
Abstract
Small primary care practices are critical to advancing Affordable Care Act (ACA) aims, yet their efforts and experiences remain little studied. We examine two strategies derived from ACA population-health provisions—enhanced use of electronic health records (EHRs) and community health worker (CHW)–led peer coaching—for hypertension control in sixteen small practices serving South Asian immigrant communities in New York City. Based on interviews with physicians, staff, and CHWs, we analyze “street-level” dilemmas encountered in implementing the strategies. Findings indicate that the strategies reinforce clinic-community social ties but present distinct challenges for small practices: internal management constraints that impede formal CHW-physician contact, and external incentives linked to EHR tools that, physicians and staff perceive, do not meet immigrant communities’ needs and expectations in medical encounters.
- small primary care practices
- electronic health records
- community health workers
- racial-ethnic minorities
- clinic-community social ties
Although the main thrust of the Affordable Care Act (ACA) has been to increase access to medical care and reduce the number of uninsured individuals nationally, such as through individual and employer mandates for coverage, creation of health insurance marketplaces, and expansion of Medicaid coverage (Levy, Ying, and Bagley 2020), a number of its provisions support population health and disease prevention–oriented reform (Chait and Glied 2018). These provisions reflect the imperative that advancing population health entails not only medical care access, but also investing in local community-based prevention, reworking public health policies and environments to facilitate healthy behavior (Farley 2009; Goodman 2009), and eliminating racial-ethnic and income disparities in health (Bassett 2009).
These provisions are now beginning to be evaluated for their health impacts, given that programs have been operational for a few years (Chait and Glied 2018). Their social effects have been less studied, however, as Andrea Campbell and Lara Shore-Sheppard (2020) note earlier in this issue. In this article, we describe an unexplored consequence of selected initiatives that derive from the provisions. We focus on the ACA’s support for clinical quality-improvement measures that incentivize physicians to enhance use of electronic health record (EHR) technology (Bardach et al. 2013) and the ACA’s recognition of community health workers (CHWs) as part of a multidisciplinary patient-centered approach to health promotion in underserved communities (Islam et al. 2015). Through such strategies, that is, by encouraging use of health information technology (HIT) and extended primary care teams to advance both individualized care and community well-being, the ACA oriented medical practice toward population health goals (Calman et al. 2012; Laiteerapong and Huang 2015; Kruse et al. 2018). By incorporating support for prevention, the ACA “open[ed] opportunities for physicians to integrate population health into primary care practice” (Jacobson and Jazowski 2011, 936).
EHR tools and CHWs introduce new clinical and organizational processes to reach patients from underserved communities. We propose that these processes may not only positively affect population health but also shift relations between clinics and the communities they serve. For instance, EHR tools can provide clinicians with an aggregate profile of their patients as a group. EHR tools that are adapted to monitor and manage disease conditions among minority communities can be used to identify groups at higher risk for disease and facilitate targeted engagement with them. CHWs who provide culturally competent peer coaching to patients in clinics and in patients’ neighborhoods can play a bridging role between the clinic and the community, enabling the clinic to open its doors to the community more widely. EHR tools and CHWs can thus ensure the continuity of care essential for disease management and prevention while also offering support to overcome nonmedical barriers to healthy behavior (such as low health literacy, low English proficiency). They can forge and reinforce the clinic’s responsiveness to a community’s health and social needs. In these ways, EHR and CHW strategies can reposition the clinic as a community-based driver of population health rather than simply an access point for medical care, building social ties between clinic and community in the process.
This study focuses on small primary care practices that serve South Asian immigrant communities in New York City. We examine how the practices implement EHR and CHW strategies as part of a hypertension control project targeted to South Asians from Bangladesh, India, and Pakistan—minority groups that have an especially high burden of cardiovascular disease and unique cultural and linguistic barriers to health behavior change (Yi et al. 2016; Sohal et al. 2015). The project, known as IMPACT (Implementing Million Hearts for Provider and Community Transformation), was funded by the Centers for Disease Control and Prevention (CDC) (Lopez et al. 2017). IMPACT’s aims for cardiovascular health advanced the goals of the Million Hearts initiative, an innovation model of the Center for Medicare and Medicaid Innovation, which falls under the authority of Section 3021 of the ACA. Million Hearts aligns and coordinates public- and private-sector efforts to prevent cardiovascular disease nationally (CMS 2019). We show that IMPACT’s EHR and CHW strategies are not just instrumental for hypertension control, but also build upon and can reinforce social relations between small primary care practices and the immigrant communities they serve. Our findings offer lessons for other aspects of the ACA’s population health-related provisions based on the experience of small practices, which have been largely peripheral in studies of ACA-derived population health innovations.
SMALL PRACTICES AND THE ACA’S POPULATION HEALTH-RELATED INITIATIVES
Small primary care practices are critical to advancing population health among underserved groups. Nationally, practices with five or fewer physicians are responsible for 70 percent of all ambulatory care (that is, outpatient) visits (Rui and Okeyode 2016). More than half of these are made to primary care physicians, the remainder to medical or surgical specialists (Rui and Okeyode 2016). In New York City and New York State overall, practices with four or fewer physicians represent 40 percent of primary care providers and serve residents of some of the poorest neighborhoods in the city with high proportions of immigrant and minority communities (PHIP 2018). Patients from minority groups are more likely to seek care from racially or ethnically similar physicians, and physicians who themselves belong to minority groups are more likely to practice primary care, work in medically underserved areas, and serve non-English-speaking patients (Xierali and Nivet 2018; Marrast et al. 2014; Saha and Shipman 2008).1 Practice characteristics, including size, location, and the race-ethnicity of physicians and patients, are thus consequential for efforts to implement population health strategies and reduce health disparities.
Under the ACA’s population health mandate, questions of how and the extent to which health-care organizations reach out to communities and incorporate community perspectives into their health-care and population health services have become especially salient. However, initiatives that integrate primary care and population health have predominantly involved midsize to large health-care organizations. Questions about clinic-community connections have less commonly been examined in regard to small practices. For instance, the ACA includes directives for nonprofit health-care organizations to conduct community health needs assessments, but these are mostly led by hospitals (Skinner et al. 2018). The ACA also promotes the patient-centered medical home (PCMH) as a model of community-based primary care (Franz and Murphy 2017). PCMH principles include care that is comprehensive, encompasses disease prevention and chronic disease management, and is coordinated across the health-care system and the patient’s community (Ferrante et al. 2010). But official PCMH recognition is higher among larger and better-resourced practices (Scholle et al. 2013; Berry et al. 2013). Small practices face distinct challenges in transforming their teams, workflow, technology, and finances to achieve patient-centered care, yet little is known about successful strategies to implement PCMH principles and other quality-improvement measures in small practices (Berry et al. 2013; PHIP 2018; Scholle et al. 2013; Divney et al. 2019).
Demonstration projects initiated under Section 3021 of the ACA, which test innovative payment and service-delivery models for potential national scale-up (Rocco and Kelly 2020), also tend to overlook the operations of small practices. In some cases, eligibility requirements, competitive application processes, and high practice-transformation expectations can mean lower participation among small practices. In the Comprehensive Primary Care Initiative demonstration, participating practices were selected based on their use of HIT, being recognized for advanced primary care delivery (PCMH status) by accreditation bodies, and previous engagement in practice transformation or improvement activities, among other criteria (Taylor et al. 2015), which are more difficult for small practices to meet. In the federally qualified health center (FQHC) advanced primary care practice (APCP) demonstration, the 400+ participating FQHCs had, on average, six or more primary care physicians per site (Kahn et al. 2015), higher than for small practices. The State Innovation Model (SIM) program funds states to develop and implement plans to improve population health and enhance accountability for quality and cost. With SIM funds, states, payers, and providers have endeavored to form clinic-community collaborations and extend primary care teams to include CHWs, among other efforts. But participation among small, independent providers has been low (RTI International 2019). Providers active in SIM initiatives are likely to have the organizational capacity to forge community partnerships, hire or contract new staff for care-coordination roles, and embed new staff into care teams (RTI International 2019), capacity that is less common among small primary care practices.
