing up the price of farmland (Barnett 2000; Peoples et al. 1992).
The 1970s boom ended abruptly for several reasons. Export markets dried up, causing commodity prices to fall more than 50 percent between 1981 and 1986, and farmers’ income suffered accordingly. Falling prices ended the speculative frenzy in farmland, and land values plunged. At the same time, the Federal Reserve raised interest rates aggressively to combat high inflation. Many farmers were underwater, that is, unable to refinance their loans because of cash-flow problems, tighter credit, and assets worth considerably less than their purchase price. Farm bankruptcies and foreclosures soared, and many rural banks failed (Harl 1990). Between 1978 and 1987, more than twenty thousand farms in Iowa ceased operating; in some counties, the number of farms declined by more than 20 percent (U.S. Census Bureau 1987).
The effects of the 1980s Farm Crisis extended well beyond Iowa farmers and their families. In addition to rural bank failures, 41 percent of rural gas stations went out of business, hundreds of automobile dealers closed up shop, and almost five hundred grocery stores were shuttered—five per county, a decline of more than 20 percent across the state. Construction sales plunged by more than 40 percent during the decade and unemployment rose. Hard-hit Iowa counties lost population as families migrated to areas of greater opportunity, school enrollments declined, and rural populations become older and poorer as a result (Conger and Elder 1994). This “shake out” (Friedberger 1989) was not unlike the restructuring that would happen in other parts of the country three decades later as a result of the 2008 financial crisis, import competition from China (Acemoglu et al. 2016), and increasing automation (Acemoglu and Restrepo 2020), factors that may have contributed to the opioid crisis and “deaths of despair” among middle-aged white Americans (Case and Deaton 2017; Pierce and Schott 2018).
Study Population and Potential for Record Linkage
The IWHS began around the same time as the 1980s farm crisis. Like any longitudinal study, the cohort and the study are a product of their time. Important research foci for the initial investigators were diet, nutrition, and risk factors for cancer and cardiovascular disease. Because the IWHS had been designed as an epidemiological study, significant effort went into collecting food frequency diaries and relatively less into measuring social and economic factors across the life course. Looking back through the lens of more recent developments in life-course sociology of health, we can recognize the single-risk factor epidemiologic approach critiqued by scholars in the 1990s during the development of fundamental cause theory (Link and Phelan 1995). Cancer incidence was ascertained via annual linkage to the State Health Registry of Iowa, a member of the Surveillance, Epidemiology, and End Results program. Through 2014, 26,472 deaths were recorded (see table A.1 online).
Respondents differed in a range of ways from nonrespondents, and potential biases went in different directions (Folsom et al. 1989): respondents were from less affluent areas but also tended to be lighter. The baseline questionnaire asked about a variety of cancer and other health risk factors, including age, smoking behavior, physical activity, education, and alcohol consumption. Weight, fertility, and family medical histories were also collected at baseline. Driver’s license information indicated that respondents’ self-reported body mass index (BMI) was 0.4 kg/m2 lower. Respondents were more likely to live in rural and less affluent counties (Folsom et al. 2000). Despite these differences in baseline health and socioeconomic status, the association of body weight with mortality and cancer incidence was similar in respondents and nonrespondents (Bisgard et al. 1994). Women rated their health on a 4-point scale (excellent, good, fair, poor). Follow-up questionnaires were mailed in 1987, 1989, 1992, 1997, and 2004, providing several measures of the trajectory of health in later life (Ahmed et al. 2008).
Despite collecting a limited amount of social and economic data at baseline, and in follow-up surveys, the IWHS provides an unusual and important opportunity to add objective measures of early-life circumstances to a longitudinal study of aging women. Tracing men forward or backward in time is relatively straightforward because men do not change their name at marriage. An extensive literature now links men between different census enumerations or from the census to mortality records (Aizer et al. 2016; Beach et al. 2016; Ferrie and Rolf 2011). Objective measures of early-life circumstances are important because their impact is attenuated when studies use recalled information (Galobardes, Lynch, and Davey Smith 2004). The IWHS was originally designed to study mid- and late-life influences on health and mortality, not the extended reach of early childhood conditions on mortality after age fifty-five. However, a baseline question on maiden name has allowed the study to be repurposed in its own later life.
The question on maiden name was designed to facilitate mortality follow-up, as some states include maiden names on death certificates as an additional attribute to identify individuals and verify the age of death through linkage to birth certificates. At the 1986 baseline interview, 97 percent of the women provided either a maiden name or were never married, implying that their current last name was likely to have been their name in early life. Because IWHS subjects were born between 1916 and 1931, their early-life census records are now publicly available (Ruggles 2014). Complete electronic databases of the 1850 to 1940 Censuses can be obtained for scholarly research through the Minnesota Population Center (Ruggles, Fitch, et al. 2021). Restricted-use versions of the data contain names and low-level geographic information that allow individuals to be identified.
The potential is significant for IWHS subjects to be linked to multiple early-life records to develop a dataset of life-course social and economic circumstances for the cohort. Because a large share of the cohort were born in Iowa or surrounding states, our search space for matching women on the basis of name, race, and age is limited, increasing the likelihood of finding unambiguous matches, or matches that can be identified with an acceptable degree of (un)certainty. Born fairly uniformly between 1916 and 1931, the IWHS cohort can be identified in multiple early-life censuses. Federal censuses from 1920 to 1950 included a core of information that allows reconstruction of residential and socioeconomic trajectories (see table A.2 online).
We estimate we can match more than thirty-five thousand IWHS subjects to at least one early-life census record, and around twenty-eight thousand to all of their 1920 to 1950 census records (see table A.3 online). Even after adjusting for more under-enumeration than occurred in the region (Hacker 2013), we expect we could link nearly thirty-three thousand IWHS subjects to multiple records, including more than twenty-six thousand to three censuses, and fourteen thousand to four or more early-life records. Because our links to early-life records are retrospective, linkage failure is not as consequential as in prospective studies. It is highly unlikely that under-enumeration or spelling errors in early life are correlated with mortality.
