
Abstract
Sleep is a key restorative process, and poor sleep is linked to disease and mortality risk. The adolescent population requires more sleep on average than adults but are most likely to be sleep deprived. Adolescence is a time of rapid social upheaval and sensitivity to social stressors including discrimination. This study uses two weeks of daily e-diary measures documenting discrimination exposure and concurrent objective sleep indicators measured using actigraphy. We assess associations between daily discrimination and contemporaneous sleep with a diverse sample of adolescents. This novel study shows youth with higher average discrimination reports have worse average sleep relative to their counterparts. Interestingly, youth reporting daily discrimination have better sleep the day of the report than youth who do not.
Sleep is an important restorative process instrumental in regulating physiologic systems, cognition, and behavioral outcomes (Balbo, Leproult, and Van Cauter 2010; Kliewer and Lepore 2014). Sleep quality and duration are associated with an array of morbidities including metabolic conditions, cardiovascular disease, and major depression (Irwin 2015). Because adolescents are a population vulnerable to poor sleep during a key developmental period of significant physiological and environmental change, they are an important group to systematically assess with regard to sleep patterns and social conditions linked to chronic disease risk (Becker, Langberg, and Byars 2015; Park et al. 2016). A growing literature indicates that sleep may function as a key mechanistic pathway through which exposure to social stressors such as discrimination or other social exclusionary experiences decrease health (Lewis et al. 2013; Hicken et al. 2013). This research, however, primarily focuses on adult populations with inferences based mostly on self-reported rather than objective sleep measures. This study fills the gap in existing sleep research by examining adolescents, a key at-risk group for poor sleep and stressful social dynamics, using a lengthy window of objective actigraphy-based sleep measures.
Adolescence is a critical time to study the impact of social stressors on sleep because they are more likely, on average, to report difficulty falling asleep, staying asleep, and to be chronically sleep deprived (Yip 2014; Carskadon 1990). For adolescents, sleep is instrumental in the ability to regulate negative emotions and coping with stressful conditions (Dahl 1999; El-Sheikh et al. 2010). Although frequency of day-to-day discrimination exposure as well as accumulated discrimination has been linked to poorer mental and physical health outcomes, less is known about the role of discrimination for sleep patterns among adolescents (Schmitt et al. 2014; Goosby et al. 2015; Torres and Ong 2010). To address these gaps, this study uses novel pilot data from a diverse sample of adolescents combining survey data, daily electronic-diaries (e-diaries), and actigraphy-based sleep measures to address the following questions (Eufemia et al. 2012): In early to mid-adolescence, do experiences of discrimination or unfair treatment affect sleep (both quantity and quality) consistently over time? Do daily fluctuations in such experiences influence nightly sleep variability?
LITERATURE REVIEW
Public health concern is growing over sleep quality and duration, also known as sleep health, in the United States. Nearly 25 percent of the U.S. population report insomnia complaints and 10 percent meet clinical criteria for insomnia (see Irwin 2015). Due to the importance of sleep for numerous health and behavioral outcomes, interest in studying sleep quality and duration is considerable (Kingsbury, Buxton, and Emmons 2013; Gregory and Sadeh 2012; Irwin 2015). Moreover, increasing evidence suggests that sleep characteristics differ across populations and are linked to social and environmental conditions.
Sleep patterns appear to vary by sociodemographic factors that include age, socioeconomic conditions, race and ethnicity, and education (Hale, Emanuele, and James 2015). Adolescents, for example, as a group require more sleep on average (approximately nine hours) but are less likely to actually get adequate sleep than adults (Becker, Langberg, and Byars 2015). People living in economically disadvantaged and segregated neighborhoods also have poorer sleep quality, in part due to the excess noise and crowding found frequently in such environments (Hale, Emanuele, and James 2015; Massey 2004). Race differences are also documented, particularly among African Americans relative to whites; African Americans are a population at higher risk for living in or near economically disadvantaged neighborhoods and at higher risk for disruptive chronic stressors (Williams 2012). Consequently, this population commonly shows signs of harmful sleep patterns by sleeping both shorter and longer durations than the recommended average and accompanied by poorer sleep quality that is less restorative (Kingsbury, Buxton, and Emmons 2013; Mezick et al. 2008; Profant, Ancoli-Israel, and Dimsdale 2002).
Yet much of the literature has used subjective sleep reports rather than objective measures of sleep, and that subjective reports have relatively low reliability relative to more objective measures is well documented (Short et al. 2012, 2013). Respondents asked retrospectively about their sleep duration, for example, are more likely to overestimate duration and underestimate number of awakenings during the night; adolescents in particular may tend to only report more salient, recent information (Wolfson et al. 2003). Daily diaries are another self-report approach to measuring sleep that has the advantage of capturing day-to-day variation usually over an extended period to characterize sleep. Use of temporally proximal data on sleep habits across a range of days is more strongly correlated with laboratory-based gold standard measures of sleep quality than one-shot, long-term subjective self-reports (Wolfson et al. 2003). Among self-report measures, sleep diaries appear to provide the most reliable sleep measures, particularly among adolescents (Short et al. 2013). Sleep diaries, however, tend to overestimate total objective sleep time and underestimate awakening frequency during the night because individuals may not always be aware of waking during the night or other factors that may make sleep more or less restful (Short et al. 2012; Wolfson et al. 2003).