Small practices’ role and experiences in implementing population health initiatives and developing clinic-community ties thus remains under-examined. In this study, we analyze social and organizational factors that undergird and in turn are shaped by the implementation of IMPACT’s EHR tools and CHW strategies to improve hypertension control in sixteen small, immigrant-serving primary care practices. IMPACT used health education material developed by the Million Hearts initiative and adapted it culturally and linguistically for South Asian subgroups. Million Hearts was launched in 2012 with the goal of preventing one million heart attacks over five years. It is co-led by the Centers for Medicare and Medicaid Services (CMS) and the CDC (HHS 2013). Million Hearts coordinates and enhances cardiovascular disease prevention activities across agencies and levels of government and the private sector. To this end, it produces resources to guide clinical care and community health education; cultivates collaborative learning among federal, state, local, and private-sector partners; and aligns partners’ activities around national goals for cardiovascular health, bringing together existing and new efforts to improve health across communities (HHS 2013; CMS 2019). Unlike demonstration projects that test model effectiveness for future expansion into national policy (Rocco and Kelly 2020), Million Hearts works mainly to disseminate information and convene partners.
IMPACT integrated EHR tools and CHWs—two interventions that have separately been demonstrated to be effective in meeting Million Hearts goals (HHS 2013). EHRs and CHWs predate the ACA, but the ACA incentivized their integrated use and deployment in connection with population health goals and delivery system reform. That is, the ACA created a comprehensive policy structure—a blueprint for practice and delivery system transformation—that promoted both EHR and CHW interventions through interconnected incentives for value-based, patient-centered care. For instance, the ACA built on key elements from the Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009, such as incentives to encourage meaningful use of EHRs (Gold and McLaughlin 2016). Whereas the HITECH Act delineated infrastructure, standards, and protocols for HIT, the ACA positioned these as foundational aspects of delivery system reform. The importance of HIT to the ACA’s reform objectives is evident in Section 3021/22 innovation models, which presume and incentivize a high level of investment in HIT.
EHRs contribute to achieving population health goals by enhancing care coordination, improving preventive services delivery (such as by encouraging contact and sending reminders to patients), and strengthening the public health infrastructure by enabling electronic exchange of information between primary care practices and public health agencies (disease registries and measurement of population-level quality of care, for example) (Grant and Greene 2012; Laiteerapong and Huang 2015; Kruse et al. 2018). Culturally and linguistically adapted EHR tools enable physicians to adapt medical care for minority communities, contributing to improving population-level health. EHRs are a clinic-based technology, but their widespread adoption, especially in primary care, can address health disparities and achieve population-level impact (Calman et al. 2012). ACA provisions orient primary care to respond to local needs, to provide services that are “culturally appropriate and situationally relevant,” to emphasize prevention and education, and to advance population-level concepts such as community well-being (Franz, Skinner, and Murphy 2016, 835). EHRs facilitate these efforts (Calman et al. 2012).
The ACA also built on rising interest among public agencies, payers, and providers in CHWs’ potential to reduce health disparities and improve population health (Islam et al. 2015; Kangovi, Grande, and Trinh-Shevrin 2015). ACA provisions on CHWs include Section 5313 on promoting a community health workforce and Section 2703 giving states the option to provide health homes for enrollees with chronic conditions in Medicaid. Preventive services furnished under Section 4016 of the ACA can be provided by CHWs as long as the service is recommended by a physician or other licensed practitioner (CMS 2013). The ACA thus promoted CHWs as a part of delivery system reform, supporting their role in primary care teams to improve population health. For the small practices that participated in IMPACT, implementing an integrated EHR and CHW program for hypertension control tailored for their patient population represented a way to prepare for and achieve the high-quality, patient-centered care that payers increasingly incentivize. Our study examines the practices’ implementation of EHR and CHW strategies, offering insights into its social and organizational implications from the perspective of small practices.
CONCEPTUALIZING CLINIC-COMMUNITY SOCIAL TIES
By clinic-community social ties we mean the nature of social relations between clinics and the communities they serve. The term social relations refers to the “multiple ways in which people are connected to one another in society” (Hall and Lamont 2013, 50). People’s actions are social, as Max Weber formulated, when they are oriented to and take account of the behavior of others. People evaluate, interpret, and make sense of their social environment and experiences; this understanding guides social action and hence shapes social relations. Social relations can be observed in the day-to-day actions of and interactions between and among individuals, groups, or organizations. These actions and interactions, which may be informal (left to individual agency) or formalized (reflecting traditions or rules), are always conditioned by cultural, material, and social-structural factors (such as religious beliefs, financial resources, and social hierarchies) (Hall and Lamont 2009).
We focus particularly on social relations that link communities and formal institutions (such as health-care organizations) and that bear on the community’s health, welfare, and well-being (Szreter and Woolcock 2004). Such linking social relations can be instrumental for health; that is, people—clinic or community members—can use and develop these connections to achieve their health-related objectives. But, as discussed, social relations also embody ideas, norms, and subjective understandings that underlie and guide people’s actions, and that reflect material resources and social-structural conditions that constrain and enable actions. Based on this view, we propose that clinic-community social ties comprise actions and interactions involving clinic-related members (physicians, staff, CHWs) and community members, wherein the form, intent, and meaning of actions are all significant features of the social tie. A shift in the social tie implies a change in any of these features.2
Health system changes in recent years, reinforced by the ACA’s community-based approach to population health, call for greater attention to how clinic-community social ties are implicated in primary care provision. For more than three decades, a key feature of health policy reform has been to structure payments, or physician reimbursements, to improve care quality and control costs. Previous health policy research, such as that concerning managed care in the 1990s, focused on how the reforms shifted the structure of financial incentives physicians faced (such as by prioritizing cost-containment), affected physicians’ professional authority (such as through evidence-based medicine and utilization review), and hence shaped their clinical interactions with patients (Mechanic 2004). Research on the social effects of reforms thus analyzed their impact on the physician-patient relationship (Boyer and Lutfey 2010).
By contrast, health policy reform under the ACA foregrounds social ties between clinic and community as a complement to relations between physician and patient. Clinic-community social ties are implicated in ACA support for payment incentives linked to the quality, value, and integrated delivery of health care, which calls for multiprofessional health teams, including CHWs, to address patients’ social needs as a part of patient-centered care (Conrad et al. 2014; Wong et al. 2012; Bitton et al. 2012). ACA-initiated innovation models such as the SIM program expressly support clinic-community collaborations. The SIM program requires states to define population health improvement plans, incorporate new delivery system models into the plans, and specify interventions related to prevention, health equity, and the social determinants of health (Kaiser Family Foundation 2015; Clary 2015). The ACA’s population health-related provisions thus underscore that the organizational features that influence health care—its quality, value, and patient-centeredness—are not only those that determine a physician’s medical treatment decisions and reimbursement incentives. Also crucial are the organization’s social ties to communities and community-serving actors.
While existing clinic-community social ties can facilitate effective health-care delivery, health-care policy can, in turn, drive the development of social ties. As other articles in this issue note (see Courtemanche, Marton, and Yelowitz 2020; Fording and Patton 2020), policy can bring about attitudinal change via the information it offers, message it sends, or ideas it promotes among the public. Our study underscores that policy can also produce social effects, specifically social ties, through those who implement it. In particular, policy provisions that encourage health-care organizations to actively assess and respond to community needs can alter clinic members’ interactions and relations with communities. To examine such a shift in clinic-community social ties, we turn to relevant social scientific theories to conceptualize the implementation of EHR and CHW strategies in terms of, first, the individuals who implement the strategies, and second, the organizational context that conditions individual actions.
Primary Care Physicians, Staff, and CHWs as Frontline Service-Delivery Agents
We conceptualize physicians, staff, and CHWs as frontline service-delivery agents who, in fulfilling their clinical and patient outreach tasks, are also fulfilling policy aims. That is, in their service-delivery roles, they effectively implement the goals that health policy is intended to achieve. They are, in this sense, “street-level bureaucrats,” a term applied to frontline workers charged with implementing policy (Lipsky 2010). By examining workers’ “dilemmas,” or conflicts stemming from tensions between organizational constraints and intervention- and community-related demands, and examining as well their everyday decisions, actions, and responses to dilemmas (Lipsky 2010), studies of street-level bureaucracy explain how policy unfolds on the ground.