DATA
In this article, our scope is more modest because we work with a subset of the best matches between the IWHS cohort born before April 1, 1930, and the 1930 Federal Census of Iowa. Thus we miss women not yet born and those who were outside of Iowa at that point, around one-sixth of the sample. We identified IWHS subjects who were alive in April 1930 (39,621 of the total study population) and matched them to 1930 federal census records from Iowa. Potential matches were identified in a comparison of names in the IWHS and census records, adapting procedures used for the construction of the IPUMS Linked Representative Samples (Goeken et al. 2011). We searched among census records plus or minus one year of the age the IWHS subjects would have been in 1930. Two trained research assistants independently reviewed potential matches. The subjects selected for this analysis were cases for which only one potential match was found in the census records, the census record matched only one IWHS subject, and both research assistants recorded the match as legitimate.
We matched 10,375 women to early-life census records, restricting matches to women resident in Iowa in 1930 in order to bring in additional, consistent county-level data collected from state government publications. Although state of birth information was not collected in the IWHS, we can assess the effects of this sample restriction in several ways. In the first instance, we can assess whether the linked sample was representative of the populations from which it was drawn. Significantly, the sample matched to early-life records was representative of both populations: the cohort of females up to age thirteen resident in Iowa (see table 2), and the full IWHS sample (see table A.4 online).3 Significant numbers of women were found in every county in Iowa (see figure A.1 online). The major substantive difference is that early-life matches are more likely to come from farming households than their counterparts in Iowa in 1930. We expect this to have occurred because of stronger intergenerational persistence in place and occupation for people who owned farms (Baker, Duffy, and Lamberti 2001; Feigenbaum 2018; Fink 1986). Despite a structural move out of farming, Iowa continues to be a heavily agricultural state and inheritance of farmland and a farm business remain a key mechanism by which people enter farming as adults. On the other side of the process, we match a smaller than expected number of never-married women out of the IWHS sample to early-life records. 95 percent of the sample linked to the 1930 Census had been born in Iowa, with another 3.5 percent born in the six surrounding states.
Characteristics of 1930 Iowa Cohort and IWHS Early-Life Matches
More broadly, we can assess external validity of the Iowa sample through comparison of the cohort of Iowa-resident women who would later be eligible to participate in the IWHS to other women of the same cohort in the 1980 federal census. Iowa today is not representative of the United States. But in the early twentieth century, it was quite representative of the white population (Goldin and Katz 2000). Three-quarters of the eligible cohort had been born in Iowa and were likely to have lived there for their entire life given migration patterns in this cohort. The cohort resident in Iowa were 98.6 percent white relative to the national average of 88.5 percent. Yet the racial composition of this cohort in Iowa was similar to that seen in other states in the Upper Midwest, New England, the Great Plains and Mountain West. On other important dimensions, women eligible to participate in the IWHS were representative of white American women their age across the country, having nearly identical rates of marriage, fertility, and labor-force participation.
The most significant difference in adulthood between the IWHS study population and white American women of the same cohort is that the IWHS cohort was significantly more likely to be rural. At the 1986 baseline interview, 19 percent of the IWHS sample were living on a farm, and an additional 19 percent were living in a rural area or a town with fewer than one thousand people. Although the IWHS cohort is distinctive for being rural in later life, growing up in a rural area was common for women born between 1916 and 1931, and our sample represents reasonably well the distribution of childhood environments for white Americans in the early twentieth century, lacking only a major metropolitan area. At the 1930 Census, 48 percent of American women born between 1916 and 1930 lived in a rural area.
MEASURES
For early-life residence, the 1930 census identified residential location with more or less precision in urban and rural areas. In cities and towns, this was a street address. Approximately half of Iowa had a street address in 1930. In rural areas (townships with a population of less than 2,500) information is less precise, but no worse than location within a five- by five-mile area. We categorize women in 1930 as living in one of three statuses: on farms, in rural areas off-farms, or in urban areas.
The 1930 census collected information on adult occupations, which have been coded by IPUMS into the U.S. Census Bureau’s 1950 occupational categories, for early-life socioeconomic status. We aggregated these occupational categories further into variables denoting whether fathers worked in white-collar jobs (professionals, managers, clerical and sales workers), as farmers, skilled or semi-skilled workers in manufacturing, utilities, and transport, or as laborers in farming or industry. We measure the economic status of mothers through a binary variable for labor-force participation. Distinguishing different occupations for women workers is less important, because labor-force participation by married women at this time was very low; nationally fewer than 10 percent of white married women worked and in Iowa 7 percent of married women.
Later-life residential status was classified by the IWHS into six categories: farm, rural, and four categories of town or city size from the 1980 census: fewer than one thousand people; between one thousand and 2,499 people; between 2,500 and 9,999 people; and ten thousand or more. For ease of interpretation and consistency with the early-life measures, we collapse some categories. The identification of town or city size is made on an urban area basis. Small administrative municipalities that were functionally part of a larger urban area are classified into urban areas. For example, a small municipality contiguous with Des Moines (a suburb), would be classified as being in the metropolitan area.
In regard to adult health and sociodemographic status, we measure baseline health at age fifty-five through sixty-nine through BMI, and smoking status (never smoked, currently smoked, past smoker). Family structure at the baseline interview was measured by a question on current marital status. Because the IWHS cohort was composed of women older and younger than typical retirement age, a question on current employment would not accurately capture the socioeconomic position of women. The baseline questionnaire therefore asked about usual work done for “most of your life,” classifying response into homemakers, professionals and managers, clerical and sales work, craft and service work (associated with greater physical intensity), and agricultural work.
Mortality follow-up was carried out nationwide via linkage to the Iowa death registry and National Death Index.
