
Abstract
Overseas recruitment has become a common strategy in filling nurse shortages within U.S. health institutions, sparking the proliferation of nursing programs in the Philippines. Export-oriented education exacerbates a mismatch, however, between available jobs (in both the Philippines and the United States) and the number of nursing graduates, thus increasing joblessness and underemployment among Filipino youth. Pursing higher education as a means to migrate also puts Filipino students at risk of getting caught in a migration trap, where prospective migrants obtain credentials for overseas work yet cannot leave when labor demands or immigration policies change. Such problems highlight the complicated impact of immigrant labor niches in places like the United States on developing nations, beyond the brain drain narratives that dominate academic and policy discussions.
As policymakers highlight the growing health care demands of the aging populations of developed nations, foreign nurse recruitment has become the fastest and most common strategy to fill local manpower needs (Brush and Berger 2002; Rother and Lavizzo-Mourey 2009). With scholars estimating a shortage in the United States as severe as 1 million registered nurses by 2020, the United States has emerged among receiving countries as the most active recruiter (Buchan 2006; Keuhn 2007). This demand has created an immigrant labor niche within the American health care system: foreign nurses now fill positions in large urban hospitals as well as in a growing number of rural hospitals and nursing homes (Brush 2008). To date, the largest group of foreign-born nurses comes from the Philippines, a country whose colonial ties with the United States have facilitated nurse migration for more than a century (Brush 2010; Choy 2003).
Scholars have raised concerns about the impact of such migration flows on nurse migrants’ countries of origin, given that the U.S. health care system, which employs the largest professional nurse workforce of any country in the world, exerts “a strong pull on global nurse resources” (Aiken 2007, 1300). Policy discussions also warn of the disastrous implications of “brain drain”—the exodus of trained nurses from poorer nations, which need them the most (Brush 2010; Lorenzo et al. 2007). Yet these problems, while important, do not completely capture how U.S. nursing shortages affect migrant nurses’ home countries.
The brain drain narrative depicts emigration as a pressing issue in many developing nations, but it fails to recognize that a growing number of migrant-sending countries now regard emigration as an economic strategy and train workers specifically for overseas markets in order to maximize future monetary remittances (Cabanda 2015; Rodriguez 2010). Studies have shown that U.S. hospitals’ aggressive recruitment of foreign nurses has sparked the proliferation and expansion of nursing programs in the Philippines; the country’s mostly private colleges and universities are now eager to offer aspiring migrants the chance to take advantage of overseas opportunities (Masselink and Lee 2010; Ortiga 2014). The promise of immigrant success in the United States has also encouraged Filipino families to invest in higher education as a means to migration and created a widespread demand for nursing degrees (Asis and Batistella 2013; Ortiga 2017). International policymakers have largely praised such efforts as an effective “supply response” to global demands and a valid alternative to previous government efforts to prevent nurses from leaving the country (Tan 2009, 8).
This article challenges such celebratory notions of export-oriented education by discussing how attempts to educate aspiring migrants to fill overseas labor demands actually exacerbates the problems of deskilling, youth unemployment, and a growing mismatch between postsecondary education and available jobs within the local labor market. Drawing on two years of ethnographic research within Philippine nursing schools, I argue that as Filipino aspiring migrants educate themselves to fill the U.S. nursing labor niche, they also risk getting caught in two types of traps. The first is the migration trap (Jimenez-David 2008): aspiring migrants obtain specific credentials in the hope of working overseas, yet are unable to leave when labor demands or immigration requirements change. In the context of the most recent U.S. nursing shortage, a backlog of immigrant visa applications in the mid-2000s severely curtailed the outflow of Filipino nurses to the United States (Acacio 2011), and the financial crisis in 2008 reduced migrant nurse hires around the world (International Centre on Nurse Migration 2012). Lacking public funds, Philippine hospitals could not offer permanent positions to the staggering number of nursing graduates within the country, leaving many unemployed and unable to obtain the work experience needed for jobs in alternative destinations like Japan and Singapore. Filipino nursing graduates caught in this situation then find themselves in an opportunity trap (Brown 2003): the never-ending need to collect credentials in order to secure a positional advantage in the job market.
The struggles of Filipino nursing graduates caught in these two traps show that however much the continuous need for foreign nurses benefits migrants and the U.S. hospitals in need of their labor, the impact of such immigrant niches on migrant-sending countries is far more complicated. Even as researchers predict a global demand for nurse labor, aspiring migrants grapple with the loss of time and money in an effort to remain “employable” for jobs they have yet to obtain. Rather than brain drain, I argue, the U.S. migrant nurse labor niche is more likely to lead to a problem of brain waste as qualified nursing graduates find themselves in industries and jobs that have little need for their skills.
THE U.S. NURSING LABOR NICHE
For the past fifty years, a cyclical demand for registered nurses (RNs) within the American health care system has led to inflows of foreign-educated nurses into the United States (Glaessel-Brown 1998; Goodin 2003). Such inflows have come in fits and starts, largely defined by massive structural changes within U.S. health care institutions and policy responses seeking to address the impact of these shifts on American health professionals.
Nurse shortages in the 1980s were attributed to hospital expansions and changes in the Medicare payment system that increased nurse-to-patient ratios. Foreign nurses played a significant role in filling this need until the recession of the early 1990s, when hospitals offered higher salaries to entice more Americans to enter the nursing profession (Glaessel-Brown 1998; Gordon 2005). The recruitment of foreign nurses increased again toward the turn of the century as American nurses became disillusioned with the emergence of managed care—a set of structural changes designed to make hospitals operate in line with a corporate model of efficiency and financial viability (Aiken 2007). Already faced with heavier workloads and more administrative duties, American nurses also encountered higher risks of retrenchment, given the entry of more “unlicensed assistive personnel,” such as nurse’s aides and licensed practical nurses (LPNs), who took on some of nurses’ work (such as changing beds and turning patients). Hospital administrators justified this change as a way to decrease the number of nurses needed on the hospital floor, yet they still expected nurses to take on the extra work of monitoring nurse’s aides (Gordon 2005). When these conditions led to another exodus of nurses from U.S. hospitals, the most recent wave of recruitment for nurse labor overseas began. According to researchers, one of the largest inflows of foreign nurses occurred during this particular period: more than 50,000 migrant nurses entered the United States from 2000 to 2006 (Acacio 2011).