An emerging literature applies street-level bureaucracy theory to analyze private “street-level organizations” that are engaged in policy delivery, such as through public-private partnerships or contracts from state agencies (Brodkin 2012, 944). The small private practices in our study are not directly contracted to deliver public policy. However, by striving to fulfill requirements for PCMH certification, demonstrate meaningful use of EHRs, and achieve quality metrics in return for financial incentives, they effectively advance policy goals related to patient-centered, value-based care. Payer organizations play a central role in structuring how and why providers advance such policy goals. For example, payers may set health plan membership requirements that steer providers to incorporate a population health view in their operations. Safety net health plans may induce and support their network practices in this direction, such as by enlisting practices to implement screening interventions targeted to racial-ethnic minorities, making on-site peer counselors and nurses available to clinics, and training physicians on the EHR (ACAP 2014). In participating in these initiatives, physicians, clinic staff, and CHWs effectively operationalize policy aims. The decisions and actions they take are social acts, shaped by their organizational environments and social relations with communities.
We explore the nature of dilemmas that physicians, staff, and CHWs in IMPACT’s small immigrant-serving practices confront, examine how they navigate the dilemmas, and identify the implications that follow for the social effects of selected population health-related initiatives.
External Resource Dependence Among Small Primary Care Practices
We conceptualize primary care practices as organizations embedded in an external environment that can facilitate, undermine, or direct their functioning in particular directions. According to resource dependence theory, organizations depend on resources and support from their external environment to survive and thrive (Pfeffer and Salancik 2003). Examples of resources and support include finances, labor, and information as well as the legal-regulatory apparatus within which they operate. An organization’s performance is thus not a function solely of its internal capacity, but also of its reliance on other organizations, including government entities, which affect the flow of resources toward it. When environments shift, organizations may have to strategically adapt, such as by acting to secure resources and negotiate their external dependencies.
Health system reforms under the ACA, emphasizing value-based payment, population health outcomes, and patient-centered care, represent such a shift in external dependencies for health-care organizations. For example, achieving PCMH recognition can require primary care practices to acquire new staff, train existing staff, and expand patient services, representing dependency on the labor market. Payers may accept a practice into a value-based payment contract only if the practice “serves enough of the health plan’s members to generate results (on cost and quality metrics) that the payer considers statistically valid” (PHIP 2018, 3) reflecting practices’ dependency on payers’ preferences. To participate in value-based payment arrangements, practices have to negotiate and manage the contracting process and develop data and analytic capacity to meet payers’ reporting requirements, potentially incurring dependencies on outside experts in technology and insurance systems (PHIP 2018).
Small primary care practices confront unique challenges in adapting to shifts in their external environment, exemplifying a tenet of resource dependence theory: not all organizations are equally positioned in their relationships and access to resources in their external environment. As Jeffrey Pfeffer and Gerald Salancik (2003, 87) note, “some organizations had more power than others because of the particularities of their interdependence and their location in social space.” Small primary care practices that serve a high proportion of low-income patients may be more vulnerable to shifts in Medicaid payment arrangements than large integrated health-care organizations, such as hospitals, that operate at scale and with greater resources (PHIP 2018). Value-based payment contracts require practices to regularly report to payers on measures of quality, health-care utilization, and cost. Building these new capacities necessitates practices to make “cumulative, sequential, and stepped investments” (PHIP 2018, 3). Small practices’ ability to adopt new technology, reconfigure staff roles and workflow, and employ new staff is limited by their managerial capacity and adds operating costs that can strain their financial viability (Bitton et al. 2012; Scholle et al. 2013; Landon and Normand 2008; PHIP 2018; Berry et al. 2013).
Research applying resource dependence theory in health care has included statistical analysis to examine, for example, how external environments influence physicians’ adoption of HIT (Bramble et al. 2010) and hospitals’ participation in accountable care organizations (Yeager, Zhang, and Diana 2015). In this study, our aim is not to test the theory. Rather, we draw on its insights to suggest how external resources might influence the constraints and opportunities that small practices face and that condition their workings. We thus integrate a conceptualization of clinic-related actors as street-level bureaucrats who confront service-delivery dilemmas and primary care practices as organizations that confront external resource dependencies. The study illuminates organizational processes involved in the implementation of the ACA’s population health-related provisions, specifically through EHR and CHW strategies in small immigrant-serving practices, and their implications for clinic-community social ties.
STUDY SETTING
IMPACT ran from 2014 to 2019 and was led by the New York University Grossman School of Medicine–City University of New York Prevention Research Center. Other project partners were IPRO, a quality-improvement organization, which trains and assists practices to transform to PCMH and maximize their EHR use, and Healthfirst, a not-for-profit managed care organization. Healthfirst is the largest Medicaid managed care plan in the New York City area and works through close provider partnerships and community involvement. IMPACT leveraged Healthfirst’s efforts to implement Million Hearts among a subset of its practices serving South Asian populations in New York City. Healthfirst data indicated that a majority of these members seek care at independent, small South Asian-owned practices.
In IMPACT’s sixteen primary care practices, on average per practice, more than 70 percent of revenue was from Medicaid and more than 75 percent of patients belonged to South Asian subgroups (table 1). Practices were located in Queens, Brooklyn, and the Bronx, in neighborhoods identified as having a high proportion of South Asian residents with limited English proficiency (Kum et al. 2018). Each practice employed, on average, two physicians and two staff (table 1). There were fourteen physicians in all, two of whom ran two practices each. All physicians but one were South Asian. Most medical assistants and office managers were also South Asian. In several practices, office managers and medical assistants were medically trained in their home countries but not qualified to practice medicine in the United States. Their views reflect not only perspectives on everyday clinic operations, but also a close understanding of disease burden, social norms, and obstacles to healthy behavior change among South Asian immigrants.
Characteristics of Primary Care Practices Participating in IMPACT
Among South Asian immigrants, a strong sense of collectivism (individuality subsumed in the interest of group welfare) and an emphasis on self-help and informal help-seeking networks (family, neighbors, friends) are known to influence health-care choices and service use (Bhattacharya 2004; Sohal et al. 2015). IMPACT’s guiding premise was that physicians can effectively serve South Asian communities with clinical decision-support EHR tools tailored for South Asian communities, which CHWs can reinforce through in-language, culturally competent peer coaching for hypertension control.
IMPACT’s EHR tools include registry reports, alerts, and order sets tailored for the South Asian population (Lopez et al. 2017). Registry reports (patient lists generated from the EHR) identify patients with uncontrolled blood pressure readings and patients with a diagnosis of hypertension. The reports enable the clinic to identify patients lost to clinical follow-up and call them to schedule visits. Alerts are pop-ups that function as reminders and a call to action in the EHR; IMPACT designed alerts to prompt physicians to ensure blood pressure measurement and follow-up care for patients with hypertension. Order sets are disease-specific preset prescriptions, laboratory tests, and counseling orders that physicians can easily access as a set in the EHR. IMPACT developed hypertension-specific order sets linked to evidence-based, culturally adapted, and in-language educational materials for South Asians.
CHWs worked with patients from IMPACT practices but were not practice employees. CHWs screened a subset of patients visiting the practices for their eligibility in the six-month-long CHW component. CHWs planned and led five in-language, culturally adapted education sessions on diet, exercise, cardiovascular disease, and stress management at the practices. CHWs also conducted bimonthly individual health coaching to set goals to improve healthy behaviors via phone and in person, and facilitated appointment-keeping and referrals to social services. Of IMPACT’s six CHWs, three were male and three female. All were South Asian.