Although self-reported measures of sleep can provide meaningful information and in some cases be correlated with objective sleep measures, they are not as reliable in accurately measuring total sleep duration, waking after sleep onset, or activity during sleep. In nonlaboratory settings, the current state-of-the-art method for objectively measuring sleep dimensions is actigraphy (Short et al. 2012). Actigraphy uses accelerometers placed on the wrist to document sleeping and waking states (Marino et al. 2013). Though actigraphy cannot measure specific sleep architecture or sleep staging, it has been validated to accurately measure distinctions between sleeping and waking along with total sleep time (TST) in both sleep disordered and general populations (Ancoli-Israel et al. 2003). Actigraphs are particularly useful for nonlaboratory studies because they can be worn for extended periods for tracking sleep patterns, which cannot be feasibly measured in sleep labs. Despite the convenience of actigraphy for measuring sleep in the field, use of it is not yet as common in studies of adolescence. We broadly characterize adolescents’ sleep using a rich set of actigraphy measures taken nightly over a two-week period, emphasizing a key exclusionary social experience, discrimination, and relationships to different features of sleep.
Discrimination and Sleep
The need for social bonding and connection is among the most basic of all human needs (Baumeister and Leary 1995), and our health suffers when our needs for social connection are not satisfied (Cacioppo and Patrick 2009). Social exclusion has widespread implications for health, health behaviors generally, and sleep specifically (Hawkley et al. 2003; Duclos, Wan, and Jiang 2014; on sleep, Pereira, Meier, and Elfering 2013; Sladek and Doane 2014). A key dimension of social exclusion is the perception of discrimination or unfair, prejudicial, and exclusionary treatment based on certain characteristics or stigmatized identities such as race, obesity, gender, and sexuality (among others). Specifically, discrimination has been linked to a variety of health outcomes including poorer self-rated health (Krieger et al. 2011), high blood pressure (Lewis et al. 2009), vascular resistance (Guyll, Matthews, and Bromberger 2001), adiposity (Lewis et al. 2011), increased inflammation (Lewis et al. 2010), and higher allostatic load (Brody et al. 2014). As early as adolescence, discrimination is linked to worse self-rated health (Priest et al. 2013), depressive symptoms (Hope, Hoggard, and Thomas 2015), anger (Wong, Eccles, and Sameroff 2003), as well as elevated systolic and diastolic blood pressure, and higher C-reactive protein (CRP) (Goosby et al. 2015). Although less is known about the links between discrimination and sleep quality than some other stressors, research suggests that even the anticipation and rumination on social exclusion can decrease sleep quality (Hicken et al. 2013; Åkerstedt 2006; Åkerstedt, Kecklund, and Axelsson 2007).
In findings from sleep lab clinical studies, discrimination exposure predicts less time in restorative sleep stages and greater daytime fatigue in adults (Thomas et al. 2006). In nonclinical, larger scale surveys, differences in subjective sleep quality and wakefulness after falling asleep among African Americans relative to whites are attenuated (though not eliminated) by reports of chronic discrimination (Lewis et al. 2013) and racism-related vigilance (Hicken et al. 2013). Although the evidence from adults points to a key role for perceived discrimination in reducing sleep quality, less is known about links between discrimination and adolescent sleep. Limited available evidence suggests that the same pattern for adults may also hold for youth; adolescents who retrospectively report experiencing higher levels of discrimination over the past year reported lower sleep quality and quantity in their daily sleep diary reports (Yip 2014).
Discrimination exposure and sleep are dynamic processes, but most studies in this area have so far relied heavily on retrospective measures of both discrimination and self-reported sleep quality. Despite the cross-sectional nature of these studies, the links between discrimination and sleep, as well as for other health outcomes, are robust. In a study of Latino youth, researchers Lucas Torres and Anthony Ong use daily diary information documenting both discrimination events and depressive symptoms found a day lag among youth who reported discrimination for subsequent elevated depressive symptoms (2010). Both this study and Tiffany Yip’s of 2014 suggest that the accumulation of chronic discrimination may have long-term implications for subsequent sleep; however, neither study examined daily discrimination experiences and sleep contemporaneously, thus leaving an open question regarding whether discrimination can have more immediate consequences for youth sleep patterns.
Our study aims to address these gaps in the literature by first assessing the temporal relationship between daily experiences of discrimination and subsequent objective dimensions of sleep among a sample of adolescents. We explore sleep both as average sleep trends over a two-week period and as day-to-day fluctuations in sleep. Our first hypothesis (H1) posits that the accumulation of discriminatory experiences is related to poorer average sleep. Our second hypothesis (H2) states that adolescent sleep will be poorer on days that adolescents perceive they have been discriminated against.