Nursing salaries increased again in the mid-2000s, sparking local interest in nursing programs and encouraging former nurses to return to the workforce (Rother and Lavizzo-Mourey 2009). At the same time, the financial crisis of 2008 led to the scaling back of migrant nurse recruitment in most destination countries, like the United States, the United Kingdom, and Canada (Buchan, O’May, and Dussault 2013; International Centre on Nurse Migration 2012). Some scholars argue that these changes signaled a temporary reprieve from the nursing shortage (Buerhaus, Auerbach, and Staige 2009), while others warn that the U.S. nursing labor deficit is far from over and that foreign recruitment will eventually resume and intensify in the next decade (Cortés and Pan 2014; Kingma 2008).
In seeking to understand the pervasive nursing shortages in the United States, scholars have pointed to the inability of U.S. nursing programs to train a sufficient pool of registered nurses for local hospitals. The majority of U.S.-educated nurses possess a three-year associate degree obtained from a community college, while roughly one-third hold a four-year baccalaureate degree from a college or university. In recent years, nursing schools have offered an eighteen-month “accelerated program” for applicants who already have a bachelor’s degree (Ellenbecker 2010). Despite these different pathways to a nursing credential, U.S. colleges and universities continue to admit only limited numbers of students owing to the lack of qualified nursing faculty (Aiken, Cheung, and Olds 2009; Gordon 2005; Rich and Nugent 2010). Nurses who hold an associate degree are less likely to pursue graduate studies and take on a faculty position, and more likely to take longer when they do. Thus, recruiting foreign nurses continues to be the quickest way to address nursing needs (Buchan 2006; Rother and Lavizzo-Mourey 2009).
Establishing the Labor Niche
Nurse migrants have moved across U.S. borders in a variety of ways, taking advantage of education and training opportunities in the United States or, in the case of the Philippines, previous colonial ties (Brush 2010; Choy 2003; George 2005). What differentiates post-1965 nurse migration is the emergence of brokers: private agencies that facilitate the entry of foreign nurses into local hospitals (Acacio 2011; Aiken 2007; Kingma 2006). Agency representatives take on the work of advertising open positions in source countries like the Philippines and navigating the bureaucratic process of preparing foreign nurses’ paperwork for emigration (Guevarra 2010; Kingma 2008; International Council of Nurses 2006).
Contemporary nurse migration has also seen the emergence of different immigration policies to hasten the entry of nurses into the United States. Unlike other recruiting countries like Japan, the United States did not establish bilateral ties with source countries to facilitate the entry of nurses. However, U.S. officials introduced visa categories that would ease the entry of foreign-educated nurses (Kingma 2007). In the 1980s, U.S. lawmakers established the H-1A visa, a specific category to admit foreign-educated nurses. Subsequently, the Immigration Nursing Relief Act of 1989 enabled foreign nurses with H-1A visas to apply for permanent residence after three years as a registered nurse. This act was allowed to lapse in 1995, when the nursing shortage was perceived as having ended (Glaessel-Brown 1998). During the most recent shortage, foreign nurses entered the United States through the EB-3 visa program; this permanent immigrant visa is reserved for applicants who work in preferred occupations or professions. The United States granted more than 50,000 EB-3 visas to health professionals and their families from 1999 to 2007 (Acacio 2011). The issuance of such visas slowed after the recession in 2008, thereby stemming the flow of migrant nurses into the United States.
Despite foreign nurses receiving special considerations in U.S. immigration policy, American requirements for the entry of migrant nurses are the most stringent among receiving countries. Applicants must pass an English proficiency test, a review of credentials, and the National Council Licensure Examination for Registered Nurses (NCLEX-RN). In fact, foreign nurses were more likely than their local counterparts to possess a bachelor’s degree and to have more work experience (Polsky et al. 2007). Patricia Cortés and Jessica Pan (2015) argue that there is a strong positive selection among Filipino migrant nurses in particular, given that those who make it through this process are likely to come from more highly educated families and possess more social capital. As of 2010, 8 percent of the U.S. nursing labor force was made up of foreign nurses (Cortés and Pan 2015). Filipino nurses are the largest group of foreign-born nurses in the United States, with other groups originating from the Caribbean and Latin America.
The next section illustrates how institutions within foreign nurses’ countries of origin have also sought to take advantage of nurse shortages in the United States, eventually exploiting the nursing labor niche as a lucrative source of profit. Focusing on the Philippines, I discuss the role of private colleges and universities and its impact on aspiring migrants and their families.