IMPACT’s cultural and linguistic adaptations were designed to ease barriers that immigrants may confront in understanding health information and self-managing chronic conditions (Acevedo-Garcia et al. 2012). For example, CHWs approached patients with the awareness that gender norms might constrain women from participating in physical exercise or in the intervention altogether. Health education material depicted ethnic foods and anticipated specific modes in which South Asian patients would adopt healthy behavior change (for example, engage in outdoor physical activity in groups or with family members, cook healthy foods within intergenerational households). IMPACT also addressed health-care-seeking norms: immigrants who are unfamiliar with the U.S. health system or have low health literacy are likely to seek care as in their home countries, such as by visiting the doctor for symptomatic treatment, not for preventive care. IMPACT enabled the clinics to actively call patients in for preventive care and follow-up visits. Figure 1 shows connections between clinic and community and the ways IMPACT’s EHR and CHW strategies extend connections.

Extending Clinic-Community Social Ties Through EHR and CHW Strategies
Source: Authors’ illustration.
Note: Clinician icon made by Vectors Market from www.flaticon.com. Other icons made by Freepik from www.flaticon.com.
METHODS
We conducted semi-structured interviews with eleven physicians, sixteen clinic staff (office managers and medical assistants), and all six CHWs to study their experiences with and perspectives on the EHR tools, peer coaching, and interactions with the South Asian community. We also interviewed three senior managers from Healthfirst. We obtained oral consent for interviews. In some cases, interviews were recorded with informants’ consent and transcribed. For many interviews with physicians and clinic staff, we wrote extensive handwritten notes in lieu of recording to maintain a natural conversational flow and sustain rapport. We directly observed clinic workflow at all sites before intervention and surveyed all sixteen sites to assess clinic resources and patient profile. Ten sites were surveyed two years following implementation for another study, which allowed us to note any changes in clinic profile over time.
Thematic analysis of transcribed interviews and field notes was conducted using Atlas.ti. Codes were developed to capture informants’ perspectives on implementing the EHR and CHW components and on South Asian patients and communities. Codes were also developed based on our theorized constructs, namely, demands and challenges of implementing the EHR and CHW components, the practices’ internal organizational features, and their external dependencies as evident from their perspectives and experiences. Three research members separately coded the data. Alongside coding, research team members wrote analytic memos to reflect on emergent themes. Team members met to compare, discuss, recode, and reach agreement on interpretations of coded data and themes. The analysis was thus revised through an iterative process connecting theory and data (Emerson, Fretz, and Shaw 2011). Descriptive statistics of the survey data provide details on resources and staffing at the practices.
FINDINGS
We first present our findings on implementation of the EHR tools, namely registry reports, which involved clinic outreach, followed by alerts and order sets, which were used during clinical encounters. We then relate our findings on CHW implementation, separately reporting on clinic-CHW connections and CHWs’ connections with communities.
Registry Reports
Running registry reports entailed first generating a list of patients with uncontrolled hypertension, and then calling patients on the list to schedule visits. IMPACT advised practices to generate a set of registry reports quarterly or weekly, depending on the measure and information they wished to use for managing their patient panel. Physicians and staff said the reports helped to track patients. One physician noted how some patients “always have problems” and were regularly on the lists. Staff at two practices said the lists were a good form of reference to determine who had been coming into the clinic and who had not. However, physicians and staff reported running the reports with varying frequency and cited internal organizational reasons for their inconsistency. For instance, an office manager at one practice acknowledged that he should be using and consulting the reports more often but said that he felt constrained by time. Staff across various clinics reported that the person trained on the EHR no longer worked there or worked only part time, or that their EHR system had changed and they had to relearn the procedures, or that it had been initially difficult to incorporate a new procedure in their already busy operations. Although all practices had received EHR training for this purpose, several relied on an external technical consultant, supplied by IMPACT, to generate the reports for them on his visits to the practice rather than doing so themselves.
Patient outreach following on from the registry reports was more consistent and uniform across practices. Staff and physicians showed us printouts of the reports—lists with handwritten notes in the margins indicating whether and when patients had been called and whether they had made an appointment to visit the practice. Staff who made the phone calls said that patients were responsive, even when it took some effort. It was “difficult to bring [some patients] in. But patients do come,” one clinic manager explained. A physician pointed to copies of the registry report on her desk and said that when she looked at the numbers of patients with uncontrolled hypertension on the list, the list was shorter than it used to be, fewer patients needed follow-up. She added that if it had been more than six months since the patients’ last visit, then “we must get them [in] through the door . . . we must follow up with them.”
Physicians and staff described challenges in getting patients to return regularly to the clinic and the strategies they used to overcome some of these challenges. For instance, staff at one practice said patients were reluctant to come back in for a visit just for a blood pressure check-up, and to address this, she tried to schedule patients for a visit when they sought prescription refills. For patients not yet on medication, waiting time at the busy practice was another hurdle: patients were deterred by the long waits simply for getting their blood pressure checked, she said. At another practice, a physician said that a challenge was getting patients to make and keep appointments. He estimated that only 30 percent of their Bengali-speaking patients kept appointments, whereas 80 percent of patients from other communities did so. The registry reports, he added, helped them reach patients who otherwise regularly missed appointments. Another physician echoed the tendency among South Asian patients to make unscheduled visits: “If they feel symptoms, then they come in to see the doctor.” The registry reports helped bring patients in, he said. Our site observations affirmed the high proportion of walk-ins, indicating that 20 to 80 percent of visits were walk-ins. At one practice, all visits one afternoon were unscheduled.
The registry reports thus induced a shift in clinic-community social ties by introducing a new form of and purpose for physicians’ and staff’s interactions with patients. The reports enabled physicians and staff to identify and track patients with uncontrolled hypertension, and in turn to view patients in collective rather than individual terms and to work toward proactively and systematically improving group-level outcomes rather than episodically treating individual cases. Outreach following from the reports gave practices a concrete way to counteract what they already knew was the community norm—seeking symptomatic rather than preventive care for chronic conditions—and to influence this health-care-seeking behavior toward ongoing care for hypertension. Yet bringing patients in was only the first part of the problem, according to one office manager, who said that patients were amenable to “come [for a visit] . . . but the outcome is zero, because they are not following what [we] are actually suggesting.” Alerts and order sets, discussed below, were instituted in part to address this problem at the point of care.
Alerts and Order Sets
Physicians and staff broadly reported that alerts and order sets worked as expected, and for some practices were a useful tool in generating discussions with patients on the importance of blood pressure control. One physician noted, for example, that he could show the red status of an EHR alert to the patient and explain that this was due to their uncontrolled hypertension. He said it had a “psychological impact” on patients, prompted them to discuss their symptoms, and made them more receptive to medical advice: “If they don’t see the red alert, they say they feel fine.” Staff at another practice noted that the alerts helped them streamline processes: “Before . . . for one patient, we used to use at least fifteen to twenty minutes just to figure out everything . . . Now it only takes five minutes.” Order sets contained material tailored for South Asian patients, and this was helpful to educate patients, several physicians remarked.
The use of these EHR functions, however, was mixed. Many staff and physicians said that they “just close[d] the link” when the alert window appeared on the screen. One physician said that beyond noting the alert as a visual reminder, they did not use it. Others reported technical problems; staff at one practice said the alert appeared but its follow-on links did not work. A physician said that lately the alerts were not appearing as they should, and wanly commented that working with his EHR system was difficult. Physicians and staff thus struggled with optimally using their EHR systems. Their struggles reflect challenges common to underresourced practices, who are unable to carefully select and tailor their EHR systems and often use systems with known deficiencies in functionality related to PCMH incentives (Cohen et al. 2018; Divney et al. 2019).
Our site observations, conducted before IMPACT implementation, showed limited technological capacity at the practices. One physician had noted that although they had customized templates to document patient progress notes, the staff did not know how to use them. The same physician had said he was “very poor on the counseling codes,” meaning that although he counseled patients, he did not know how to document the counseling in the EHR and hence did not get credit for it. At another practice, the physician used mostly paper-based files and charts to record patients’ health history. When these practices expanded use of EHRs, they required training and time to overcome constraints of capacity and custom.