DATA AND METHODS
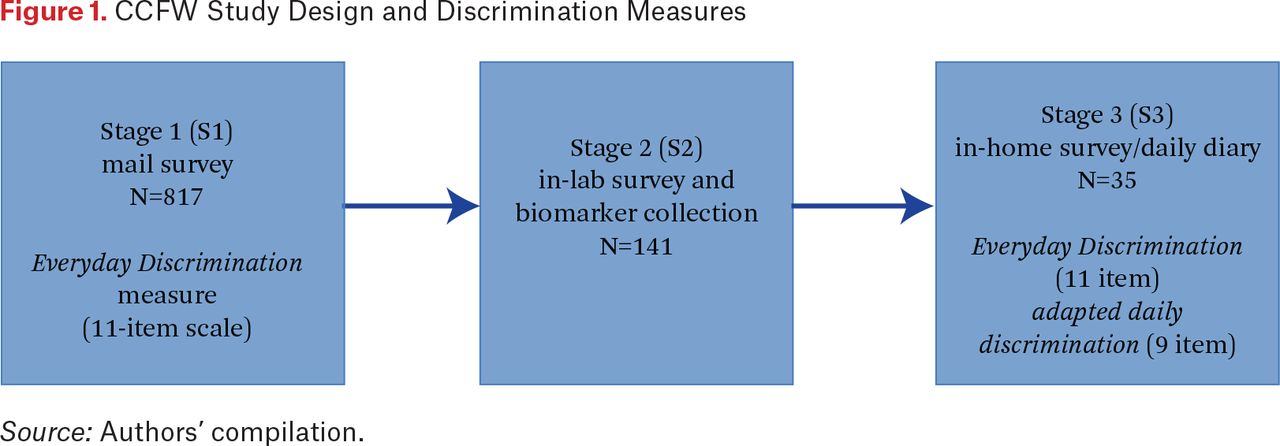
Data in this study come from the Community Connections and Family Wellness Study, which was designed to assess the intergenerational health and well-being of parent-child dyads and was originally conceived of as a two-part pilot study comprising a mail survey screening for an in-lab component to develop and assess recruitment protocols for a larger social neuroscience project (Falk et al. 2013). Sampling and data collection methods included three stages ranging over two years. Figure 1 outlines the stages (S1–S3) of data collection for this multistage sample. In stage 1, in collaboration with a local school system in a mid-sized Midwestern city, we contacted a subset of 2,181 (1,000 white, 1,181 African American or biracial) middle- and high school students ages eleven through fourteen in the school district during the fall of 2014. Two survey packets, one for the parent or guardian and another for the student, were mailed to each family in summer 2014 with a $2 incentive for each. A total of 817 parent-guardian and child dyads completed the mail surveys in stage 1.

CCFW Study Design and Discrimination Measures
The stage 2 data collection took place from December 2014 to June 2015 with a subset of 141 parent-child pairs from stage 1 who expressed interest in participating in future studies. These participants were invited to visit a laboratory space on a local college campus where anthropometrics, biospecimans, experimental, and additional survey data were collected. Participants in this phase of the study were restricted to families of white, African American, and biracial youth with one African American parent. A $20 incentive was given to each participant along with meal vouchers for participants who were interested in visiting campus (based on responses to an incentive question during stage 1). The overall response rate for participation in the stage 2 portion of the study was 32.4 percent.
Approximately a year later, a subset of forty parent-youth dyads from the in-lab participant pool were recruited for a third stage (stage 3) in-home data collection between February and May 2016. At the initial home visit, after parental consent and child assent, the parent and child independently completed baseline survey measures of health, daily experiences, diet, sleep behavior, and anthropometric measurements. Participants were then trained to use ActiGraph Black/wActiSleep BT and Red/wGTX-BT wristbands and the daily online e-diary procedure (Eufemia et al. 2012). Both the parent and youth were sent an email nightly with a link to their e-diary, which was formatted for use on either a computer or smart device. Both the parent and youth were asked to wear the actigraph wristband all day and night for fourteen consecutive days to measure sleep activity. At the end of the period, parents and youth returned the actigraph wristbands and, to facilitate recruitment and retention of participants, were compensated with cash (up to $200 for the family based on adherence to the study protocol). High rates of protocol adherence (approximately 90 percent) were obtained with both e-diary and actigraph protocols.
Of the 113 families contacted for participation, fifty-eight could not be reached or did not return messages, and thirteen refused, had moved, or were otherwise ineligible. Based on the race of the child, twenty-one of the families were white, four were African American, and fifteen were biracial (one biological African American parent). However, because of missing sleep and biological data, only thirty-five families were used in these analyses. The distribution across race groups in the current analytic sample was twenty-one white, four African American, and ten biracial adolescents. Of these, sixteen were male and nineteen were female. For this study, African American and biracial youth were combined into one category because of the small sample sizes.
MEASURES
Sleep measures are derived from the mathematical decomposition of accelerometer data recorded continuously on the actigraph wristbands. The devices were configured to collect data at 60hz with the idle sleep mode enabled. The actigraphy measures were calculated using the ActiLife 6 software package (ActiGraph 2012). The actigraph data were segmented into sixty-second epochs and wear time validation was assessed using Troiano’s algorithm (Troiano et al. 2008). Sleep analyses then utilized Sadeh’s algorithms and were manually adjusted using bed and wake time information collected in the nightly e-diary (Sadeh 2011; Sadeh, Sharkey, and Carskadon 1994).