EDUCATING FOR EXPORT: THE PHILIPPINE MODEL
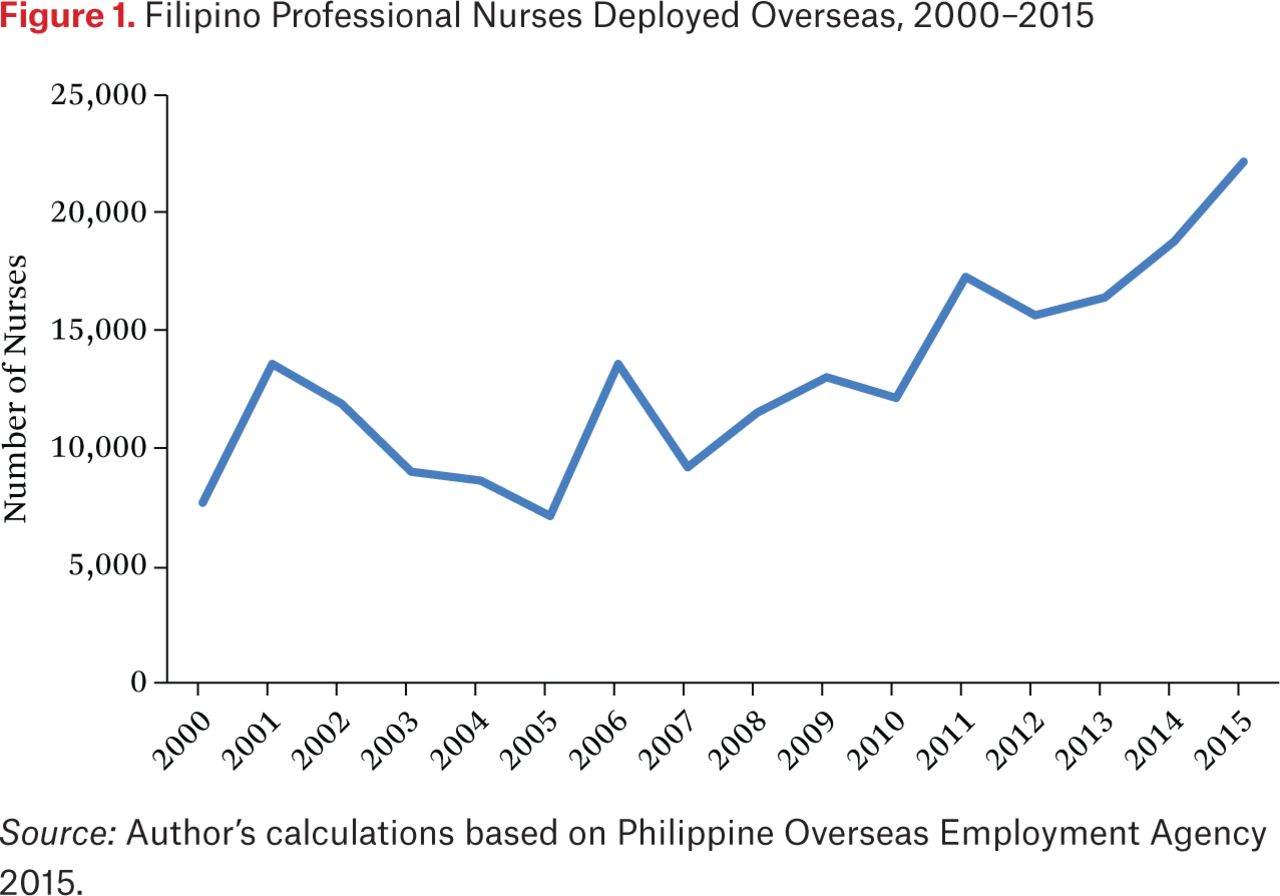
As one of the largest migrant-sending countries in the world, the Philippines has been well known for its response to overseas labor demands, with state-run institutions playing a key role in certifying migrants’ exit papers and qualifications, ensuring their safety, and brokering their labor to potential employers (Goss and Lindquist 1995; Rodriguez 2008, 2010).1 In the case of nursing, the Philippine state promoted Filipino nurses as an ideal source of labor to address global nursing shortages, and government-regulated agencies marketed Filipino women’s inherent ability to do care work (Guevarra 2010).2 These efforts have resulted in a steady increase over the years in the number of professional nurses deployed overseas, and Filipino nurses now work in a wide range of countries, including the United States (see figure 1).
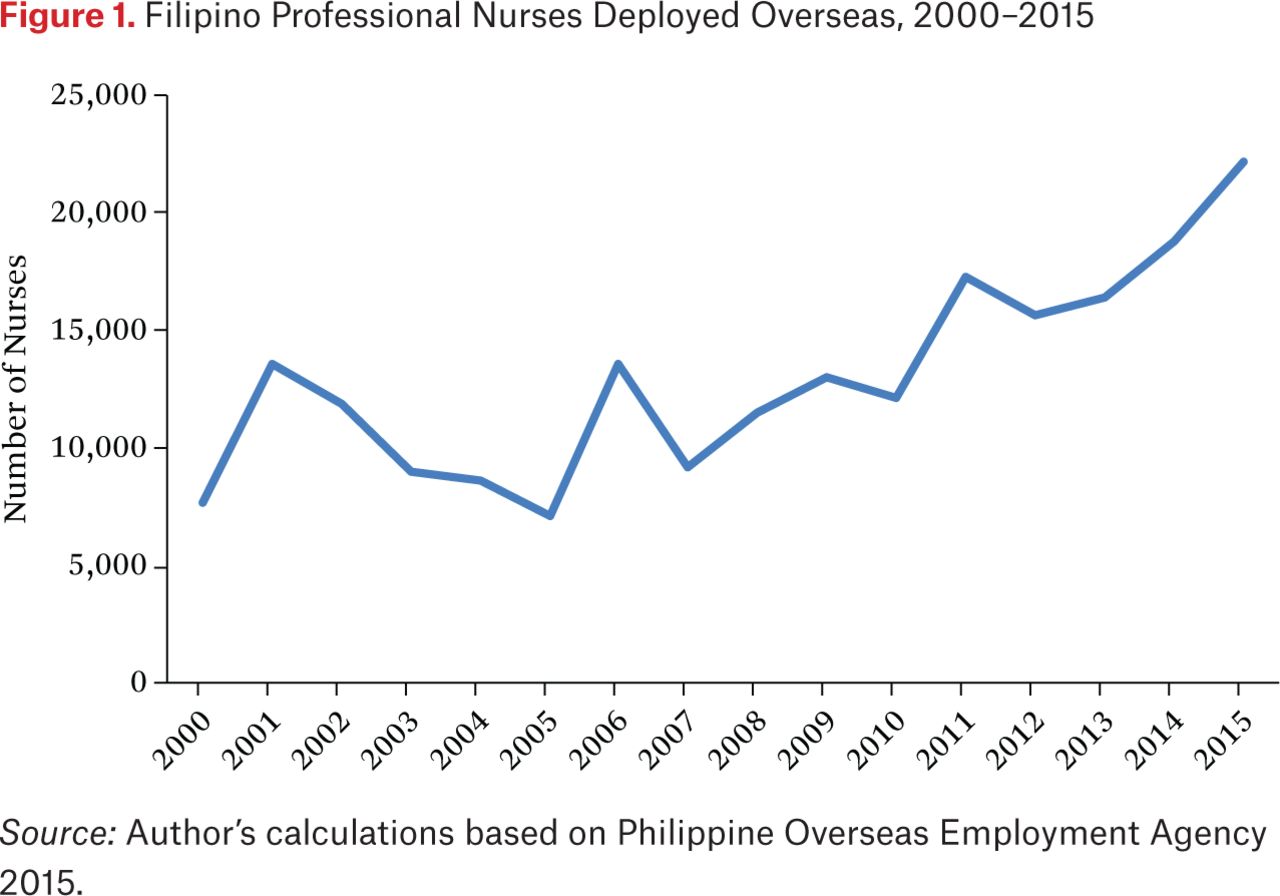
Filipino Professional Nurses Deployed Overseas, 2000–2015
Although given less attention in the migration literature, the growth of commercial industries catering to Filipino nurse migration came with the expansion of nursing programs within Philippine colleges and universities—all eager to produce the nursing graduates their U.S. counterparts were unable to provide. Corporations and family-owned businesses operated the majority of these schools and relied completely on student tuition for profit. Although Philippine media reports highlighted the dubious operations of “fly-by-night” nursing schools (Bagaoisan and Ching 2009; Uy 2008), most private colleges and universities actually complied with standards set by the Philippine Commission on Higher Education (CHED) and were state-recognized institutions.3
Research studies on migration and development have tended to highlight the negative impact of out-migration on educational attainment within sending communities. Although overseas remittances allow migrant households to pay for tuition and school supplies, such benefits are supposedly outweighed by the costs of absent parents and increasing household responsibilities (Creighton, Park, and Teruel 2009; McKenzie and Rapoport 2011; Nobles 2011). In contrast, the Philippines has emerged as a rare “success” story: the prevalence of migration actually leads to better school attendance and increased college enrollment (Yang 2008). The surges of demand and decline in enrollment in Philippine nursing schools have been in line with the cyclical nature of nursing shortages in the United States (Choy 2003). The most recent wave of foreign nurse recruitment to the United States sparked the largest demand for nursing degrees, which peaked at 450,000 new nursing students in 2005 (Ortiga 2014).