ANALYSIS
Our analysis focuses on describing the differences in social characteristics in baseline health status and survival after 1986 in relation to migration between urban and rural areas within Iowa between 1930 and 1986. Starting from detailed information on residential locations at each point we categorize women’s migration patterns into one of twelve categories summarized by the cross-categorization, and summarize the distribution of key social and health characteristics within these categories (see table 3). Although we are summarizing life-course trajectories somewhat crudely with information at just two points in time (1930 and 1986), the combination of different social and migration statuses necessitates a multivariate approach to further understand health trajectories. Because not all of our sample is deceased, and right censoring is an issue, we use Cox proportional hazard models to estimate hazard ratios of childhood, family structure, socioeconomic status, place of residence, and migration trajectories. The chance of surviving from the start of 1986 through the end of 2013 is, of course, strongly influenced by age at study entry, which varies between fifty-five and sixty-nine. Thus we control for age at entry in all models.
Residence in 1930 and 1986
RESULTS
Although record linkage across long periods is inherently selective, our sample is reasonably, maybe even remarkably, representative of both the cohort of girls (born between 1916 and 1930) living in Iowa in 1930, and of the cohort of women in the IWHS in 1986. We matched a sample of 10,375 women from the IWHS to 1930 federal census records. We expected that women who survived and remained in Iowa at the time the IWHS began in 1986 to be distinct from the cohort of girls resident in Iowa in childhood because migration and mortality are not random. However, our sample matched the total cohort of girls in Iowa in 1930 closely (see table 2). The most significant difference between our matched sample that survived to be in the IWHS and the 1930 Iowa girls was that our sample was more likely to be living in a rural area or on a farm in 1930, and slightly more likely to be living in a family with both parents present. Similarly, we find the group matched to early-life records has a very similar distribution of social and health characteristics in 1986 to the entire IWHS cohort (see table A.4).