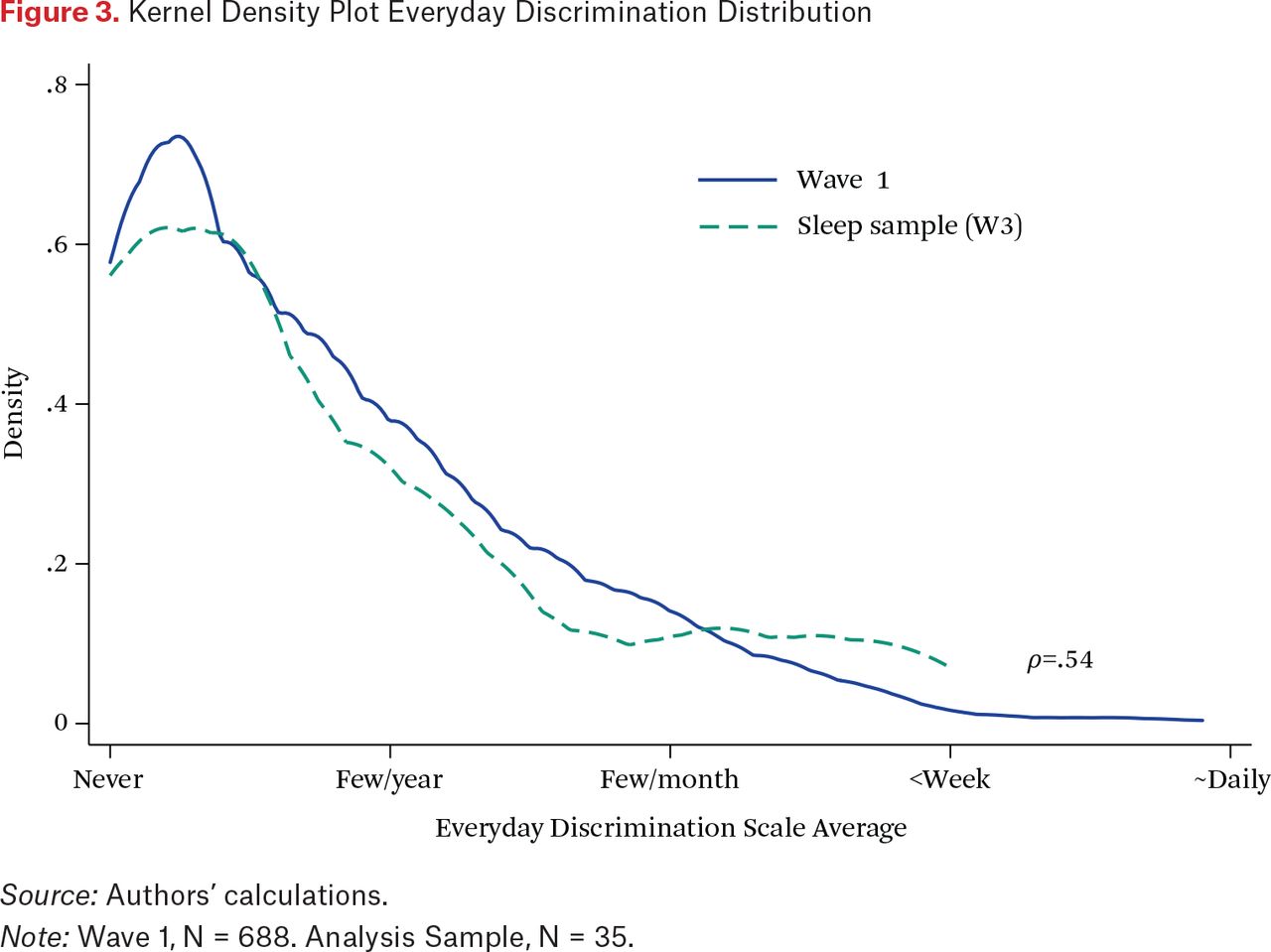
We present a diverse number of sleep measures, including multiple measures of both sleep duration and quality, in this study. Descriptions are presented in table 1 for reference. Example data are presented in figure 2 for illustrative purposes. The lightly shaded sleep period denotes the time in bed and the darker shaded period denotes the time asleep. The top chart in figure 2 shows a highly efficient night of sleep with only short interruptions as indicated by physical movement. The second chart shows much less efficient and poorer sleep with longer periods of disrupted wakefulness and delayed sleep onset. In addition to the actigraphy data, the bottom row of table 1 describes a sleep factor score that was constructed after conducting exploratory factor analysis of the following sleep quality items: sleep efficiency, waking after sleep onset (WASO), average awakening length, movement index, and sleep fragmentation. The scale was then validated using a confirmatory factor analysis to provide an overall sleep quality measure. All sleep measures in the statistical analysis were standardized over the entire sleep distribution to facilitate effect size comparisons.