Although the Philippine state brokers Filipino nurse labor to many destination countries, the United States remains the students’ ideal destination—a preference strongly informed by the country’s history as a former American colony, but also reinforced by the promise of higher wages and the best possibility of permanent settlement, as compared to other receiving nations like Japan and Saudi Arabia (Buchan 2006). Thus, Filipino families invest in nursing education with the hope that their children will eventually be able to work in the United States and send remittances home.
Until the mid-2000s, Philippine state officials celebrated the expansion of nursing education as an opportunity for both aspiring migrants and the Philippines as a whole. On the one hand, nursing shortages in the United States encouraged aspiring migrants to work toward obtaining higher education, which both policymakers and migration scholars associate with immigrants’ likelihood of success. Studies have shown that the better social networks and resources of highly educated migrants make it easier for them to be economically incorporated into their host society (Csedo 2008; Menjivar 2010; Portes, Fernandez-Kelly, and Haller 2005).
On a broader scale, the rise of Philippine nursing schools reflects an increasingly popular strategy of educating migrants for “export”: migrant-sending countries create “surpluses of certain categories of the highly skilled” on the assumption that these individuals will find lucrative positions overseas and eventually contribute to the development of their home communities (De Haas 2005, 1272; Ortiga 2017). Individuals with higher skill levels also incur lower migration costs, thus decreasing the risk of being exploited or abused (Martin 2012). As such, Philippine state officials have tended to regard skilled professionals like nurses as “ideal migrants” because they are less likely to need protections from the state (see Rodriguez and Schwenken 2013).
Such positive interpretations of the Philippines nursing education boom have faced opposition from nursing activists and academics, who question what the outflow of Filipino nurses has meant for local institutions and health care delivery. Researchers have cautioned government agencies on the problematic implications of brain drain: the loss of valuable labor in Philippine hospitals (Buchan, Kingma, and Lorenzo 2005; Lorenzo et al. 2007). The policy analyst Nicola Yeates (2009, 2010) warns that while nursing schools could produce new graduates to replace those who leave, nurse migration to the United States still leaves Philippine hospitals with a lack of experienced nurses with more professional expertise.
However, the growth of the foreign nurse labor niche in the United States has also led to problematic outcomes not easily captured in the brain drain narrative. Given the Philippines’ largely private higher education system, aspiring migrants pay the cost themselves of enhancing their overseas employability, leaving the Philippine state free to benefit from their future remittances without having to invest in their education. Aspiring migrants also absorb the risk involved in obtaining necessary qualifications for future jobs in the context of an unstable market. Although these uncertainties affect undergraduates all over the world, they are magnified in the Philippine context, where both students and schools aim to fill nursing labor needs beyond national borders. When the most recent nursing “boom” that propelled an outflow of Filipino nurses to the United States ground to a halt during the 2008 financial crisis, stemming the recruitment of foreign nurses, visa processing for Filipino immigrants went into “retrogression”—the term used by embassy officials when the number of visa applicants exceeds the number of visas available (Acacio 2011). Here I discuss the implications of such events for the everyday lives of Filipino nurse graduates and their plans for the future.
METHODS
This article stems from a larger project analyzing the ways in which Philippine universities attempt to educate graduates for “export” to the global market by adjusting school policies and curricula to meet the anticipated needs of foreign employers. From 2011 to 2014, I conducted fieldwork in Manila, where I interviewed educators and students from programs associated with overseas jobs, such as nursing programs and hotel and restaurant management (HRM) programs. My findings are based on a total of 104 interviews with nursing students, instructors, and graduates. This sample includes fifty-three nurse educators and twenty-one nursing students who were working and studying at private nursing schools at the time I conducted my fieldwork. I also interviewed thirty individuals who graduated from nursing programs between 2005 and 2011 but were unable to find work overseas.
It is important to note that in nursing the boundaries between instructors, students, and graduates are often blurred. At the height of the nursing boom, fresh graduates were immediately hired as instructors, often within six months, and even if they had limited hospital experience. I found that many of the “nursing graduates” who had left the profession were actually former clinical instructors who had moonlighted in nursing schools at one point in their careers. These interviewees shifted between different perspectives, speaking sometimes as a former nursing student or instructor, and sometimes as a former nurse who was no longer practicing the profession.
I recruited participants by circulating an invitation letter through school associations and asking participants to refer me to other faculty, students, and recent nursing graduates. At the time I conducted my interviews, some graduates had entered government programs that deploy unemployed nursing graduates to rural communities; many others had left the profession and were working as call center agents or sales representatives. Interviewees were relatively privileged, given that only one-third of Filipino high school graduates are able to pursue higher education (Asis and Batistella 2013). Nursing is also one of the most expensive degrees in the Philippines. Nevertheless, I would not consider my respondents part of Manila’s wealthy elite. Most upper-class students attended universities that were far more expensive than the nursing schools I visited. At the same time, many of my interviewees had overseas relatives who sponsored their school fees, without which they would not have been able to afford to go.