For instance, reflecting on order sets, one physician observed that “Installing these was not hard. But using them, that is hard.” If he had time to learn the technology, he explained, he could get more information out of it. “There are some easy things that we don’t know,” he said, adding that using the new EHR functions had helped him learn about its capabilities. An office manager at another practice echoed this sentiment. Physicians were “not very used to that template . . . they’re used to their own [ways], the way they used to always [conduct the clinical encounter],” he said, noting that time and workload impeded physicians’ EHR use. He initially used to “remind the physicians every other week that actually we have this and you can use it if you want. But . . . still it’s not 100 percent ... definitely not 100 percent.” One physician said she found order sets cumbersome and that she might refer to the order set to counsel patients, but did not otherwise rely on it for the medical encounter.
Other physicians articulated the problem with order sets not in terms of usability but utility, specifically in terms of addressing the needs of certain South Asian patients—older adults, recent immigrants, or those who were not literate. Physicians noted that the order set contained culturally tailored materials (such as plate planners depicting heart-healthy South Asian meals), which provided useful visuals to guide conversations about diet change, particularly in contrast to most mainstream health education material made available by municipal agencies or campaigns. Yet many also said printed materials were inadequate on their own to change patient behavior. It was more useful to tell patients, one physician remarked: patients were more likely to respond to a doctor’s oral advice. A medical assistant noted that if he gave his elderly Bangladeshi patients a handout, they might simply discard it. Patients needed to hear advice from their doctors, he stressed. He explained that an older Bangladeshi woman who had never exercised was not going to begin now, and even patients who did decide to exercise did not know much about it: he had to educate patients that walking from their home to the grocery store a couple of blocks away did not count as adequate exercise. He said he had previously worked in Bangladesh and treated patients there; now that he was in New York, among people who have immigrated here, he saw the same patterns, the same issues with diet and exercise, with keeping appointments, with understanding prescriptions and the importance of taking medication. Some patients did not understand they had a number of prescribed medications they had to take. He had to ask them to bring in all their medications so he could determine which ones they were taking.
At another practice, an office manager who was trained as a health education counselor expressed that it was not the quantity but the source of the information that mattered for patients’ responsiveness to advice. He contended that patients did not respond as well to “what society tells them” about a healthy lifestyle as they did to advice that came from doctors, religious leaders, or other such figures. The doctor or coach had to “read” the patient and personalize information for the patient, he said.
Existing clinic-community social ties were thus evident in physicians’ and staff’s intimate understanding of their South Asian immigrant patients’ health behavior and responsiveness to medical advice. Especially salient here was the role of verbal advice in the medical encounter. Physicians’ and staff’s perspectives suggested that written health education material, as available in order sets, could complement oral counseling, but was likely to be less effective among older and recent South Asian immigrants. Physicians and staff deemed it important to reinforce this material for certain patients by personalizing advice (such as sorting through medications and clarifying which physical activities counted as adequate exercise) and delivering this advice face-to-face. In this respect, alerts and order sets complemented clinic-community social ties by expanding the ways physicians could educate, advise, and interact with patients. But in physicians’ perspectives, conversational exchange appeared crucial to the interaction.
Our findings also show that the practices’ organizational capacity for adopting EHR technology constrained their use of the alerts and order sets. Underresourced practices that do not have the capacity to purposefully choose and customize their EHRs may not fully reap the benefits of EHR adoption (Divney et al. 2019). Yet, despite espousing some ambivalence about aspects of alerts and order sets, physicians were keen to sustain their EHR capability for all tools mentioned, a point we return to in the discussion.
Clinic-CHW Connections
Physicians and staff uniformly agreed that CHWs were useful for their patients. One physician said that a patient had reported the sessions had improved her (the patient’s) compliance with diet and lifestyle change. Another physician noted that the group sessions enabled patients to talk to each other, to share experiences. Still another viewed the sessions as a feature to draw patients into the clinic and to motivate them to schedule a physician visit the same day, and suggested regular classes in the future so patients could routinely drop in to the practice.
Physicians and staff were sympathetic to the difficulties CHWs faced in reaching out to South Asian communities. Staff at one practice said he recognized that patients did not want to come in solely for an education session if they had no medical reason to visit the doctor. One physician concurred that a key challenge for CHWs was to recruit patients, to “gather the community” for the group classes. Staff at another practice said that CHWs’ mailing letters to recruit patients was not enough: “We have to call them. They won’t respond to [only] a letter. They want to hear it from the doctor.” Direct encouragement from physicians was imperative not only because of their medical authority and patients’ trust in them, but also because of patients’ low literacy. As one CHW explained, older immigrants may read neither English nor their native language: “They speak Punjabi but they don’t read [it].”
CHWs therefore stressed the importance of physicians and staff reinforcing their message by reminding and encouraging patients to participate in classes and health coaching. When asked about the effect of the physician’s involvement, one CHW exclaimed that it made a “big difference!” He had given a physician flyers to be kept in the consultation room, he said, and had told the doctor that, “if you see any hypertensive patients, give [them] this flyer. Tell them to come to this program.” Staff at most practices said they posted flyers. But apart from the practices’ passive advertising of the program, CHWs reported mixed levels of support from physicians. A CHW said that at one practice the physician would “sometimes greet us in the hallway . . . ask us about how it’s going, if we need any help.” The physician questioned and pressed patients to follow the sessions, “and that’s why at that site we’re more successful,” the CHW said, contrasting it with his experience at another practice, which was short-staffed: “They help us, but sometimes, when we ask them, they say, ‘we don’t have time’ or, ‘we’re very busy today.’”
CHWs commonly worked without sustained contact with physicians, but in a few cases were able to approach physicians directly. One CHW, who had worked with some of the physicians on previous projects, acknowledged that high workload and informal organizational processes in the small immigrant-serving practices made physicians seem inaccessible to newer CHWs: “If you go to the clinic . . . whole room is full of people. You can’t even walk in the sitting areas. Packed. They don’t have enough time to give you . . . And because this is not appointment-based, always walk-ins . . . One person finishes, then the next comes, that’s the way they’re doing it. So finding time, meeting with [the doctors], is really hard if you don’t know them.”
Another CHW said he did not contact the physician directly but drew on his relationship with the office staff: “so I call them [and ask] can I talk to the doctor . . . can you let the doctor know [what I need] and [let me know] what should I do?” He also noted that “different doctors have different perspectives.” Some liked to know how their patients were doing, how attendance at the sessions was progressing, and at times would say, “I’m giving you this number, so contact this patient.” But some, the CHW remarked, say instead, “this is [the] intervention, they’ll do their work and I’ll do my work.”
At the same time, some physicians expressed a desire for more communication with CHWs. One physician recounted that a patient had once visited the practice on a CHW’s recommendation, but the CHW had not informed the clinic about the patient’s high blood pressure, and the patient had inadvertently waited his turn as a walk-in visitor. An office manager at another practice observed similarly that “[if] patients are doing well or not, achieving goals or not, [CHWs] should tell us.”
Clinic-CHW connections did emerge informally in several practices through CHWs’ efforts and resourcefulness and the support of staff and physicians, but practices did not develop formal procedures to involve CHWs in teamwork or exchange information about patients. Potential reasons for this include IMPACT’s short-term, hypertension-specific goals, under which CHWs were likely perceived as temporary, external adjunct workers dedicated to a particular health program. Other factors pertain to the practices’ small size (an average of two clinical and two office staff), workload (high number of walk-ins), and informal management processes, typically without structured teamwork as in larger health-care organizations. We explore these challenges in the discussion.
CHWs’ Connections with Communities
CHWs’ narratives about South Asian immigrant communities demonstrated their in-depth, nuanced, and tacit knowledge of the community. This knowledge enabled CHWs to build social relations with community members and to anticipate the reluctance they would encounter. For instance, CHWs described one challenge as the normalization of hypertension. In the “Bangladeshi community, sometimes people feel [high] blood pressure is not a disease,” one CHW explained. CHWs further said that recruiting patients for health education sessions was constrained by the difficult working lives that immigrants led. As one CHW noted of a young man in his mid-twenties who had hypertension, “He was so busy. I understand immigrant people, they are always busy. They’re working around the clock to make their living. . . . [His] father was also our client. He is also hypertensive . . . I explained, ‘You have to take [this] very seriously, my friend, if you want to live long.’” In response, an approach CHWs often took in their counseling was to raise an alarm, to emphasize the dangers of uncontrolled hypertension. This strategy was similar to that of physicians who showed patients the red status of alerts in the EHR to move them to act.