More than half a century after the 1930 Census, we observed 24 percent of our cohort still living in the same county. Even in the light of declining intercounty (domestic) migration over the twentieth century (Fischer 2002), we are inclined to regard this proportion as a high rate of persistence in the same place. Yet, given the combination of setting (Iowa) and sample selection (women age fifty-five to sixty-nine at baseline) this level of persistence is consistent with expectations. Among women born in Iowa in the same birth cohort, slightly more than half had migrated to other states by 1980. We observed no substantial differences in the social characteristics or baseline health status by intercounty migration status. That is, anthropometric measures and self-rated health at the 1986 baseline survey were similar among women who remained in the same county and those who moved.
Given the declining rural population share of Iowa from more than 50 percent in 1930 to less than 20 percent in 1986, we observe a substantial movement of women out of farm and other rural residential locations and into towns and cities (see table 3). However, the rural-to-urban shift is one seen more in the aggregate than in individual trajectories. Nearly a quarter of women growing up in Iowa’s larger cities in 1930 were in 1986 living on a farm or in townships that would have been classified as rural by the historic census bureau definition (a population of less than 2,500 defining the border between urban and rural). Women observed in 1930 in smaller towns and cities or nonfarm rural areas had the most diverse 1986 destinations, being relatively less likely to be in the same type of place than either the farm or city girls of 1930. The residential patterns we observe here reflect the population geography of Iowa—a state whose largest metropolitan area is around half a million and where the organization of farming and agricultural processing industries has produced a state with many small towns and cities.
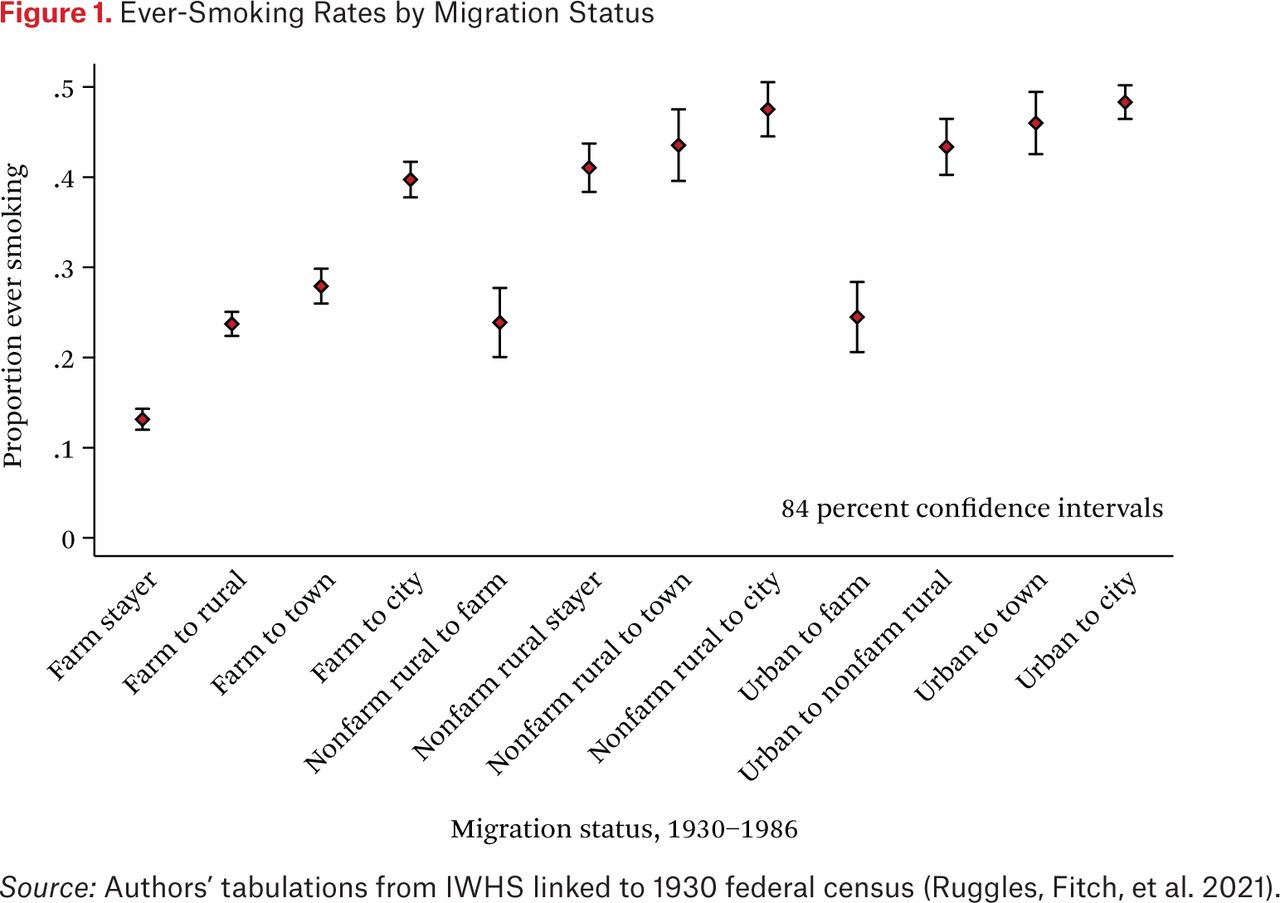