I asked interviewees why they decided to pursue nursing as a profession, how they experienced the decline in demand for nursing degrees, and what happened when they looked for work after graduation. This article is limited in that I did not interview nursing graduates who had succeeded in finding work in the United States.
LEARNING TO FILL THE LABOR NICHE
Despite the growing emphasis on academic credentials, the global economy has seen a decline in permanent employment and increasing instability within workplaces (Brown, Lauder, and Ashton 2011; Kalleberg 2009; Smith 2010). As a result, students today spend more on schooling but are less likely to get the jobs they want (Brown and Hesketh 2004; Tomlinson 2008). Yet the promise of higher education and future immigrant success remains a convincing reason for many Filipino students to pursue a four-year degree in nursing. A quick glance at Philippine migration statistics shows that an aspiring migrant could easily leave the country as a domestic helper or construction worker, with little need for academic training or credentials. Still, my interviewees wanted to obtain jobs with better wages, higher social status, and protections against employer abuse—privileges that many of their migrant relatives had not been able to enjoy. College education thus served as an expensive “investment” in a better future and a better migration experience. Joey, a 2011 graduate, explained that the idea of becoming a nurse came from his mother, who was working as a domestic helper in Italy:
Mama was jealous of her friends whose children were able to get good jobs in Italy because they were nurses. … So the reason I took nursing was so we could swap, I will be the one to work there and she can finally come home. It’s hard now because [pause] she’s not legally allowed to be there.
Joey was lucky to get a scholarship that covered most of his tuition at a private university. However, his mother still struggled to remit enough money for miscellaneous fees, field trips, uniforms, and the countless supplies that nursing students had to bring with them during clinical rotations. “For every visit to the [hospital], you had to buy surgical gloves, cotton, medicine … if your nursing kit was not complete, the instructors would take points off your grade,” Joey said. “After one semester, I could tell Mama was starting to regret choosing this major, but she worked hard to make sure I graduated.”
Other interviewees did not have a parent who funded their education but relied instead on “sponsors” or relatives working overseas. Most of these sponsors perceived higher education as a means to pass on to a younger member of the family the responsibility of supporting the family. Some sponsors worked in blue-collar positions, like Joey’s mother, but many were also professionals within the health field. These migrants chose a young family member to finance through college with the hope that they would eventually be able to go overseas as well. Nestor, who graduated in 2014, said that he owed his college degree to his dad’s sister, a nurse working in the United States.
My tita [aunt] has a lot of influence in our family. She’s really successful in the U.S., and she was able to help everyone in our family. I’m the eldest grandson, so everyone [in the family] said that I should take nursing like her. Then I can be the one to help my family when I graduate. … But if you ask me, I wouldn’t take nursing. I wanted to take architecture or business management. Those fields are more of my forte. But I don’t really have a choice. I can’t just pick a major because I like it. I have to think of my family too.
Pursuing a higher education degree as a step toward emigration is not a misguided plan. One needs academic credentials to obtain professional work, and in many migrant-receiving countries, higher degrees are an increasingly important factor in deciding which immigrants are granted entry (Kofman 2007). This rationale has justified the promotion of export-oriented strategies among local universities and the push in migrant-sending states like the Philippines for academic programs that train students for labor niches overseas (Ortiga 2017). Yet, as mentioned earlier, the pursuit of higher education as a means to finding overseas work exacerbates the risk for college-educated graduates in the Philippines of getting caught in one or both of two types of traps that can lead to underemployment and brain waste.
The Migration Trap
The opportunity offered by the U.S. nursing labor niche to Filipino nurses is often fleeting and unstable. Open positions are filled very quickly, and U.S. officials change immigration policies depending on nationality quotas and domestic conditions. Thus, Filipino students who invest in certain degrees in the hope of migrating often discover that they are unable to leave the country because they have graduated at the end of an overseas job trend. This is the problem of the migration trap.
Rina Jimenez-David (2008) describes the migration trap as a problem for those who have already obtained their degree, but aspiring migrants among my interviewees shared that they felt “trapped” even before they graduated. As students, many of them were well aware that overseas opportunities for Filipino nurses were dwindling; subsequently, many were left stuck in the Philippines and struggling to find work. Gina, a nurse who graduated in 2006, said that even while the number of students enrolled in her college was still high, she started to hear stories about previous cohorts who could not find work:
I could tell something was wrong [in senior year] when I would see some of our graduates around town. I would ask them what they’ve been doing, and they’d say, “Wala!” [Nothing!], or, “Nasa bahay lang, tambay!” [Just hanging out at home!] Or sometimes I would see them in the hospital, working as volunteers … with no salaries! That’s when I started to wonder what would happen to me.
Despite these signs, many nursing students did not want to “waste” the money they had already spent on books and nursing courses by shifting to another program. Daisy, who graduated in 2014, said that after she graduated from high school, “my parents told me that nursing is a very expensive major so they really asked me if I could handle the load. They said, ‘Once you start, no more shifting to another major!’” Similarly, Patrick, Daisy’s classmate, shared that college was a “luxury” for his family. As such, paying extra money for more classes would have been out of the question. He explained, “My mother told me that college is a one-shot deal. If I flunk a class or drop a class, they will pull me out. I think it’s because the money for my tuition is not from them, it’s from my aunt in Canada. So yeah, just one shot.” Although Patrick and Daisy knew that the opportunities for migrant nurses had waned, financial and time constraints prevented them from pursuing other courses of study. Because Philippine college curricula require students to take major subjects as early as the first semester, it is harder for students to shift majors without worrying about delaying their graduation.
Caught in the migration trap, nursing graduates said that they became depressed with their situation: still being required to continue with the difficult clinical rotations and board exam reviews amid such career uncertainty. Few students wanted to practice as nurses in the Philippines given the low wages and deplorable working conditions in local hospitals (Guevarra 2010; Lorenzo et al. 2007). The nursing profession attains high social status in the Philippines only when associated with possible emigration. Otherwise, nursing is seen as a thankless, undesirable job. “It’s disappointing and degrading,” said Jay, who graduated in 2012. “Before, people would look at you and say ‘Wow, nursing student!’ They look up to you. Now, after the decline, it’s like, ‘Ah, laos na course mo, maghanap ka nalang ng iba.’ [Your major is obsolete, find something else to study.] But I was in my third year already, so what else can I do but finish?”