According to CHWs, in their target South Asian communities, many women’s lives revolved around intergenerational households with extended families. One CHW felt that women participants had “large family responsibilities” that distracted them during counseling sessions: “When they come for the session they always think about their home issues.” Social expectations associated with a woman’s age, caregiving roles as mothers and grandmothers, and gender-based power differentials were major hurdles, CHWs said. As another CHW explained of the women,
They cannot go outside by themselves or they don’t know how to speak English, or they don’t want to learn [about health]. . . . And most of the time they don’t have their [own] phone . . . We have to go through their [adult] children or husband or other family member. So we have to convince [the family members] first and then we have to go to the women . . . sometimes [the family members] say, “Oh no, they take care of the babies, or they take care of the home, or they are too weak to go outside, they cannot go by themselves. . . . We know program is good but we don’t want to join.” . . . If the session is a little far from their houses, [the women] don’t want to come. And they make excuses: we might get lost or it’s too far.
Preliminary enrollment data from IMPACT bore out the CHWs’ narratives. Data from one round of enrollment show that of the 328 patients contacted and confirmed as eligible for the program, 111 patients, or one-third, declined to participate. Of those who declined, 14 percent said they were too busy, and for another 14 percent—all women—a spouse or adult child declined on their behalf.
Cultural norms and social expectations influenced not only community members’ participation in the program, but also CHWs’ practical and affective experiences with reaching patients in their communities. When CHWs made home visits, they had to navigate the customary hospitality of South Asian households as they attempted to efficiently deliver goal-oriented health counseling. One CHW said he preferred to meet patients individually in places other than their homes: “I feel like when I go to people’s houses, I put them into problem. You know, making tea . . . our culture, South Asian culture . . . They love to entertain when someone comes [home].” The CHW recounted a time he had visited a patient’s home at 9:30 p.m., after the patient, a limousine driver, got off work. The CHW, worried about being asked to dinner, had to deftly ensure he could leave immediately after the counseling session.
CHWs also keenly experienced the diversity of South Asian immigrant subgroups. All the CHWs were South Asian, but the CHW’s national origin or ethnic or religious identity did not always match that of the patient. For example, Pakistani Muslims and Indian Sikhs from the Punjab region of South Asia may speak the same language but have different cultural and religious norms. One CHW recounted a home visit: “Knocking [on the door] is common. But then how to behave? . . . Taking off shoes is common sense. But besides that? . . . The [patient’s] family was very involved. Everybody was asking questions, coming in, going back and forth. And she didn’t . . . inform us there will be other family members. . . . It took longer, but then we have learned the lesson moving forward. . . . how to deal with it, going into another culture and another religion.”
CHWs concurred that one-on-one counseling benefited patients but found it more practical and effective to engage patients individually outside their homes. For example, one CHW said he had met with patients at Dunkin’ Donuts, in a restaurant, and in his car. “Those we call ‘home visits,’” he said. Another described patients as more attentive away from their homes, such as during group sessions: “It’s the environment . . . participants talk to each other in between or toward the end . . . and then I learn from their conversations. . . . I think participants are more engaged when they come to the clinic, actually.”
Beyond group and one-on-one sessions, CHWs’ support to patients included referrals to public and community services. CHWs considered this an inherent, essential part of the job; it built trust and helped ensure that people returned for health education. One CHW explained: “We help people to get food stamps. We help them to apply for passport . . . to get Bangladeshi passport from [the Consulate]. Then we also help them to apply for housing. . . . They get our trust because we help them with a lot of things. . . . We teach [them how to] take the train, how to go to doctor’s office. . . . Sometimes we go with them to the doctor.”
The CHW recounted that a South Asian patient she had counseled on a previous project had moved elsewhere in New York State and had called the CHW to ask questions about the moving process. Another CHW described how he had helped people apply for health insurance and temporary housing. One CHW noted that many immigrants were either busy or unaware about services, “so they never explored [their options] and when they find out [what is available], they’re really happy.”
Another CHW stressed the vulnerability that immigrants felt and the CHWs’ critical role in responding to individuals’ personal histories as these were linked to their health. She described how her father had arrived in the United States after having worked in a managerial capacity in a bank at home, but his accent and competencies had not seemed adequate for similar work here. He felt as though he was “just starting, growing . . . this is the new country,” she said. The displacement immigrants experienced affected their mental and physical health, she said, adding it was important to “understand their psychology, how they feel. . . . When they have health issues, they feel [that] because they can’t speak English, maybe they can’t [explain] what’s inside, what’s going on, they can’t communicate to the doctor. They have a different kind of pain that [they] can’t explain.”
CHWs thus drew on their understanding of not only the community’s health behavior but also experiences of immigration. CHWs’ work brought patients to the practices outside of physician visits, and CHWs visited patients at home or other neighborhood locations, thus introducing new modes of and purpose for clinic-community interaction and reinforcing social ties. CHWs expanded patients’ access to social and community resources, repositioning the clinic’s role beyond medical care.
DISCUSSION
EHR tools and CHWs reinforced and extended the practices’ social ties to communities in several ways. In generating registry reports, the practices adopted new organizational procedures by which they systematically called patients in for follow-up visits. This situated the practice as a place for patients to go to maintain health, not only episodically resolve symptoms. Order sets, which contained culturally and linguistically adapted resources that physicians could access and offer patients, effectively placed physicians’ existing community knowledge into the health education process via the EHR. CHW-led health education classes positioned clinics as sites for community members to gather, learn, and share experiences about making diet and lifestyle changes. CHWs’ one-on-one counseling bridged clinic-based care and community-based support. At the same time, features of South Asian immigrant communities and the practices’ organizational constraints contributed to service-delivery dilemmas, as we discuss.
Dilemmas of Implementing Population Initiatives in Small Clinics
Physician, staff, and CHW experiences and perspectives suggest that they confronted at least three dilemmas as they sought to improve hypertension control among South Asian communities. One dilemma concerned the intended and practical utility of some of the EHR tools. A second and related dilemma concerned physicians’ interest in maintaining EHR capability despite their mixed views about using EHR tools. A third dilemma concerned CHWs, who could engage and build ties with South Asian immigrant patients but operated with uneven clinic support to extend their outreach.
EHR tools formalized community knowledge but could not codify relational norms.
Physicians generally reported lower use of alerts and order sets than of registry reports. In part, their limited use of particular EHR tools reflected their low capability with EHR technology. It also reflected, however, how physicians and staff viewed their South Asian patients: as communities with low health literacy, who might be stirred to act when shown a red alert about their elevated blood pressure, but required personalized advice to clarify their health knowledge and were not likely to respond solely to written communication. Alerts and order sets could not codify the relational norms, emphasizing a conversational medical encounter, that physicians perceived as important to reach South Asian communities.
Research on physicians’ use of clinical decision-support tools shows that although EHR tools can improve ordering and prescribing of preventive care services, physicians’ use of tools is generally low and not associated with higher patient satisfaction (Bright et al. 2012). PCMH programs in community settings similarly indicate that clinical decision-support tools are only “marginally associated” with physicians’ delivery of preventive care, and that the “relationship-centered aspects of PCMH are more highly correlated with preventive services delivery in community primary care practices than are information technology capabilities” (Ferrante et al. 2010, 109). By emphasizing high-tech rather than high-touch principles, the measurement of patient-centeredness under PCMH guidelines can overlook core attributes of primary care that make a practice substantively relationship centered (Ferrante et al. 2010).
Our findings underscore that if EHR technology is to be an effective foundational aspect of delivery system reform and population health improvement as the ACA stipulates, then it should be informed by an understanding of health care as a social act. Health-care provision in this sense is a product of biomedical interventions, technologies to deliver them, and social relations within which the physician-patient encounter is embedded. IMPACT’s immigrant-serving physicians are caught between being encouraged to use EHR technologies widely and being intimately cognizant of health-care-seeking behavior and preferences among their patients, for whom they deem certain EHR tools possibly ineffective. Alerts and order sets appeared to have less traction with physicians, suggesting that though EHR tools can reinforce clinic-community relations, their relevance depends on the type of tool. Registry reports, which sustain patients’ regular engagement with the clinic, were more salient in this regard than alerts and order sets, which are used during a visit.