Description of Sleep Measures
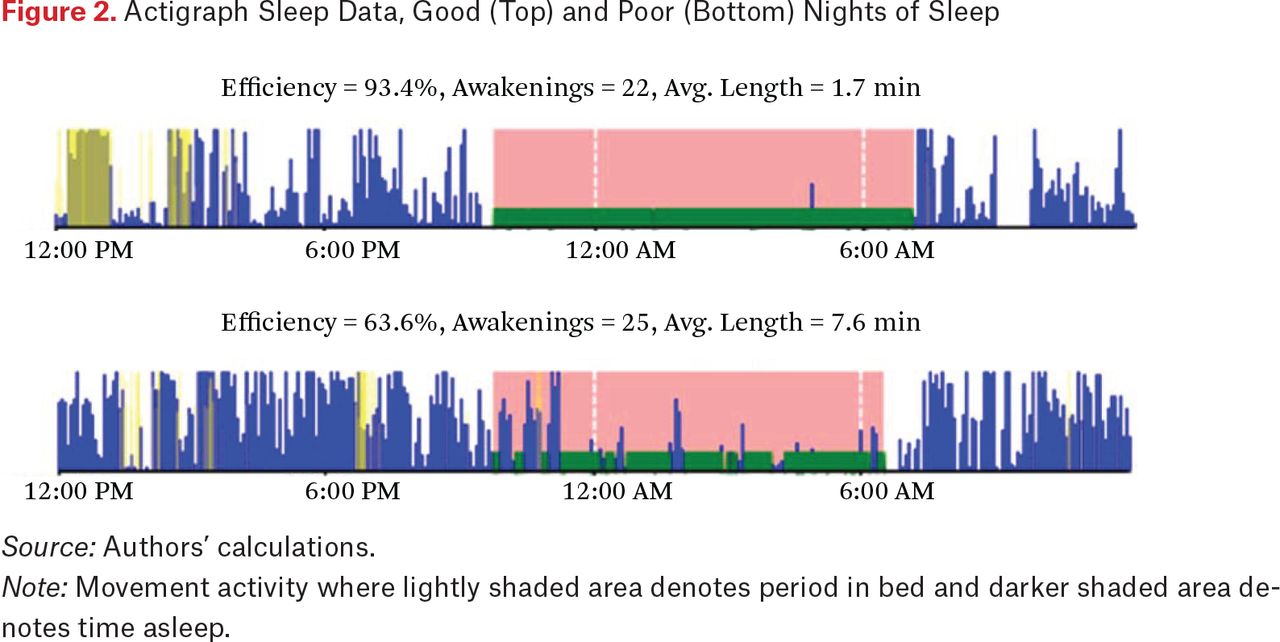
Actigraph Sleep Data, Good (Top) and Poor (Bottom) Nights of Sleep
Discrimination
The key predictor of sleep in this study, measures of discrimination, are operationalized three ways. First, the Williams Everyday Discrimination Scale (EDiS) adapted for adolescents was collected during the initial stage 3 home visit before the actigraphy sleep data was collected (Williams et al. 1997). The EDiS comprised eleven ordinal items categorized from never (0) to almost every day (5). Items were prefaced with the question “In your day-to-day life, how often do you experience the following?” The scale covered a range of social exclusionary and unfair treatment situations that included being treated with less courtesy and less respect, receiving poorer service at restaurants and stores than other people, being insulted or treated poorly by teachers, and being threatened and harassed. Factor loadings were all greater than 0.6 and Cronbach’s = 0.9. The mean was calculated across items and scores were standardized across participants. Importantly, the EDiS is one of the most widely used scales in the area of health disparities research (Paradies 2006). It is also shown to have good reliability, validity, and measurement invariance across African American and white populations (on validity, Benjamins 2012; on measurement, Shariff-Marco et al. 2011; Kim, Sellbom, and Ford 2014). In short, a key advantage of EDiS to measures of, for example, racism-related discrimination is that the EDiS captures discrimination-based social exclusion for a variety of groups, including white respondents.
Next, a series of binary items based on the EDiS were included in the daily e-diaries to indicate whether specific types of mistreatment had occurred over the course of the day. These items captured unfair or poor treatment at school, store, restaurant, or other public space. Five questions measured specific types of mistreatment drawn directly from EDiS, such as “Over the course of the day, did you feel like you were called names or were insulted?” Four additional EDiS items asked whether participants felt that others thought they were not smart, were afraid of them, thought that they were dishonest, and better than them over the course of the day. These items are operationalized as a sum score at the daily level. The third measure is based on the average daily number of experiences, standardized across participants to facilitate comparison with the traditional EDiS instrument.
Controls
Biomarkers from dried blood spots from capillary whole blood were collected during the stage 2 in-lab data collection and were included in the current analyses as controls for potential markers of prior chronic disease risk. Blood spots were assayed for hemoglobin a1c (HbA1c), high sensitivity CRP, and Epstein-Barr virus (EBV) titers. Samples were stored at –20 degree freezer at the University of Nebraska and shipped overnight to the University of Washington Department of Laboratory Medicine for assays (Mark H. Wener, MD, director, Seattle, Washington). Hemoglobin Hba1c, a marker of the percentage average blood glucose over two to three months, is an indicator of diabetes risk, a condition correlated with poor sleep. The raw percentage Hba1c levels of respondents were derived from dried blood from 3.2mm punch disc eluted in a buffer. The raw percentages were converted to the blood equivalent (B-E) value, which is the equivalent of conventional venous liquid blood samples. These values were used in this study and are used to determine cutoffs for normal (< 5.7 percent), prediabetic (5.7–6.4 percent), and diabetic (> = 6.5 percent) range (Potter, UW lab personal correspondence). CRP is a cell-mediated inflammatory marker that is strongly correlated with cardiovascular disease risk. CRP concentrations were also assayed from a 3.2mm punch disc and eluted in a buffer. CRP values converted to serum equivalents using established clinical metrics (for example, NHANES) range from low (< 3 mg/L), elevated (3 < 10 mg/L) to high (10 <) values likely due to acute infection (Pearson et al. 2003). Epstein-Barr antibodies (anti-EBV VCA IgG Ab), whose elevated presence is an indicator stress induced immunosuppression (McClure et al. 2010), were assayed and converted to plasma equivalent values as well. Little is known about its link to sleep. Both CRP and EBV were transformed using a hyperbolic sine transformation that is very similar to a log transformation (Burbidge, Magee, and Robb 1988). All scores were then standardized for use in statistical analyses.