Looking back at their educational experience, nursing graduates shared that timing was the trickiest part of choosing the right college major. Parents and relatives had little idea of whether the demand for nurses in the United States would last until their children completed a four-year degree. Mira, who took nursing as a “second course,” shared that she always had “bad luck” in choosing college majors. She first pursued microbiology as a premed major in 1998, but realized as she approached her senior year that her parents could not afford to send her to medical school. Not wanting to go into research or teaching, she took a job at one of the many call centers in Manila. In 2003, her parents suggested that she take up nursing, and an aunt who lived in the United States volunteered to pay her tuition. Mira recalled that there had been about two thousand students in her cohort, about one hundred of whom were also pursuing nursing as a second degree. “I thought I had chosen a good time to go back to school. We were so many,” she admitted. Yet by the time Mira graduated and passed her board exams in 2008, the number of nurses leaving for the United States had started to decline, and the sheer number of nursing graduates had overwhelmed Philippine hospitals. Feeling trapped with another degree that “doesn’t lead anywhere,” Mira returned to call center work.
For other interviewees, the problem of bad timing was made worse by employer demands for international certification, appropriate work experience, and language tests (Kingma 2006). Lorna, who obtained her nursing degree in 2004, claimed that she had completed all her requirements for immigration by 2006, right when U.S. hospitals started to stem the hiring of foreign nurses.
My sister-in-law passed all her requirements in 2005, and they processed all her papers in less than a year. I thought I would still make it, but it was too late. Maybe because of the financial crisis in the U.S., they became stricter with visa applications. The agency tells me there’s still a demand. The government just doesn’t want to bring in more people. … Now, I just think that if a new opportunity comes again, at least I’ll be the first in line.
Lorna comforted herself with the idea that her investments in certification would open up the possibility of migration in the future. Yet she was unsure as to when the “next time” would be, and she admitted that some of her exam results would become invalid in five years. She would then face the risky decision of whether to invest even more money in her migration plans, given the unpredictable timing of nurse recruitment in destination countries.
These Philippine aspiring migrants were not stereotypical Third World immigrants, desperate to leave under any circumstances, but rather sought particular conditions for emigration. Even though caught in the migration trap, they did not necessarily have no means of leaving the country. Rather, they were unable to leave in the manner they had envisioned and in which they had invested. At the time of my interviews, government agencies still reported a need for nurses in places like Yemen, Jordan, and Saudi Arabia. However, few of my interviewees would consider working in the Middle East, mainly because of what they had heard about Arab employers. Tanya, a 2014 nursing graduate, said that employers in the Middle East were “violent” and “abuse women.” Although she knew little about Middle Eastern countries, she said that she had seen enough on TV to decide that she did not want to work in the region. Similarly, Mara, a 2011 nursing graduate, said that her parents wanted her to work only in the United States and that “they would worry too much if I went anywhere else.”
These views reveal that nursing graduates’ decision to emigrate is often more nuanced than simply a quest to earn higher wages. Philippine nursing students pursued higher education in the hope of gaining access to the United States even with no assurance that their college degree would automatically lead to a job in an American hospital. Studies of college students in other countries echo this trend: students spend exorbitant amounts on higher degrees with no clear notion of the difficulties they will face after graduation (Arum and Roksa 2011; Brooks and Everett 2009). In the Philippines, however, this problem is made worse by an export-oriented education system that directs students toward the promise of opportunities beyond national borders.
The Opportunity Trap
Nursing graduates caught in the migration trap face two choices: find other ways to practice nursing, or leave the profession altogether. Yet, whichever decision they make, nursing graduates often find themselves caught in another difficult situation: struggling to accumulate more and more credentials to improve their chances in a poor job market. The sociologist Phillip Brown (2003) calls this the problem of the opportunity trap: individuals continuously pursuing training and education to obtain tough-entry jobs, despite little evidence that more qualifications will lead to better opportunities. As more people engage in this strategy, the harder it becomes for anyone to get ahead. Yet few can forgo this race for credentials given the risk of completely losing out in the end.
In the Philippines, the massive number of nursing students has worsened the effects of the opportunity trap. As the number of jobs in the United States began to drop, graduates scrambled to differentiate themselves from the thousands of others with the same academic qualifications. Many of my interviewees remained hopeful that the U.S. market would open up for the recruitment of migrant nurses in the future and worked fervently to “build up” their résumés with extra training and certification. With only limited open positions, however, Philippine hospitals were unable to absorb the thousands of nurses flooding the market. Mirielle Kingma (2007), a consultant for the International Council of Nurses, notes that this problem is common in countries that experience high rates of nurse migration, not because of a lack of need, but because local hospitals lack funds and support for staff. Desperate for work experience, many of my interviewees resorted to paying for their own professional development, thereby adding to the thousands of pesos their families had already invested in their education.4
One expensive option was pursuing a master’s degree in nursing. For many of my interviewees, “going back to school” seemed like a better way to spend their time, given the lack of hospital jobs for nurses in the current market. Yet these nurses had only a vague idea of whether such a credential would actually lead to higher returns in the United States. Rey, a nurse who graduated in 2007, was one of the lucky few who found full-time work, at a children’s hospital in Manila. He attended graduate classes during his free time and eventually obtained a master’s degree in nursing. Rey admitted that he was not really sure what opportunities a master’s degree would bring, but he had enrolled in the program because his colleagues were doing the same thing:
A lot of people believe that a [master’s] will help you get to the U.S., but that’s not true. I took it because I would hear all the other nurses talking about wanting to take a master’s. There would be all this talk about how their master’s will be credited abroad or how it will make sure you get a higher rank when you go abroad. Now I find it funny because they wanted the degree, but they don’t really know what it involves.
Research does indicate a need for more nurses with postgraduate degrees, mainly to take on faculty positions in understaffed nursing schools in the United States. Yet, with foreign recruitment mainly channeling migrant nurses into hospitals and nursing homes (Keuhn 2007), it is unclear whether a master’s degree from the Philippines would be an advantage to them. Nurses like Rey are most probably overqualified for the positions they are likely to obtain in the United States.