We observe important social and health differences between women in different migration states (see table A.5 online). Women migrating to urban areas, whether from farms or nonfarm rural areas, had higher rates of college attendance than women remaining on, or moving to, farms. Women who ended up in cities in 1986 had higher rates of attending college (see figure A.2 online), reflecting that college attendance often migrating out of the county.4 Although college attendance and graduation is positively associated with health status in the contemporary United States, the effects of migration to urban areas were less clear in the mid-twentieth century. Smoking rates were significantly higher in urban areas. For the majority of women in our linked cohort, who grew up on farms, the difference in rates of ever smoking (see figure 1) between those who remained on farms (0.13), and those who ended up in towns of larger than ten thousand in 1986 (0.39) was threefold.

Ever-Smoking Rates by Migration Status
Source: Authors’ tabulations from IWHS linked to 1930 federal census (Ruggles, Fitch, et al. 2021).
Both origins and destination were important in women’s adoption of smoking. Migrants to farms had smoking rates nearly half that of their peers seen in 1930 off the farm (either nonfarm rural, or any urban area). Similar patterns are evident for current smoking rates (figure A.3 online). Smaller differences in health indicators are evident when comparing BMI (figure A.4 online) and the likelihood of reporting excellent health (figure A.5 online) at the baseline interview.
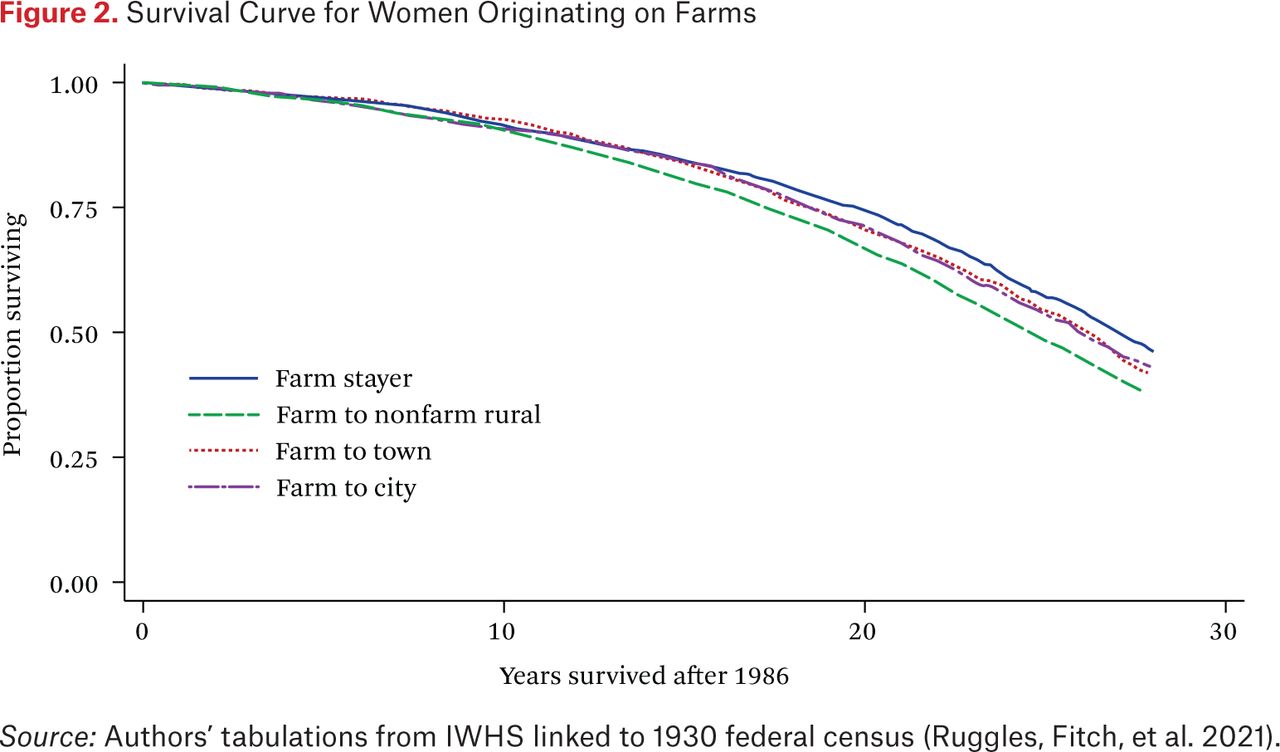
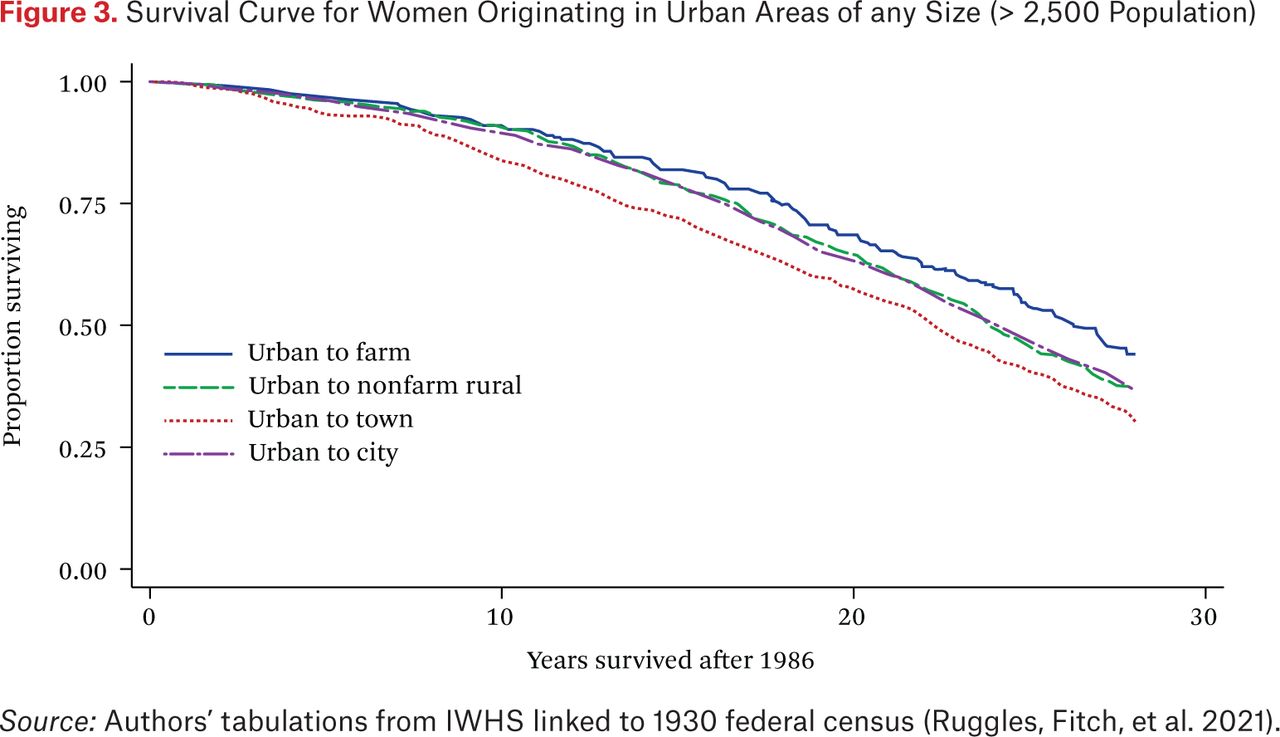
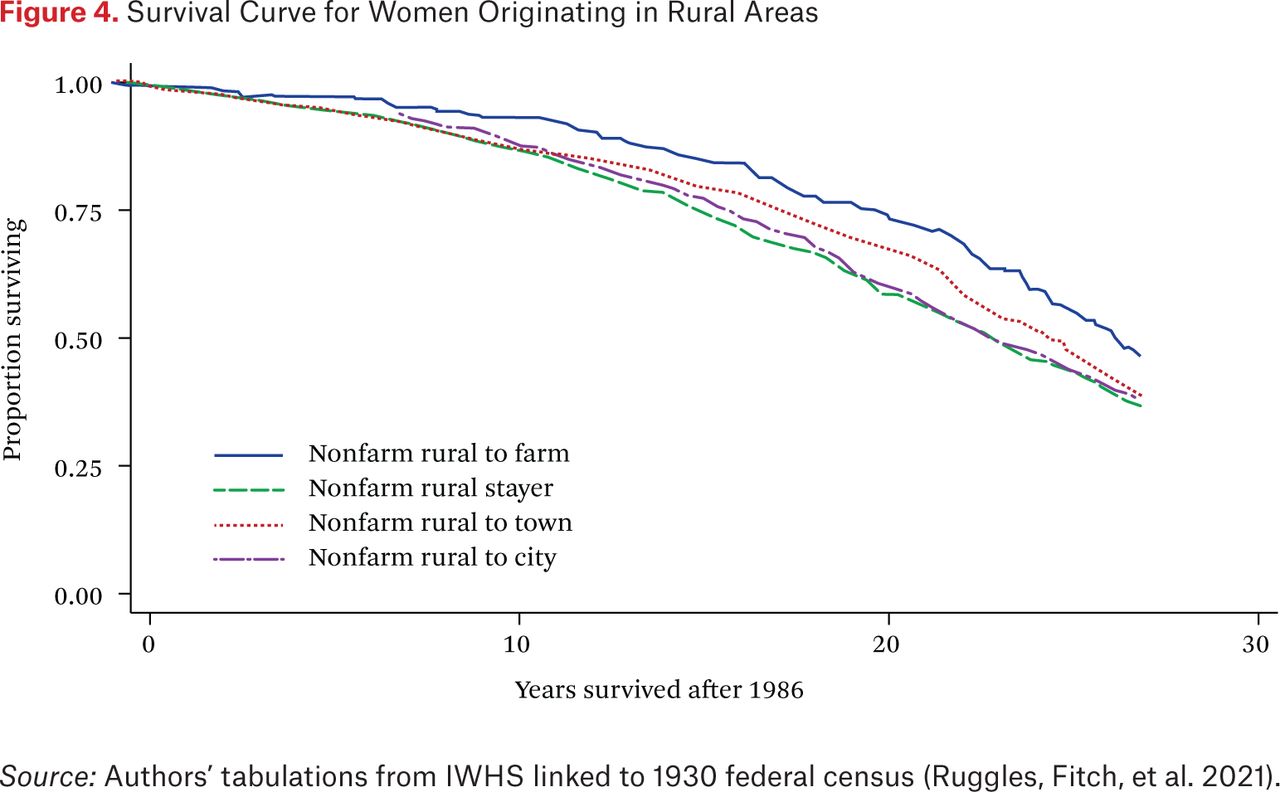
These general patterns of health advantages for farm stayers and migrants to farms, and social disadvantage for women in nonfarm rural areas later in life continue when we examine survival profiles for women in the twenty-eight years of follow-up following the baseline interview. Originating on, or moving to a farm, is associated with higher survival (see figure 2). Women who were living in an urban area in 1986 (see figure 3), but moved to a small town had poorer survival than those moving to farms or staying in the city. Similarly, women originating in nonfarm rural areas had higher observed survival when migrating to a farm by 1986 (see figure 4).