Evaluations of ACA-initiated demonstration projects have found that practice transformation entails shifting existing facility culture and procedures, which can be difficult to achieve in the short duration of a pilot project (Rocco and Kelly 2020). Evidence from IMPACT’s small immigrant-serving practices suggests that facility culture—such as physicians’ preference for oral medical advice—may reflect not just the stickiness of entrenched organizational norms but physicians’ ongoing, deliberate, socially attuned choices. Physicians may perceive that some high-tech elements are not only difficult to execute in a compressed timeframe, but also unproductive as a way to reach minority communities.
EHR capability could help meet external incentives even if not always meet community expectations.
Despite physicians’ uncertainty about the usefulness of particular EHR tools, they were positive about building their EHR capability. In part, their interest stemmed from their recognition that they stood to develop and do more with their EHR system. In part, it highlights the practices’ external resource dependence on performance incentives. For instance, the practices received incentives from payers (for example, Healthfirst 2019) predicated on quality metrics that included preventive care and chronic disease management. EHR tools helped the practices achieve these aims. Practices that participated in the New York State PCMH transformation initiative were potentially eligible to receive supplemental payments through state Medicaid programs if they achieved PCMH recognition or its equivalent; EHR use contributed to their achieving this recognition (NYS-DOH 2019; Felland, Lipson, and Heeringa 2018). Under Medicaid incentive programs, in prior years PCMH-certified practices could receive $7.50 per member per month for each Medicaid patient served (PHIP 2018). For the small practices in our study, who had, on average, 70 percent Medicaid patients, such incentive programs represented significant sources of technical assistance, training, and supplemental revenue linked to their developing and meaningfully using their EHR system. The incentives made up part of the practices’ external dependence. Physicians’ narratives suggest that their motivation to develop EHR systems lay as much in the EHR tools’ potential to improve patient engagement as in the critical external incentives linked to the tools. Researchers note that initiatives that certify practices as PCMH—EHRs, staff skills, and teamwork, among others (Kieber-Emmons and Miller 2017)—may not all enable practices to substantively respond to community needs (Franz and Murphy 2017). One study, conducted among primary care innovators, found that the decision to pursue PCMH certification was, “in many cases, based on financial incentives and not necessarily on a belief that the recognition would result in higher quality of care” (Hahn et al. 2014, 313).
The small practices in our study made EHR system changes that enabled some to achieve PCMH recognition (Lopez et al. 2019). But for physicians and staff, truly engaging their South Asian immigrant patients entailed acknowledging community preferences and building on a fundamental understanding that people’s personal and collective beliefs and experiences shaped how they made sense of health and illness (Franz and Murphy 2017). This understanding drove how physicians listened and responded to patients as well as which EHR tools they used and how. Their use of “more flexible, less formal strategies” and relationship-centered care is important to consider in assessing factors that underlie the effectiveness of population health-related efforts (Berry et al. 2013, 585; Ferrante et al. 2010).
These lessons bear on the interpretation of evaluations of ACA demonstration projects. Evaluations show that isolating the effects of an intervention can be difficult in a complex external policy environment (Rocco and Kelly 2020). Our findings emphasize that intervention effectiveness is also shaped by the complexity of practices’ internal organizational parameters. IMPACT’s participating practices may show improved hypertension control metrics, but this may not follow solely or directly from their adoption of EHR tools. Instead, it would depend on the practices’ capacity to absorb new EHR strategies into existing relationship-based care processes, to not only adopt but also flexibly adapt EHR systems to meet incentives without compromising patients’ preferences. The findings therefore also highlight how external social environments—in addition to external policy environments—can influence implementation. In IMPACT’s immigrant-serving practices, community preferences and needs, alongside internal EHR capacity and external EHR-linked incentives, together guided the practices’ selective use of EHR tools to improve hypertension control.
CHWs built social ties in communities but were not formally involved within practice workflow.
As much as CHWs could build social ties with patients and link patients to the practices, CHWs’ connections with the practices varied. The practices’ organizational constraints—few staff, high proportion of walk-in visits, and informal workflow—coupled with IMPACT’s time-bound, disease-specific program likely contributed to CHWs’ experiences in this respect. But the CHWs’ uneven involvement in the practices may also reflect a physician-centric mindset in small practices (Nutting, Crabtree, and McDaniel 2012). In small practices, the physician often has a major financial stake and holds clinical authority, and societal roles and conventions can further reinforce the power of physicians over other clinical and nonclinical staff. The practice may “revolve primarily around physicians’ schedules, approaches to practice, and preferences for use of office systems” (Nutting, Crabtree, and McDaniel 2012, 2418). It may neglect the perspectives of ancillary health workers such as CHWs and fail to leverage their contributions. Transforming the practice toward patient-centered, community-based care therefore requires not only making CHWs available to patients, but also ensuring that CHWs are supported by the primary care team. This is a challenge that CHW programs widely confront. Despite growing evidence of CHWs’ potential to improve population health, guidance on programmatic details to integrate CHWs into primary care is limited (Rogers et al. 2018; Kangovi, Grande, and Trinh-Shevrin 2015). Evaluations of the ACA-initiated SIM program have identified CHW workforce shortages as a significant barrier to achieve population health objectives (RTI International 2019). For small practices, a further challenge will be to incorporate CHWs into their teams.
Implications
Lessons from IMPACT’s EHR and CHW strategies are relevant to other aspects of the ACA’s population health-related provisions, discussed here alongside the three categories identified by Nadia Chait and Sherry Glied (2018): provisions to expand government capacity through public programs, structures, and funds for population health; increase access to clinical preventive services; and incentivize prevention in the private sector.
An example from the first category is the SIM program, under which states receive funds to integrate population health improvement strategies, community-based services, and health-care delivery systems for all populations. Participation among small, independent practices has so far been low in SIM programs (RTI International 2019). Our findings suggest that small practices are uniquely positioned to integrate population health activities into their ongoing services, specifically with the aid of CHWs. Small minority-serving practices are likely to already enjoy informal social ties with the communities they serve, enabling primary care teams to readily apprehend community members’ social needs. Small practices may not be able to or desire to invest in establishing formal community partnerships to connect patients to social services, and in this respect CHWs play an important role as mediators between health and social services, between clinic- and community-based resources. CHWs can assist low-income patients with health insurance enrollment, ensuring continuity of coverage despite restrictive policy changes such as Medicaid work requirements that threaten to undo the ACA’s transformation of Medicaid as a program that serves all, not just the “deserving poor” (see Levy, Ying, and Bagley 2020; Fording and Patton 2020). Our study cautions, however, that small practices’ managerial limitations and physician-centric operations can impede CHW integration into primary care teams. Overcoming this challenge will entail supporting small practices to tailor clinic workflow and teamwork to accommodate CHWs, and training CHWs to support the needs of small practices.
The ACA expanded access to preventive care by eliminating cost-sharing for preventive services and expanding coverage for insurance that included preventive care. The impact of this strategy on use of preventive services has been mixed (Chait and Glied 2018). For instance, the use of one new service, the annual wellness visit (AWV) for Medicare beneficiaries, has been low (Jensen et al. 2015), especially among underserved populations (Ganguli et al. 2018). Whereas practice characteristics are one factor contributing to variation in AWV provision and use (Ganguli et al. 2018), our study suggests how social factors may diminish uptake of preventive services among minority communities: barriers to uptake may include health-care-seeking norms tied to cultural beliefs, health literacy, and home-country experiences. Among IMPACT’s South Asian immigrant communities, walk-in visits for episodic, symptomatic treatment were the norm, contrary to the regular visits essential for disease management and preventive care. EHR-based registry reports helped counteract this norm by enabling practices to generate patient lists and actively call patients to make and keep appointments. CHWs helped through conducting health education and enhancing self-efficacy around preventive care. Alongside policies to expand access to preventive services, promoting uptake among underserved populations would require strategies to address the social factors that shape how people seek care and self-manage health behavior. Carrie Fry, Thomas McGuire, and Richard Frank (2020) point to another example: social factors can thwart uptake of health services among justice-involved individuals, which can diminish social spillover effects, such as lower rates of recidivism, that potentially follow from the ACA’s Medicaid expansion. Studies show that CHWs who are themselves formerly incarcerated can help former inmates apply for Medicaid and access preventive care as part of community reentry (Fox, Anderson, Bartlett, Valverde, MacDonald, et al. 2014). Yet unstable housing and employment can constrain former inmates’ retention in care for hypertension, diabetes, and opioid dependence, suggesting the need for supportive services alongside access to health care (Fox, Anderson, Bartlett, Valverde, Starrels, et al. 2014).