For nursing graduates who find pursuing a master’s degree too costly and time-consuming, enrolling in short-term “training sessions” can be a more viable alternative. Offered by both public and private hospitals, these sessions provide nursing graduates with “certified” skills in specialized areas of the hospital. Amy, who graduated in 2008, shared that since she passed the board exams, her mother had spent 26,000 pesos (about U.S.$523) on two training sessions: a three-week seminar on inserting intravenous tubes, and a six-week session on being a dialysis nurse. Amy confided that she was ashamed to ask her mother for more money, given that her parents had already financed her college education. However, her mother had insisted that she go for the training rather than give up and work at a call center. Sheila, who graduated in 2007, paid for two training seminars; focused on occupational health and safety, they catered to would-be company nurses. Like Amy, Sheila paid for her extra training with the help of a cousin in the United States, who also funded her nursing education. She believed that the extra investment increased her ability to perform certain hospital tasks, thereby enhancing her employability. Both Amy and Sheila rationalized their decision to undergo further training by arguing that training certificates would be useful when applying for work overseas.
Although such training certificates do provide nurses like Amy and Sheila with some advantage over their peers, they represent a costly investment that is fully absorbed by individuals and their families. The head nurse of a local private hospital confided that such training sessions used to be offered as free professional development seminars for hospital staff. With the large number of unemployed nursing graduates in need of “exposure,” hospital administrators opened these sessions to the public, thus garnering a very lucrative source of extra income.
Although paying for what was once offered for free may have seemed unfair, many nursing graduates felt that enrolling in these training sessions was still better than volunteering at local hospitals. With nurses outnumbering the available positions in Philippine hospitals, many resorted to providing their labor for free, just to get the work experience required by many foreign employers. At one point, local hospitals even started charging nursing graduates for the “experience” of working in the hospital. One interviewee shared that administrators in her university charged their own graduates 6,000 pesos for only three months of “exposure” in the campus hospital. The fees were higher for work in specialized areas such as kidney dialysis. Eventually, news of nurses paying to work led to a public uproar, prompting Philippine politicians to ban hospitals from collecting these fees. However, hospitals—both public and private—could still accept nurse “volunteers,” thus continuing to benefit from their free labor.
Sadly, these volunteer experiences do not always pay off. Aside from paying for training sessions, Sheila also volunteered in two medical institutions: a public community hospital and a larger private hospital in her home province. Both hospitals gave her a certificate designating her a “Volunteer Nurse,” but unfortunately, recruitment agencies refused to accept it. “They said that the hospitals [overseas],” she complained, “will not accept a nurse who only had experience as a volunteer. My COE [certificate of experience] said I was a ‘Volunteer Nurse,’ not a ‘Staff Nurse,’ but we did the same work as the hospital’s nurses! Of course the staff nurses did most of the difficult procedures, but in most wards, there were only two staff nurses. Everyone else working were volunteers!”
In response to this problem, Philippine state agencies implemented short-term programs that employed nurses in health centers and provincial hospitals in the country’s rural areas. Interviewees saw this program as a temporary way to pay the bills, but not as a training ground to enhance their chances of migration. Patrick, who finished a one-year stint with this program, did not find the experience useful in his migration plans because he had been limited to routine procedures like administering vaccines and taking vital signs. In fact, his nursing job was so “easy” that he worked part-time at his aunt’s convenience store and transcribed interviews for a researcher at a local university. Many of his classmates avoided these government programs, despite the lack of nursing jobs elsewhere. “No one really wants to work in [rural communities],” Patrick said. “Your work there is not credited if you want to go abroad, so it’s pretty useless.” The only “break” Patrick caught came when the head nurse at the government hospital where he was volunteering secretly gave him a certificate of experience as a staff nurse. “Actually, what she did was illegal, because we were volunteers, not full-time staff. Naawa lang talaga siya sa amin [She just felt so sorry for us].” With his COE, Patrick applied for a nursing job on a cruise ship. He had given up on making it to the United States.
Given the resources needed to remain in the nursing field, more than half of my interviewees opted to leave the profession altogether. Facing pressures to contribute to the household income, many of them could no longer afford to spend more money for training, work experience, or certification. Unfortunately, the decision to leave nursing did not always lead to freedom from the opportunity trap. Jimenez-David (2008) argues that many nursing graduates are also likely to receive the “short end of the employment stick,” partly because potential employers fail to recognize their qualifications and skills. As a result, nursing graduates seeking new professional careers must still pursue credentials in order to gain entry into other fields. A few parents allowed their children to go back to college and major in other areas like education or business management. Most opted for cheaper alternatives such as technical vocational (tech-voc) certificates awarded by the Philippine Department of Labor and Employment. Although a tech-voc certificate was considered a “demotion” from a college degree, nursing graduates rationalized that many tech-voc courses were related to health and lent some professionalism to their résumé. Arnel, a 2007 nursing graduate, became a certified “spa therapist” after obtaining a tech-voc certificate in massage therapy. He initially paid for a tech-voc certificate in caregiving, thinking that he could still go to Canada to work as a live-in caregiver. However, available openings for caregivers had declined by the time he finished the course, so he was now focused on teaching massage therapy to other nursing graduates like himself. He admitted that, despite his successful change in career, his job carried a certain stigma among family and friends. “Someone once told me, ‘Nag-nursing ka pa eh ngayon masehista ka lang.’ [All that work to be a nurse and now you just give massages for a living.] I just keep quiet and then post pictures of myself on Facebook, lecturing my class on massage therapy.”
While nursing graduates like Arnel were determined to remain within the health field, others entered other industries where employers were not choosy about academic degrees, mostly in the field of business process outsourcing (BPO). In the Philippines, call center agencies actively recruit new graduates to answer customer queries, transcribe meeting notes, and process company databases. These jobs offer much higher pay than nursing positions in Philippine hospitals, yet interviewees perceived call center work as requiring few skills—especially the kind they worked hard to develop in their professional education.
Other nursing graduates settled for either domestic work or low-skilled service work, both locally and overseas; such jobs were readily available and did not require too much paperwork. Darlene, a 2007 graduate, found work as a cashier at a factory canteen after working as a salesgirl and a grocery store attendant. She had spent the first few years after graduation as a volunteer nurse in a public hospital, but because she had to care for her elderly father, she decided that she could no longer afford to work for free. Now, almost a decade after she passed the nursing board exams, she was considering applying for domestic work positions in Singapore. Unlike Darlene, Kim, a 2009 graduate, had spent little time looking for nursing jobs or investing in further training. Her parents had used most of their savings on her nursing degree, and she was expected to help pay for her younger siblings’ education after graduation. After a few months of unsuccessfully trying to find work as a nurse, she took on a housekeeping job at a hotel in New Zealand. Despite her current situation, Kim said that she would like to return to nursing as a profession. Yet her family’s financial needs made it hard for her to spend more time and money keeping herself employable for the next time nurse recruitment resumed.