Survival Curve for Women Originating on Farms
Source: Authors’ tabulations from IWHS linked to 1930 federal census (Ruggles, Fitch, et al. 2021).

Survival Curve for Women Originating in Urban Areas of any Size (> 2,500 Population)
Source: Authors’ tabulations from IWHS linked to 1930 federal census (Ruggles, Fitch, et al. 2021).

Survival Curve for Women Originating in Rural Areas
Source: Authors’ tabulations from IWHS linked to 1930 federal census (Ruggles, Fitch, et al. 2021).
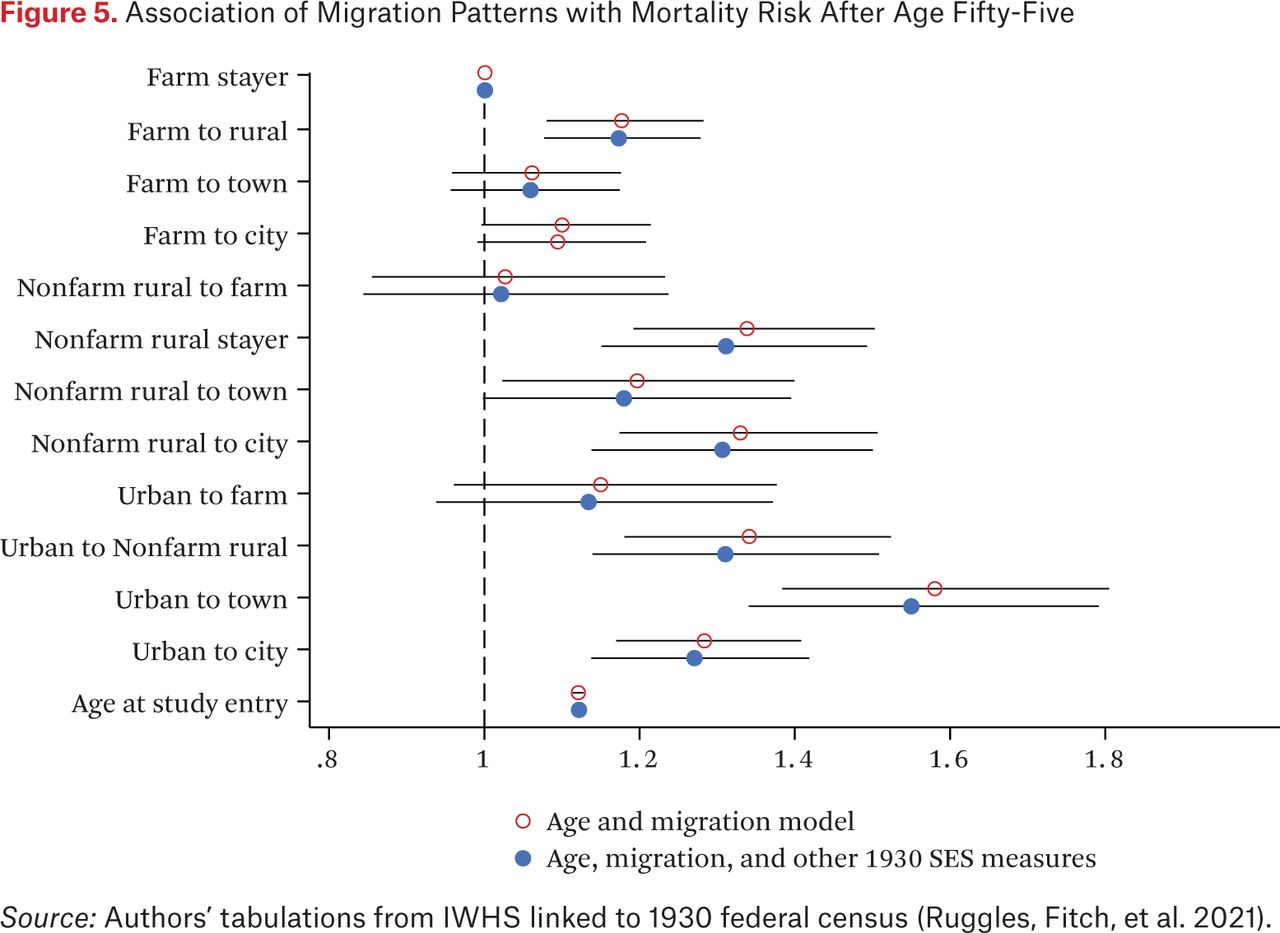
With important differences in social characteristics and health behaviors at baseline by migration status we turn to a multivariate model to describe and explain these patterns (see table A.6 online). We observe important differences in mortality along multiple dimensions of early life experience. The mortality risk for girls growing up on farms and remaining there is significantly lower. Given the twelve categories of migration origins and destinations between 1930 and 1986, interpreting the association of all-cause mortality with migration is complex. The association of migration patterns and mortality is only slightly affected by controlling for socioeconomic status in childhood—the estimates are very stable when comparing a basic age and migration model, with a model including 1930 characteristics (see figure 5). The patterning of migration and mortality is clearer visually, and we draw attention to two features of these results. First, it was advantageous to originate or move to a farm. Girls who grew up off-farm in 1930 in a small town (fewer than 2,500 people) but moved to a farm had nearly the same mortality risks as those growing up on a farm and remaining there. Similarly, girls who grew up in urban areas (a population of 2,500 or more in 1930) and moved to a farm had the lowest mortality risk of any subgroup originating in urban areas. Second, originating in or moving to a nonfarm rural area was associated with generally higher mortality.