Additional measures include waist-hip ratio from stage 2, standardized across participants to adjust for body size when the biological data were collected (Dalton et al. 2003). From the stage 3 e-diaries, daily somatic complaints as well as the two-week somatic complaint average was calculated from four ordinal items—none (1) to a lot (4)—capturing poor appetite, aches or pains or muscle-joint soreness, being tired for no reason, stomach ache or upset, and headaches. At the daily level, poor self-rated health (five categories, very good to very poor) is included as a standardized measure, along with a standardized person-average over the two-week study period. Finally, all models include an indicator for whether the child was biracial or African American, female, whether the focal parent is married, and whether the family income was greater than $45,000, approximately 250 percent of the state poverty level collected at stage 1 (CFIN 2012). The number and age of children in the household were also included.
Analytic Strategy
The sleep measures comprise the key dependent variables of the analysis and have two key forms of dependency. First, the data are nested within individual participants. For this reason, the basic model is a two-level random-intercept model with each day’s sleep nested within each participant (Raudenbush and Bryk 2002). The daily e-diary measures (discrimination, somatic complaints, SRH) are used to predict sleep that night; the remaining parameters reflect associations with average sleep over the study period. Because the child-means are controlled at the between participant level of the model, the daily measures are orthogonal to the between-subject random intercept and can be interpreted as within-person estimates (Allison 2005). Second, the within-subjects data are neither independent nor exchangeable after accounting for the nesting structure. Rather, an ordered dependency is captured using an autoregressive AR(1) residual structure (Chi and Reinsel 1989).
The models are presented in two ways. First, a between-subjects model including EDiS but not the daily e-diary measures is presented. This model captures the association between sleep and retrospective reports of perceived discrimination in day-to-day life collected during the in-home visit. Second, EDiS is removed from the equation and the daily e-diary discrimination measures and their over-time average are included. The control and biological measures are included in all models reported.1
RESULTS
Descriptive statistics for the sleep variables are presented in table 2 for the total sample, by race and by gender. In general, participants fell asleep within two minutes and with a sleep efficiency rating of approximately 80 percent, which is less than normal healthy sleep efficiency (85 percent). The youth in this sample spent considerable time in bed, nearly (521/60 = ) 8.7 hrs and had a TST of nearly seven hours (413/60), well below the recommended sleep time for this age range of approximately nine hours. The wake after sleep onset averaged around ninety minutes and awakenings per night, of approximately two minutes each, totaled about twenty-three. Differences between groups were minimal other than an indication that biracial and African American youth had more fragmented or restless sleep than white youth, which falls in line with prior literature that finds African Americans have lower average sleep time and more disrupted sleep quality (Hale and Do 2007; Krueger and Friedman 2009).
Descriptive Statistics of Sleep Measures
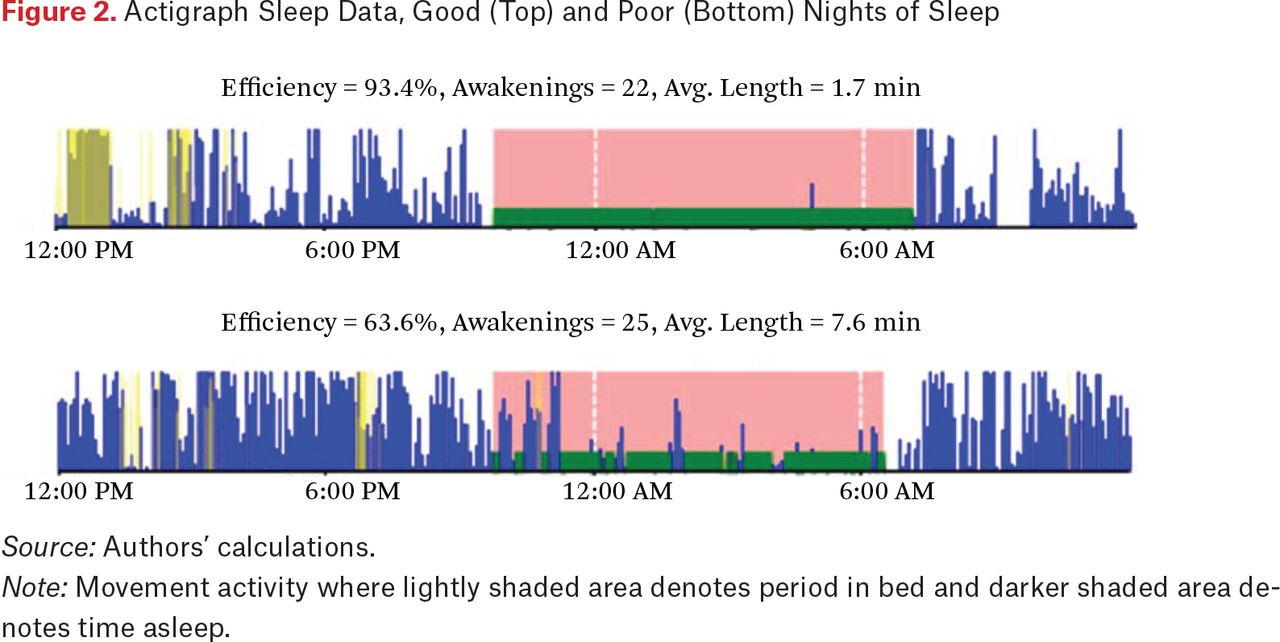
Table 3 presents the descriptive demographic and health characteristics along with averages of both daily and retrospective discrimination levels reported in the sample. The youth in this sample were relatively disadvantaged, about half coming from homes making less than $45,000 per year. Overall, retrospective EDiS average across items was low with the 1-value category reflecting “less than once a year” and the two-value category reflecting “a few times a year.” However, youth reported 0.6 events per day, on average, suggesting that the retrospective EDiS may underreport the amount of discriminatory experiences that young people perceive when the questions are posed more closely in time to those experiences. It is also important that youths’ average retrospective reports of discrimination using the EDiS showed similar average trends to our initial stage 1 sample of youth from which this sample was drawn upon, who reported discrimination (see figure 3). Daily discrimination report counts were higher for biracial or African American youth, but they had fewer somatic complaints. Females reported both more somatic complaints and poorer self-rated health. Both biracial and female youth were more likely to come from disadvantaged families. The biracial youth had lower CRP values, as did females, but biracial and African American youth had higher average Hba1c and EBV antibody levels.