CONCLUSION
In seeking to enhance their chances of migration through education, nursing graduates face the risk of getting caught in the migration trap and the opportunity trap—continuously upgrading their skills and credentials in the hope of getting jobs that do not exist. These problems do not affect only migrant-sending countries. As noted by the sociologist Vicki Smith (2010, 280), today’s global economy has made it the responsibility of individuals to prove their employability—that is, the “professional and personal capacity to maximize one’s employment potential.” Even nonmigrant graduates in wealthy nations encounter problems of underemployment and joblessness; many are unable to practice in the field for which they have been educated and end up working in jobs that do not require a college degree (Asis and Batistella 2013; Brown, Lauder, and Ashton 2011). In the Philippines, however, the promise of higher education has been incorporated into a state-led system of labor export that encourages students to become educated in fields that will fill overseas labor gaps. As such, growing labor niches in desirable destination countries like the United States, as we have seen with nursing, can create massive change within Philippine higher education institutions, as schools take advantage of the thousands of aspiring migrants seeking to enhance their overseas employability.
These export-oriented education strategies complicate typical narratives about the impact of U.S. nursing labor shortages on source countries. On the one hand, the influx of Filipino nurses into the United States motivates young Filipinos to pursue four-year degrees in nursing, thus increasing the number of students seeking higher education in the country. As an immigrant labor niche, nursing is very dynamic in that it offers opportunities for professional growth and vertical mobility not offered by other occupations (Eckstein and Peri, this issue). The cyclical nature of the U.S. nursing labor shortage then provides long-term opportunities for aspiring migrants looking to invest in nursing education. Although changing visa requirements and domestic work conditions have temporarily stopped the influx of foreign nurses, U.S. nursing schools are still unable to produce enough graduates for American health care institutions. Thus, overseas recruitment of nurses is likely to continue in the future.
On the other hand, export-oriented education can exacerbate a mismatch between available jobs (both locally and overseas) and the actual number of graduates produced by colleges and universities. Philippine private schools bear no responsibility for placing their students in appropriate jobs after graduation, and Philippine government agencies do little to address the needs of nursing graduates who are unable to find work when overseas opportunities decline. Studies have highlighted the ways in which migration costs usually disadvantage workers, especially those from lower socioeconomic backgrounds, yet most of these studies have focused on recruitment costs paid to private placement agencies (see Martin 2012). This article elucidates the enormous cost and effort incurred by Filipino students seeking higher education in order to remain employable for their future U.S. employers, sometimes with little idea of how long such labor demand will last.
In the end, few of my interviewees had the luxury of waiting for the long-term benefits of their higher education, and as such, their experiences indicated a looming problem of brain waste rather than brain drain. Given the dismal work conditions for nurses in the Philippines and the lack of funding for hospital staff, having more nursing graduates does not necessarily translate into more nurses working in Philippine hospitals. Instead, thousands of qualified nurses find themselves back in school, working in call centers, or leaving the country as domestic and service workers. What is wasted is not just the money spent on college tuition, but the time and effort invested in becoming a professional nurse, with expert knowledge and health care delivery skills. Meanwhile, Philippine government agencies, such as the Commission on Higher Education, lament the continued dearth of qualified college graduates in fields that would benefit local industries, such as marine biology, mathematics, dentistry, and social work (Gamil 2011; Pazzibugan 2013).
Despite the problems faced by nursing graduates, Philippine state agencies are unlikely to prevent private nursing schools from expanding their programs when the recruitment of foreign nurses to work in the United States resumes. At the same time, the Philippines faces increasing competition in the migrant nurse labor market as other countries, like China, India, and Vietnam, adopt similar strategies to facilitate the out-migration of their citizens (Brush and Sochalski 2007). This continuous push toward export-oriented education strategies amid rising uncertainty forewarns us about future problems—problems not fully captured in the prevailing brain drain narratives—as new immigrant niches continue to emerge within large destination countries like the United States.
FOOTNOTES
↵1. As political instability and economic problems pushed more Filipinos to seek overseas employment, migration industries grew within the country, offering placement services for individual workers hoping to find better opportunities abroad (Asis 2006; Rodriguez 2010). In the 1970s, then-president Ferdinand Marcos chose to institutionalize the migration process: “labor export” was turned into an economic strategy for national development. This period saw a general policy shift toward “managing” migration outflows instead of trying to prevent people from leaving the country (Acacio 2008, 104). Government bodies made concentrated efforts to direct the movement of people through “official channels,” thus “allowing for greater transparency in labor transfers, employment conditions, migrant earnings, and foreign exchange remittances” (Acacio 2008, 104).
↵2. Although Filipino aspiring migrants saw the United States as their ideal destination, Philippine nursing schools took on the task of educating their students for a “global” market—for instance, by introducing language electives for countries like Japan and Germany and offering courses on “transcultural nursing.” Elsewhere (Ortiga 2014) I have written about the pressures this puts on Filipino nurse educators.
↵3. After the Philippines achieved independence in 1946, the war-torn government barely had the capacity to run its universities, much less establish new institutions. Budgetary constraints continue to this day, and the bulk of the state’s education budget is still allotted for basic education. To date, 88.1 percent of the country’s 1,934 higher education institutions are privately owned (Philippine Commission on Higher Education 2016).
↵4. Interviewees did not mention their parents borrowing money or going into debt for their education, although it would not be surprising if this was the case for many of them. Rather, interviewees talked about their parents using hard-earned savings or relying on remittances from a relative working overseas.
- © 2018 Russell Sage Foundation. Ortiga, Yasmin Y. 2018. “Learning to Fill the Labor Niche: Filipino Nursing Graduates and the Risk of the Migration Trap.” RSF: The Russell Sage Foundation Journal of the Social Sciences 4(1): 172–87. DOI: 10.7758/RSF.2018.4.1.10. Direct correspondence to: Yasmin Y. Ortiga at yasmin.ortiga{at}nus.edu.sg, College of Alice and Peter Tan, University Town, National University of Singapore, 8 College Avenue East, #B1-50, Singapore 138615.
Open Access Policy: RSF: The Russell Sage Foundation Journal of the Social Sciences is an open access journal. This article is published under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.
REFERENCES
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.