Association of Migration Patterns with Mortality Risk After Age Fifty-Five
Source: Authors’ tabulations from IWHS linked to 1930 federal census (Ruggles, Fitch, et al. 2021).
Cause-specific mortality estimates provide additional insight into the potential mechanisms behind these associations. In general, we observe that cardiovascular and respiratory mortality is more strongly associated with migration patterns than cancer mortality (see figure A.6 online). Cancer mortality risk only shows a significant association with farm to rural and urban to small-town migration. These migration statuses had the highest current smoking rates in the 1985 baseline survey (see figure A.3). Cardiovascular and respiratory deaths are associated with more migration trajectories and with more common migration trajectories. Cardiovascular and respiratory mortality was higher for women staying in nonfarm rural residence, moving from nonfarm rural origins to a city in later life and originating in an urban area and ending up anywhere except a farm. Similarly, cardiovascular and respiratory mortality, but not cancer mortality, is associated with indicators of early-life socioeconomic deprivation and stress: living in a home that was rented or in a single-parent household (figure A.7 online). Children living with neither their mother nor father in 1930 had lower all-cause and cardiorespiratory mortality after 1986, reflecting the fact that the majority of children seen with neither parent in 1930 were living with aunts or uncles, or both grandparents. Although the census does not identify that these children were orphans, it is highly likely that they were.
We see only small mortality gradients in father’s occupation compared to girls whose father was a farmer. The daughters of farm laborers and tradesmen may have fared slightly worse than daughters of farmers and white-collar workers, with the difference significant at the 10 percent level. We suspect this reflects that social class differentials within Iowa are muted relative to those in the entire United States.
DISCUSSION
The demography of rural and urban residence has changed significantly in the United States in the past century, having potentially important long-term consequences for health and mortality in later life. In the early twentieth century—when the current generation of older Americans were children—living in rural areas or on farms was common. Migration out of rural areas and away from farms has been significant. Working out how selection of people into and out of rural areas affects life chances is important for understanding the opportunities and challenges of growing up in rural America. Examining the experience of a sample living in favorable circumstances—Iowa was a state that invested significantly in girls’ education (Goldin 1998; Goldin and Katz 2000), and social capital was high—and surviving to at least age fifty-five, we find that migration to small towns and nonfarm rural areas is associated with higher mortality and poorer health. The childhood origins of these women were not distinctly different, but their health, social circumstances, and mortality are somewhat worse than women in larger towns and cities or on farms. Growing up on a farm in the early twentieth century appears to be associated with favorable longer-term outcomes. Although somewhat uncommon—just 5 percent of our sample—moving to a farm was associated with lower mortality in later life relative to remaining off-farm in rural areas, or moving to a town or city. We observe the worst mortality outcomes for women with nonfarm rural origins who remain in that context in later life, and women who originated in urban areas and moved to smaller towns or nonfarm rural areas.
These results highlight that the rural health disadvantage examined in recent literature (Cosby et al. 2019; James 2014) is not homogeneous. Farm residents—who are certainly rural—have longer lives in general, despite heightened mortality risk from some specific causes including accidents and site-specific cancers from agricultural chemicals. Rural residents who are not resident on farms, whether in earlier or later life, have significantly elevated mortality risk in our cohort of women in Iowa. The educational and health behaviors of the Iowa cohort suggest two, not mutually exclusive, mechanisms for these findings. First, lifetime smoking rates, and continuing to smoke in 1985, were significantly higher for women not living on farms, including those in nonfarm rural settings. It is well known that women in the United States took up smoking in large numbers nearly a generation after men, particularly after World War II (Preston and Wang 2006). Relatively little attention has been paid, however, to the life-course patterns of smoking initiation in American women who reached adulthood between the 1930s and 1960s and who took up smoking at higher rates than cohorts before or since. By contrast, prior studies of the IWHS cohort show relatively small demographic differences in diet and exercise (Shivappa et al. 2016). The similar patterning of smoking behavior and mortality risk with rural-urban migration categories suggests an important area for further research with both the IWHS and other studies of similar cohorts to explain which groups within the age cohort smoked for longer.
Second, the socioeconomic trajectory of women in nonfarm rural areas is more likely to have been declining than for those who stayed at or migrated to a farm or who were living in a city in 1985. Although women with farm origins were less likely to have attended high school, 95 percent of women living off-farm or in an urban area in 1930 attended high school. But conditional on graduating high school, women who stayed off-farm in rural areas or moved to small towns were less likely to attend or complete college. Women with urban origins (in 1930) or destinations (1985 residence) were more likely to complete college than their off-farm rural peers. These educational patterns are consistent with evidence from other studies of a steeper education gradient in women’s health (Ross and Mirowsky 2010).