Descriptive Statistics of Predictor Variables

Kernel Density Plot Everyday Discrimination Distribution
Sleep Analysis
A summary sleep analysis using the poor sleep factor score summary measure is presented in table 4. As indicated in table 1, this measure includes an array of highly intercorrelated sleep measures capturing many different features of actigraphy-based sleep assessment. Model A1 includes the home assessment of EDiS (retrospective reports) and model A2 replaces this measure with the daily e-diary reports. Each standard deviation of EDiS (about one point on the ordinal average scale) is associated with a nearly 0.3 standard deviation (p < .01) increase in poor sleep quality. Notably, the EDiS assessment is similar though smaller in magnitude than the two-week accumulation reported in model A2 (b = 0.352, p < .001). Together, these results suggest that the experience or perception of discrimination is positively associated with systematically poorer sleep. Surprisingly, however, the results also suggest that sleep may actually improve during the days when these negative experiences take place (b = –.126, p < .01), in contrast to expectations. Given the nature of this effect, it indicates that youth who experience or perceive more discrimination have poorer average sleep. These youth, however, sleep slightly better on days when those events are reported, but not better overall relative to youth who do not experience such events. Thus, these global sleep findings are consistent with hypotheses 1 but contradict hypothesis 2.
Random Intercept Models, Poor Sleep Factor Score (z)
These models are reproduced in table 5 for sleep latency, overall sleep efficiency, total minutes in bed, and total sleep time. Indications are that, over time, discrimination is associated with increased sleep latency, lower efficiency, and more time in bed with lower TST. Efficiency, in particular is lower (b = 0.3) for those who experience more discrimination, but there are signs of greater sleep efficiency on specific days when discrimination events took place. As before, the daily discrimination measures contradict the hypothesis that negative experiences during the day decrease sleep quality. Instead these results suggest that youth who experience more discrimination generally have poorer sleep, but that sleep recovers relative to personal baseline on days when those experiences take place.
Random Intercept Models, Sleep Latency, Efficiency, Minutes in Bed, and Total Sleep Time
Results for waking from sleep over the night (WASO, awakening frequency, average awakening length) in table 6 and for the sleep indices (movement, fragmentation, sleep fragmentation) in table 7 are consistent with the trends reported in tables 4 and 5. Retrospective EDiS is associated with poorer sleep characteristics and is generally smaller but similar in magnitude to the standardized average of the daily reports. Moreover, on days when discrimination events are reported, youth tend to report better sleep quality as well. Overall, the sleep findings are consistent with hypotheses 1, that discrimination is associated with average sleep quality across a range of sleep measures capturing time in bed. Contradictory to hypothesis 2, however, sleep quality did not decrease on days when discrimination was reported. In fact, signs of a small recovery relative to individual baseline were again evident. Notably, retrospective EDiS scores strongly predicts daily reports (b = 0.70, p < .001; full results not shown, and coefficient is partially standardized with respect to EDiS), suggesting that despite signs of recovery, youth who report discrimination tend to on average have worse sleep. Moreover, the poor sleep factor score on the prior night does not predict daily reports of discrimination (b = –.08, p = .014; results not shown), suggesting that reports of discrimination are not an outcome of poor sleep quality or poor mood (zCESD: b = –.13, p = .164).