Finally, ACA initiatives include performance incentives targeted to states, employers, providers, and patients to improve health. For instance, accountable care organizations (ACOs) receive financial incentives from payers to contain costs and improve quality of care, particularly for patients with chronic illnesses. Although this framework prompts ACOs to apply a population perspective to medical care, impacting population health requires not only revising medical care but also addressing the social determinants of health, which is not ACOs’ core mandate or competency (Casalino et al. 2015). A promising solution is for ACOs to partner with community-based organizations and potentially improve the health of populations within their geographic reach, not only their “attributed” patients (Casalino et al. 2015). Yet such partnerships may be difficult to develop for ACOs composed solely of networks of individual physician or small group practices, who commonly have limited resources and focus on a few selected priorities (Lemaire and Singer 2018). Our findings suggest that CHWs can enable small practices to connect patients to social services, position the clinic as a site for peer-based group health education and support, and reach beyond its “attributed” patients to activate patients’ social networks (even if not the clinic’s geographic area). Small practices can serve as nodes in minority-community networks, which are key structures through which to address health disparities and improve population health.3
Our study identifies the dilemmas small immigrant-serving practices confront in implementing EHR and CHW strategies. It also demonstrates that the strategies can build social ties between small practices and underserved populations, enabling their greater inclusion in population health innovations.
FOOTNOTES
↵1. Minority groups who are underrepresented in the U.S. physician pool compared to their proportions in the U.S. population are black, Hispanic, and Native American–Alaska Native–Native Hawaiian or Pacific Islanders. As Imam Xierali and Mark Nivet (2018) note, although the Asian group is not in this list, many studies show important subgroup differences that are masked when Asians are aggregated as a single group (see, for example, Islam et al. 2010).
↵2. Our definition of clinic-community social ties differs from the term clinical-community linkage used in the health services literature, where the linkage refers to collaborations between health-care organizations, public health agencies, and community organizations (Porterfield et al. 2012).
↵3. We witness the potential for this role in the COVID-19 outbreak, which has greatly impacted immigrant communities in New York City. The immigrant-serving primary care practices in our study have been directly affected as well. Most of these small practices do not have the infrastructure to readily support telehealth efforts, though physicians are continuing to provide care via phone. The practices are also playing an important role in disseminating culturally tailored information for patients.
- © 2020 Russell Sage Foundation. Gore, Radhika, Ritu Dhar, Sadia Mohaimin, Priscilla M. Lopez, Anna A. Divney, Jennifer M. Zanowiak, Lorna E. Thorpe, and Nadia Islam. 2020. “Changing Clinic-Community Social Ties in Immigrant-Serving Primary Care Practices in New York City: Social and Organizational Implications of the Affordable Care Act’s Population-Health-Related Provisions.” RSF: The Russell Sage Foundation Journal of the Social Sciences 6(2): 264–88. DOI: 10.7758/RSF.2020.6.2.12. We are grateful to all the physicians, clinic staff, and community health workers who shared their experiences with us. This study is supported by the National Institutes of Health National Institute on Minority Health and Health Disparities Grant U54MD000538 and Centers for Disease Control and Prevention Grant U48DP005008. NIs time is partially supported by National Institutes of Health National Institute of Diabetes and Digestive and Kidney Diseases Grant R01DK11048, Grant R18DK110740, and Grant P30 DK111022; and National Institutes of Health National Center for Advancing Translational Science Grant UL1TR001445. The views expressed are those of the authors and do not necessarily represent the official position of the funding organizations. Direct correspondence to: Radhika Gore at radhika.gore{at}nyulangone.org, NYU Grossman School of Medicine, Department of Population Health, 180 Madison Ave., #9-44A, New York, NY 10016; Ritu Dhar at rdhar4{at}jh.edu, 42-12 50th Ave., Woodside, NY 11377; Sadia Mohaimin at sadia.mohaimin{at}nyulangone.org, NYU Grossman School of Medicine, Department of Population Health, 180 Madison Ave., #8–35A, New York, NY 10016; Priscilla M. Lopez at priscilla.lopez{at}nyulangone.org, NYU Grossman School of Medicine, Department of Population Health, 550 First Ave., New York, NY 10016; Anna A. Divney at anna.divney{at}sph.cuny.edu, CUNY School of Public Health, 55 W. 125th St., New York, NY, 10027; Jennifer M. Zanowiak at jennifer.zanowiak{at}nyulangone.org, NYU Grossman School of Medicine, Department of Population Health, 550 First Ave., New York, NY 10016; Lorna E. Thorpe at lorna.thorpe{at}nyulangone.org, NYU Grossman School of Medicine, Department of Population Health, 550 First Ave., New York, NY 10016; and Nadia Islam at nadia.islam{at}nyulangone.org, NYU Grossman School of Medicine, Department of Population Health, 550 First Ave., New York, NY 10016.
Open Access Policy: RSF: The Russell Sage Foundation Journal of the Social Sciences is an open access journal. This article is published under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.
REFERENCES
In this issue





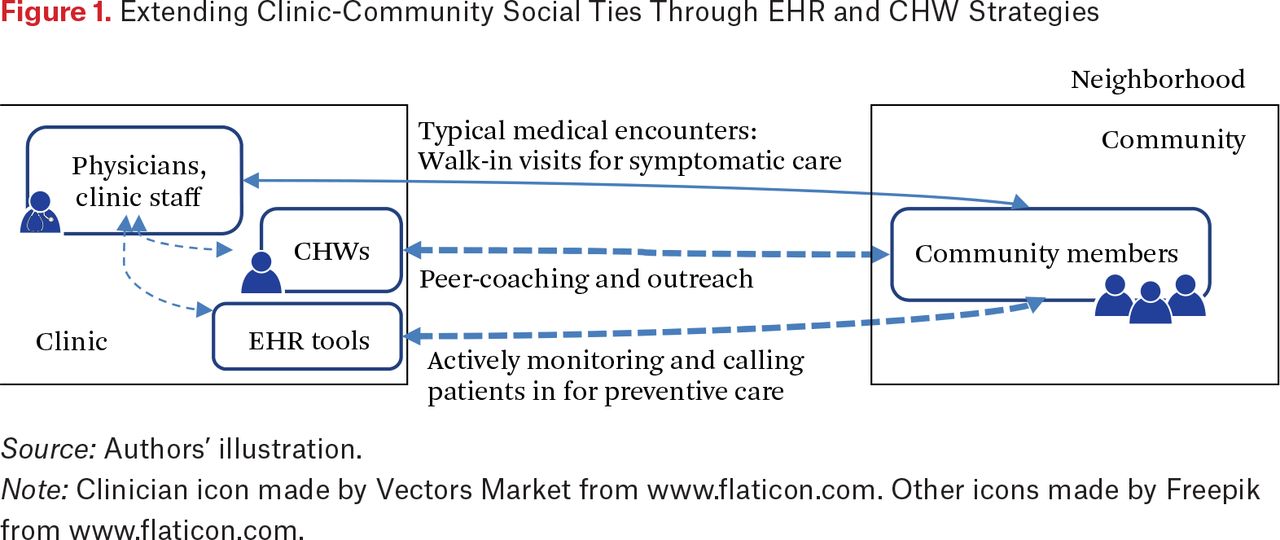{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.