An important feature of our study is that it focuses on women enrolled in late adulthood and living in a particular place. We can draw parallels to other cohort studies to highlight what we can learn from this structure. Like the Health and Retirement Study (Brandt, Deindl, and Hank 2012) and SHARELIFE (Pakpahan, Hoffmann, and Kröger 2017), the IWHS recruited subjects who had survived to at least fifty-five. What these studies and ours can say about childhood circumstances are conditional on surviving to late adulthood. Unlike the Health Retirement Study or SHARELIFE, however, the IWHS is situated in a particular place. This is not without parallel either, the Utah Population Database is structured in a similar way with a focus on people living in Utah (Smith et al. 2009). Regional datasets are limited in important ways given that interstate migration over a lifetime is common and the population that chooses to remain are self-selected. Although we highlight the similarity of our group in childhood and adulthood to other women in Iowa on observable characteristics, the differences between our cohort (who stayed) and their peers who moved and are missing by construction, are likely to be on unobservable characteristics. People who chose to leave Iowa (or to stay) likely did so with an evaluation of their economic and social prospects. The advantages we find for women who remained on or moved to a farm in Iowa were not broadly shared. Although Iowa remains a heavily agricultural state and our sample has a high proportion of women living on farms relative to the rest of the United States, it is also true that the share of women living on a farm declined from three-fifths to less than one-fifth of the sample. Whatever the ways that farming worked to benefit women in our cohort, it is not a plausible treatment that can be applied to resolve the disadvantages of other groups in rural areas. In short, the selective nature of the IWHS cohort tells us something about the structure of rural advantage and disadvantage.
Coincident with a pattern of health advantage for women with farming connections, we saw a pattern of earlier old-age mortality for women in nonfarm rural areas or small towns. We emphasize that these are empirical and selective associations rather than causal mechanisms. Nevertheless, the selective nature of disadvantage is informative. The women we see in the IWHS in later life are women who remained in Iowa. Less than half of the 1916 to 1930 birth cohort who were born in Iowa were still in Iowa at the 1980 census. Thus, although many of the nonfarm rural or small-town group moved between counties, relative to their cohort peers they did not move far. The disadvantaged group share with women remaining on or moving to farms a pattern of relatively short intercounty moves or persistence in the same county. Yet the two groups differ significantly in social and economic outcomes.
The pattern of disadvantage identified for women in nonfarm rural settings is consistent with the changing geography of economic activity in rural areas in the United States. Mechanization of agricultural work has reduced the numbers of people needed to work a given area of land. In 1930, small towns housed and provisioned farm laborers and small businesses catering to farms. But farm laborers are fewer in 1986 and thus fewer people live in small towns and rural areas that need retail or services. Paving of rural roads, for example, has enabled farmers to access commercial services and retail trade in larger urban centers. Conversely, towns and cities have provided increasing opportunity for socioeconomic advancement with labor markets diverse enough for both members of dual-earner couples to work. Persistence in nonfarm rural areas is associated with fewer economic opportunities. In Iowa after 1985, the decline in the number of nonfarm businesses in rural areas was significant. The structural decline in economic activity during the farm crisis in Iowa in the 1980s has been echoed in other rural settings in the United States in subsequent decades. Despite these structural changes, we do not see strong evidence in our sample of “deaths of despair.” Deaths from suicide, accidents, and alcohol or drug abuse were rare in this cohort. As other scholars note, the rural mortality disadvantage has been concentrated in working-age Americans (James, Cossman, and Wolf 2018), similar to the pattern identified for deaths of despair.
The contrast we identify between favorable outcomes for farm women, and less favorable outcomes for nonfarm rural women point to the challenges in understanding what it means to live in rural America. Both farms and their surrounding areas are rural, and yet the life chances of residents are quite different. Women with connections to capital in farming derive significant health benefits from their status. Despite the hazards of growing up in urban areas before World War II, women with urban origins and later-life residence have been able to take advantage of their human capital. Off the farm, families without capital in farming or a larger market for their human capital face significant social and health disadvantages. These contrasts point to the importance of social status and resources in overcoming some of the challenges of living in contemporary rural America.
FOOTNOTES
↵1. However, Iowa now lags behind the nation in its share of college graduates, 27.7 to 30.9 percent. This proportion is lower than many surrounding states in the West North Central Census Division, including Minnesota (34.8 percent), Nebraska (30.6 percent), and Kansas (32.3 percent). See the authors’ tabulation from 2019 American Community Survey available via IPUMS (Ruggles, Flood, et al. 2021).
↵2. To finance World War I, the Department of the Treasury sold Liberty Bonds to the general public in a series of loan drives. The success of these drives depended greatly on volunteers from civil society organizations (Hilt and Rahn 2020).
↵3. See online appendix.
↵4. Note that in all figures displaying group means we have used 84 percent confidence intervals around the mean, so that non-overlapping confidence intervals can be directly interpreted as having a statistically significant difference at the 5 percent level.
- © 2022 Russell Sage Foundation. Roberts, Evan, Wendy Rahn, and DeAnn Lazovich. 2022. “Life-Course Transitions in Rural Residence and Old-Age Mortality in Iowa, 1930–2014.” RSF: The Russell Sage Foundation Journal of the Social Sciences 8(4): 106–24. DOI: 10.7758/RSF.2022.8.4.05. We thank the participants in the “Growing up in Rural America” workshop, the editors, and three anonymous reviewers for their comments on earlier drafts of the manuscript. We particularly thank Reviewer 2 for constructive engagement with the paper and concrete suggestions for improvement. We thank the University of Minnesota Office of the Vice President for Research for supporting data collection through a Grant in Aid (#23111), and gratefully acknowledge support from the Minnesota Population Center (P2C HD041023) funded through a grant from the Eunice Kennedy Shriver National Institute for Child Health and Human Development. Shannyn Telander and Leah Engelman provided valuable exemplary research assistance with the record linkage. We thank the subjects of the Iowa Women’s Health Study for their participation in many waves of data collection. Direct correspondence to Evan Roberts, at eroberts{at}umn.edu, Department of Sociology, University of Minnesota 909 Social Sciences, 267 19th Ave S, Minneapolis, MN 55455, United States.
Open Access Policy: RSF: The Russell Sage Foundation Journal of the Social Sciences is an open access journal. This article is published under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.