Random Intercept Models, Waking, Frequency, Awake Time
Random Intercept Models, Movement, Fragmentation Index, Sleep Fragmentation Index
DISCUSSION
This study examines the links between everyday discrimination, daily variations in discrimination exposure, and objective daily measures of sleep using actigraphy among a diverse sample of adolescents. It contributes to the existing literature documenting the harmful consequences of discrimination for health outcomes by demonstrating the associations between discriminatory and exclusionary experiences for objective daily measures of sleep quality in adolescence. To our knowledge, this is the first study to concurrently measure both retrospective reports of Everyday Discrimination (EDiS) and daily diary reports of discrimination with concurrent objective sleep measures.
The findings support our first hypothesis that average sleep would be linked to discrimination. In fact, average discrimination, operationalized using the retrospective EDiS scale was associated with poorer sleep outcomes across all but two included measures. In general, youth who report more discrimination had shorter sleep duration and poorer sleep quality. Specifically, on indicators of sleep duration, youth who reported discrimination took longer to fall asleep (latency), had less efficient sleep, and spent more time in bed but less time asleep. In terms of sleep quality, youth who reported discrimination had more awakenings after sleep onset, longer duration awake during a sleep disruption, moved more while asleep and had more fragmented sleep. This study falls in line with research using gold standard laboratory techniques finding evidence among adults that discrimination exposure is linked to less time in restorative slow wave sleep (stage 4) (Thomas et al. 2006).
Hypothesis 2 posited that day-to-day variation in perceived discrimination would be adversely associated with sleep variability around the person-average. Thus hypothesis 2 is a within-person hypothesis, suggesting discrimination as a potential source of individual variability in sleep quality. This hypothesis was consistently contradicted by our results, which suggest that contemporaneous exposure is linked to improved sleep efficiency, longer total sleep time, less time awake after sleep onset, and decreased movement and sleep fragmentation. Given that youth more likely to report discrimination having happened over the course of the day are generally more likely to report accumulated everyday discrimination, these results suggest a partial recovery in sleep quality following the negative experience. It is important, however, that despite daily indications of improved sleep on the day of the event, the average sleep duration and quality remain lower in youth who report discriminatory events. In general, around three discriminatory experiences in one day would be required to make up for the average decrease in sleep quality over days across those sleep features given the effect sizes estimated.
In her study measuring discrimination exposure and minority youth psychological well-being, Yip posits that for minority youth who experience discrimination, sleep may in fact be a health coping mechanism that lessens the deleterious impact of discrimination in the short term (2014). Her study finds that youth who experience discrimination and have better daily sleep quality experience higher self-esteem and lower depressive symptoms. It does not, however, contemporaneously measure both daily sleep and discrimination exposure contemporaneously, pointing to the need for more research with larger and more diverse samples using designs similar to those in this study.
An important unmeasured component in this study that may shed light on our surprising results and merits examination is the role of active coping style in the face of social stressors. Sleep is an essential component for healthy adolescent development, yet variations in how coping styles impact sleep or how sleep can be used as a coping tool have yet to be systematically examined. Escape to sleep describes how individuals who have disengaged coping styles may use sleep to regulate exposure to adverse stressful emotions or social conditions. Conversely, individuals who engage in more emotionally focused coping may interpret sleep as a loss of mastery and thus are more prone to heightened arousal and sleep disruption (Sadeh, Keinan, and Daon 2004). Although this study does not include specific measures of coping styles, integrating behavioral and emotional coping among diverse populations is an important direction to take future research in this area.
Despite the novelty of these findings, this study is limited in several important ways. First, although actigraphy provides validated objective measures of sleep quality and duration, validation studies indicate that actigraphs can suffer from low specificity or accuracy when detecting wakefulness, which may affect a number of sleep indices (Sadeh 2011). However, it has been suggested that aggregate data over at least four to five nights can compensate for this issue. This study includes fourteen days of data. Second, the sample size is both small and is based on convenience sample in a single community. Obviously, more powerful samples, and samples constructed using state-of-the-art sampling methodologies are important for better characterizing sleep variability and enhancing generalizability to broader populations. Finally, though racial and ethnic heterogeneity was also low, the racial diversity in this sample is mostly biracial youth with an African American parent, which is novel. More diversity, however, is needed for understanding how the experience of discrimination shapes sleep and health over the early life course.
Overall, discrimination is consistently related to poorer sleep and poor sleep appears to be related to an important long-term health marker already by adolescence. Moreover, supplementary analyses indicated that sleep did not predict discrimination reports the following day, and measures of depressive symptoms did not predict sleep or mediate the discrimination parameters. Taken together, these results support the small but growing literature demonstrating the harmful consequences of discrimination for sleep health and the extensive literature demonstrating the association between discrimination and health risk (Slopen, Lewis, and Williams 2016; Williams 2012).
FOOTNOTES
↵1. We have omitted day of the week from these analyses because inclusion of weekday indicators did meaningfully affect the reported results or inferences. These results are available on request.
Open Access Policy: RSF: The Russell Sage Foundation Journal of the Social Sciences is an open access journal. This article is published under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.
REFERENCES
In this issue









{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.